Article Text

Abstract
Rationale In 2016, a new interferon-gamma release assay (IGRA) was introduced, QuantiFERON-TB Gold Plus (QFT-Plus), claimed to have improved sensitivity in active tuberculosis (TB).
Objectives This study aimed to determine the performance of QFT-Plus, compared with previous generation IGRAs and the tuberculin skin test (TST), in children with TB in Europe.
Methods Multicentre, ambispective cohort study within the Paediatric Tuberculosis Network European Trials Group (ptbnet), a dedicated paediatric TB research network comprising >300 members, capturing TB cases <18 years-of-age diagnosed between January 2009 and December 2019.
Measurements and main results 1001 TB cases from 16 countries were included (mean age (IQR) 5.6 (2.4–12.1) years). QFT-Plus was performed in 358, QFT Gold in-Tube (QFT-GIT) in 600, T-SPOT.TB in 58 and TST in 636 cases. The overall test sensitivities were: QFT-Plus 83.8% (95% CI 80.2% to 87.8%), QFT-GIT 85.5% (95% CI 82.7% to 88.3%), T-SPOT.TB 77.6% (95% CI 66.9% to 88.3%) and TST (cut-off ≥10 mm) 83.3% (95% CI 83.3% to 86.2%). There was a trend for tests to have lower sensitivity in patients with miliary and/or central nervous system (CNS) TB (73.1%, 70.9%, 63.6% and 43.5%, respectively), and in immunocompromised patients (75.0%, 59.6%, 45.5% and 59.1%, respectively).
Conclusions The results indicate that the latest generation IGRA assay, QFT-Plus, does not perform better than previous generation IGRAs or the TST in children with TB disease. Overall, tests performed worse in CNS and miliary TB, and in immunocompromised children. None of the tests evaluated had sufficiently high sensitivity to be used as a rule-out test in children with suspected TB.
- Tuberculosis
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Diagnosing tuberculosis (TB) in children remains challenging, mainly as children typically have paucibacillary disease. Consequently, paediatricians frequently have to rely on immune-based tests, such as the tuberculin skin test (TST) and interferon-gamma release assays (IGRAs), to support a presumptive diagnosis of TB.
WHAT THIS STUDY ADDS
The latest generation IGRA assay, QuantiFERON-TB Gold Plus, does not perform better than previous generation IGRAs or the TST in children with TB disease. Overall, tests performed worse in central nervous system and miliary TB, and in immunocompromised children.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
None of the currently available immune-based diagnostics have sufficiently high sensitivity to be used as a rule-out test in children with suspected TB. More research and funding are needed to develop new diagnostic tests able to define the TB spectrum in children.
Introduction
Paediatric tuberculosis (TB) remains a major global health issue, with at least one million children newly diagnosed with TB each year, representing 12% of all TB cases and resulting in an estimated 230 000 deaths.1 Despite this large disease burden, paediatric TB continues to receive inadequate attention.2
Achieving a definitive TB diagnosis in children is often challenging due to the lack of specific signs and symptoms, difficulties in obtaining sputum samples and the paucibacillary nature of TB in this age group.3 Therefore, detection and treatment of latent TB infection (LTBI) in children to prevent progression to TB disease are key strategies for controlling TB.4 Importantly, the risk of progression is substantially higher in children than in adults, with approximately 30%–40% of infants and 10%–20% of children with LTBI progressing to TB disease within 2 years after primary infection.5
The WHO has pledged to work towards eliminating TB globally by 2035 through the End TB Strategy.6 Accurate diagnostic tests, which can detect both LTBI and TB disease early, are critical in that strategy. Traditionally, the tuberculin skin test (TST) has been used for LTBI diagnosis, and is also used as a supportive diagnostic tool in children with suspected TB disease. However, the TST has a number of well-documented limitations, including suboptimal specificity.7 8 In recent years, newer immune-based diagnostics to detect TB infection have become available for clinical use, of which interferon-gamma release assays (IGRAs) are the most commonly used in high-resource countries.9 Despite early generation IGRAs (ie, QuantiFERON-TB Gold (QFT), QFT Gold in-Tube (QFT-GIT) and T-SPOT.TB) being more specific than the TST, they were found to lack the ability to distinguish between LTBI and TB disease and also to have suboptimal sensitivity in patients with TB disease.10 11
In 2016, the latest generation QFT assay, QFT-Plus (QIAGEN, Germantown, Maryland, USA) was released. In contrast to its immediate predecessor, the QFT-GIT assay, QFT-Plus antigen tubes only contain ESAT-6 and CFP-10 as stimulatory Mycobacterium tuberculosis (MTB) antigens, but not TB7.7. Furthermore, QFT-Plus assays have a newly added second antigen tube (TB2) containing shorter ESAT-6 and CFP-10 peptides, aimed at eliciting CD8+ T cell responses, in addition to the first antigen tube (TB1), which contains longer peptides directed at CD4+ T cells.12
Data in adults suggest that QFT-Plus may have higher sensitivity than QFT-GIT while maintaining high specificity.11 Moreover, the ability to compare CD4 and CD8 responses has been claimed to potentially aid the distinction between TB disease and LTBI.13 However, the existing literature related to QFT-Plus almost exclusively consists of adult studies.14–17 Furthermore, there are no published studies that included paediatric patients from a variety of geographical locations. This is an important limitation since many factors, including nutritional status and immunocompromise, have been shown to impair the performance of previous generation IGRAs in children.18
This study aimed to determine the sensitivity of QFT-Plus assays compared with previous generation IGRAs and the TST in children with both clinically diagnosed and microbiologically confirmed TB disease across a large number of European collaborating centres, and to identify factors that impact on assay performance.
Methods
This ambispective observational multicentre study was conducted by the Paediatric Tuberculosis Network European Trials Group (ptbnet), which currently includes 304 clinicians and researchers based in 31 European countries. The ptbnet database, hosted at Hospital Gregorio Marañón (Madrid, Spain),19 was launched in 2017, capturing data from children and adolescents <18 years of age diagnosed with TB disease at participating healthcare centres. Participating centres are able to enter patients that have received care previously (retrospective arm), as well as newly diagnosed patients (prospective arm); the dataset for each patient is identical, irrespective of whether the patient was included retrospectively or prospectively. The precise time point (between launch of the database on 1 May 2017 and study closure on 31 December 2019) when individual centres started to contribute patients prospectively varied between centres, depending on the timing of institutional and ethical approvals.
TB disease was defined according to established consensus criteria: (1) confirmed TB (microbiological confirmation by culture or PCR) or (2) unconfirmed TB: presence of at least two of the following: (A) symptoms/signs suggestive of TB, (B) chest radiograph consistent with TB, (C) known TB exposure or immunologic evidence of MTB infection and (D) positive response to TB treatment.20 The TB disease focus was categorised as follows: ‘respiratory TB’ comprised individuals with TB disease involving the lung parenchyma, intrathoracic lymph nodes, larynx, trachea, bronchus or pleura without disease elsewhere; ‘miliary and/or central nervous system (CNS) TB’ comprised children with disseminated TB, children with TB meningitis or parenchymal CNS disease, and those who had both; ‘other disease focus’ comprised patients with peripheral lymph node, osteoarticular, genitourinary, abdominal and pericardial TB.
Inclusion criteria
Patients were eligible for inclusion if they were <18 years of age at the time when the diagnosis of TB disease was made, were diagnosed during the above-mentioned time period, received care at one of the participating centres and had undergone at least one IGRA test at the time of diagnosis. Patients not fulfilling all four inclusion criteria were excluded from participation.
Diagnostic tests
QFT-GIT, QFT-Plus and T-SPOT.TB assays were performed in fully-accredited diagnostic laboratories at each participating institution, and results were interpreted according to the version of the manufacturer’s recommendations valid at the time. QFT-GIT and QFT-Plus results were categorised as positive, negative or indeterminate; where available, quantitative background-corrected QFT antigen responses (ie, TB1-nil or TB2-nil result in IU/mL) were also collected. T-SPOT.TB results were classified as positive (≥8 spots), negative or indeterminate. TSTs were performed by intradermal injection of purified protein derivative (RT23; Statens Serum Institut, Copenhagen, Denmark or Tubersol; Sanofi Pasteur, Lyon, France), with results read after 48–72 hours. Considering that the national guidelines of different countries vary in their definition of a positive TST result, only children with available quantitative TST results were included in the analyses related to TST performance; both ≥5 mm (TST5) and ≥10 mm (TST10) cut-offs were evaluated.
Statistical analyses
Categorical variables are reported as absolute frequencies and percentages; continuous variables are reported as median and IQRs. For each test, the test sensitivity was calculated with 95% CI, considering indeterminate IGRA results as negative. Test performance was determined against two gold standards: (1) confirmed and unconfirmed cases combined (ie, the entire study population), and (2) confirmed TB cases only. Wald χ2 test and Fisher’s exact test were used to compare test performances. To account for multiple statistical comparisons, Bonferroni correction was applied. Quantitative background-corrected antigen-stimulated interferon-gamma (IFN-γ) responses in QFT-Plus and QFT-GIT assays among subgroups, stratified by age and TB disease focus, were compared with Kruskal-Wallis tests. Total agreement and Cohen’s kappa coefficient (k) were used to quantify concordance between TST and IGRA results; indeterminate IGRA results were excluded from this particular analysis. All analyses were done with SPSS (V.25; IBM SPSS Statistics: Armonk, NY, USA) and NCSS2020 (NCSS Statistical Software, Kaysville, UT, USA). Figures were constructed with Prism (GraphPad Software, San Diego, CA, USA).
Results
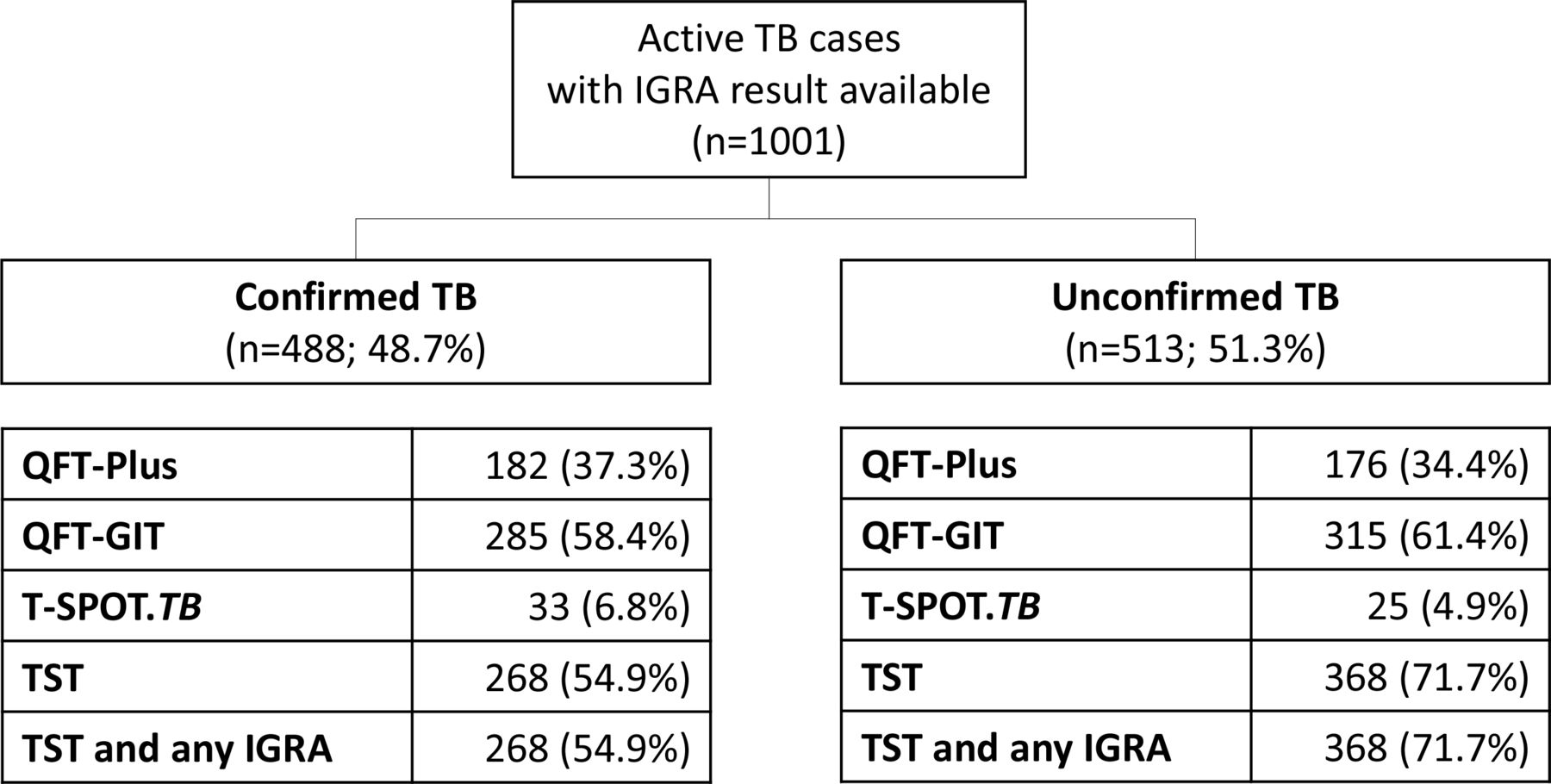
A total of 1001 children and adolescents were included in the final analysis (figure 1). The median (IQR) age was 5.6 (2.4–12.1) years. Cases were contributed from participating healthcare centres located in 16 European countries: Spain (n=399), Italy (n=311), Germany (n=87), Turkey (n=32), United Kingdom (n=23), Latvia (n=22), Greece (n=21), Portugal (n=21), Bulgaria (n=20), Russia (n=19), Switzerland (n=15), Ukraine (n=15), Lithuania (n=7), Sweden (n=4), Croatia (n=3) and Austria (n=2). The demographic details of the study population are summarised in table 1. Overall, 488 (48.8%) patients were classified as confirmed TB, and 513 (51.2%) as unconfirmed TB. Of the children with confirmed TB in whom all microbiological test results were available (n=435), 329 (75.6%) had positive MTB culture results and 300 (69.0%) had positive PCR results (n=194 both MTB culture-positive and PCR-positive). Approximately half (50.5%) had a history of TB contact (46.5% in the confirmed TB group vs 54.2% in the unconfirmed TB group, p=0.009). One hundred and thirty-six (13.6%) children had pre-existing comorbidities (online supplemental material table E1). Of those, eight had HIV coinfection, 20 were receiving immunosuppressive treatment, and 49 had other immune disorders. The most common disease manifestation was respiratory TB (table 1).
Supplemental material

Flow chart summarising the composition of the study population and the type and number of tests performed in study participants with confirmed and unconfirmed TB. IGRA, interferon-gamma release assay; QFT-GIT, QuantiFERON-TB Gold in-Tube; QFT-Plus, QuantiFERON-TB Gold Plus; TB, tuberculosis; TST, tuberculin skin test.
Baseline characteristics of the 1001 children included in the study
A QFT-Plus was performed in 358 cases (35.7%), QFT-GIT in 600 cases (59.9%), and T-SPOT.TB assay in 58 cases (5.8%). In 636 cases a quantitative TST result was available. A large proportion of children underwent more than one test: 375 (37.5%) QFT-GIT and TST, 224 (22.4%) QFT-Plus and TST, 29 (2.9%) T-SPOT.TB and TST, 5 (0.5%) QFT-GIT and T-SPOT.TB, 2 (0.2%) QFT-Plus and T-SPOT.TB and 6 (0.8%) QFT-GIT, T-SPOT.TB and TST.
Comparative performance of TST and IGRA assays
In the entire cohort, the overall sensitivity of the IGRAs and the TST at the 10 mm cut-off did not differ significantly: QFT-Plus 83.8% (95% CI 80.2% to 87.8%), QFT-GIT 85.5% (95% CI 82.7% to 88.3%), T-SPOT.TB 77.6% (95% CI 66.9% to 88.3%), TST10 83.3% (95% CI 80.4% to 86.2%). However, TST5 had significantly higher sensitivity than all three IGRAs in the entire cohort (89.9% (95% CI 87.6% to 92.3%)). Table 2 shows a summary of the performance of each test in defined subgroups, based on demographics, disease focus and pre-existing comorbidities. There was no significant difference between the sensitivities of QFT-Plus and QFT-GIT in any of the subgroups analysed. While TST10 had lower sensitivity than QFT-Plus and QFT-GIT in patients with miliary TB and/or CNS TB, there was no significant difference observed between TST5 and both IGRAs in this subgroup. TST5 showed higher sensitivity than QFT-Plus in children aged 1–5 years, and higher sensitivity than all three IGRAs in patients with ‘other TB’.
Summary of the test performance of interferon-gamma release assays and the tuberculin skin test (at ≥10 mm and ≥5 mm cut-offs) in children with tuberculosis according to demographics, confirmation status and clinical characteristics
All four tests showed lower sensitivity in the subgroups of children with miliary and/or CNS TB (QFT-Plus: 73.1%; QFT-GIT: 70.9%; T-SPOT.TB: 63.6%; TST10: 43.5%; TST5: 67.4%) and in immunocompromised children (QFT-Plus: 75.0%; QFT-GIT: 59.6%; T-SPOT.TB: 45.5%; TST10: 59.1%; TST5: 68.5%) compared with test sensitivity in the entire study population (QFT-Plus: 83.8%; QFT-GIT: 85.5%; T-SPOT.TB: 77.6%; TST10 83.3%; TST5: 89.9%).
Online supplemental material table E2 shows additional data in children with microbiologically-confirmed TB only, which are broadly consistent with the data shown in table 2. None of the subgroup analyses showed a difference between the performance of QFT-Plus and QFT-GIT.
Table 3, which summarises further comparisons of defined subgroups according to disease focus, shows that TST5, TST10 and QFT-GIT had significantly lower sensitivity in patients with miliary and/or CNS TB than in patients with pulmonary TB.
Comparison of the test sensitivities of interferon-gamma release assays and the tuberculin skin test (at ≥5 mm and ≥10 mm cut-offs) stratified by disease focus
Online supplemental material table E3 shows additional data related to the performance of TSTs and IGRAs in different ethnic groups. In TST5 and TST10, the lowest sensitivity was observed in children with Hispanic/Latino background; additional analyses revealed that the sensitivity of TST5 and TST10 was significantly lower in this ethnic group than in Caucasian children (p=0.0009 and p<0.0005, respectively).
Online supplemental material table E4 shows a comparison of the retrospective and the prospective study arms. The additional analyses did not reveal any significant differences in the sensitivity of the investigated IGRAs (QFT-Plus, QFT-GIT and T-SPOT.TB) between both arms. However, despite overlapping CIs, statistically the sensitivity of TST5 and TST10 was higher in the retrospective arm (TST5: 93.1% (95% CI 89.7% to 95.6%) vs 86.8% (95% CI 82.%6 to 90.3%); TST10: 87.1% (95% CI 82.8% to 90.5%) vs 79.6% (95% CI 74.8% to 83.9%)).
Indeterminate IGRA results
Eleven (3.1%) of 358 patients who underwent QFT-Plus had an indeterminate test result, universally due to inadequate IFN-γ responses in the positive control. Twenty-one (3.5%) of 600 patients had an indeterminate QFT-GIT result, and 5 (8.6%) of 58 patients had an indeterminate T-SPOT.TB result.
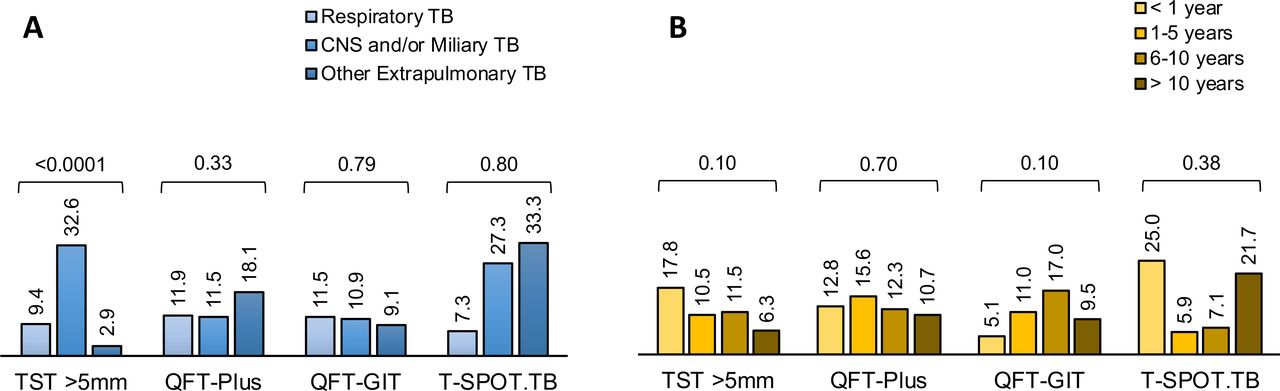
The rate of indeterminate results was considerably higher in patients with miliary and/or CNS TB, compared with patients with respiratory TB and those with ‘other focus’, both for QFT-Plus (p=0.017) and QFT-GIT (p<0.0001), while this was not observed in T-SPOT.TB (figure 2A). Comparing indeterminate results across age groups (figure 2B), there was no statistically significant variation observed in any of the IGRAs. However, in children <1 year of age, the proportion of indeterminate results was substantially higher in QFT-GIT (5/59; 8.5%) than in QFT-Plus (1/39; 2.6%). Online supplemental material table E5 shows the proportions of indeterminate test results in confirmed and unconfirmed cases, as well as in immunocompromised and non-immunocompromised patients.

Proportion of indeterminate interferon-gamma release assay results according to assay and site of disease (A) and age group (B). Figures shown are percentages and p values calculated with Fisher’s exact tests. CNS, central nervous system; QFT-GIT, QuantiFERON-TB Gold in-Tube; QFT-Plus, QuantiFERON-TB Gold Plus; TB, tuberculosis.
Negative IGRA and TST results
The proportion of negative test results did not vary substantially between the tests evaluated (table 4). A substantial proportion of patients with negative test results—varying between 36.1% and 75.0% between the tests—had microbiologically-confirmed TB, showing that those results were truly false-negative. Only a small proportion (5/47; 10.6%) of patients with negative QFT-Plus result were known to be immunocompromised, which may have accounted for the false-negative results in those particular patients (table 4).
Details regarding negative test results according to test in the entire study population
Figure 3 shows comparisons of the proportion of negative test results according to site of disease and age for each test. TST5 showed significantly higher rates of negative results in children with miliary and/or CNS TB (p<0.0001), while the proportion of negative results in the IGRAs did not differ significantly between disease sites. Similarly, the proportion of negative test results did not vary significantly between age groups, although TST5 showed a trend of decreasing rates of negative results with increasing age (p>0.05). Online supplemental material table E5 shows that in all evaluated tests negative results were more common in immunocompromised than in patients without immune compromise.

Summary of negative tuberculin skin test and interferon-gamma release assay results according to site of disease (A) and age group (B). Figures shown are percentages and p values calculated with Fisher’s exact tests. CNS, central nervous system; QFT-GIT, QuantiFERON-TB Gold in-Tube; QFT-Plus, QuantiFERON-TB Gold Plus; TB, tuberculosis; TST, tuberculin skin test.
Quantitative TST and IGRA responses
Quantitative results were available for 272 QFT-GIT (45.3%) and for 281 QFT-Plus (78.5%) assays. Figure 4 shows quantitative TST results and background-corrected antigen responses in both QFT assays across different age groups. While no significant variation in the magnitude of IFN-γ responses was observed across the age groups in QFT-GIT, both QFT-Plus TB1 and TB2 responses varied significantly, with the highest median values being observed in children 1–5 years of age.

Violin plot of the quantitative results of the TST (A), the single antigen-stimulated sample of the QFT-GIT assay (B), and both antigen-stimulated samples of the QFT-Plus assay (TB1 (C) and TB2 (D)) according to age groups. All QFT-GIT and QFT-Plus data shown are background-corrected (ie, interferon-gamma concentration in the antigen-stimulated sample minus interferon-gamma concentration in the nil sample). The horizontal lines indicate median and IQRs; p values were calculated with Kruskal Wallis tests. QFT-GIT, QuantiFERON-TB Gold in-Tube; QFT-Plus, QuantiFERON-TB Gold Plus; TB, tuberculosis; TST, tuberculin skin test. *statistically significant.
Figure 5 shows TST indurations and background-corrected antigen responses in QFT-GIT and QFT-Plus assays according to the site of disease. In all three tests, quantitative responses were lower in patients with miliary and/or CNS TB than in patients with pulmonary TB or ‘other focus’.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Violin plot of the quantitative results of the TST (A), the single antigen-stimulated sample of the QFT-GIT assay (B), and both antigen-stimulated samples of the QFT-Plus assay (TB1 (C) and TB2 (D)) according to disease site. All QFT-GIT and QFT-Plus data shown are background-corrected (ie, interferon-gamma concentration in the antigen-stimulated sample minus interferon-gamma concentration in the nil sample). The horizontal lines indicate median and IQRs; p values were calculated with Kruskal Wallis tests. CNS, central nervous system; QFT-GIT, QuantiFERON-TB Gold in-Tube; QFT-Plus, QuantiFERON-TB Gold Plus; TB, tuberculosis; TST, tuberculin skin test. *statistically significant.
Comparisons between IGRA and TST responses
Details regarding the correlation between categorical TST results (TST5 and TST10), and the test results of the three IGRAs are shown in online supplemental material table E6. Result concordance between TST and IGRA results was similar for all three IGRAs and overall higher with TST5, ranging from 87.3% (QFT-Plus) over 87.6% (QFT-GIT) to 88.6% (T-SPOT.TB). QFT-Plus had higher agreement with TST5 (Cohen’s k=0.462) than QFT-GIT and T-SPOT.TB (Cohen’s k=0.343 and k=0.271, respectively).
Discussion
To our knowledge, this is the first multinational multicentre study investigating the diagnostic accuracy of QFT-Plus in comparison with other IGRA assays and the TST in children with TB disease, which was facilitated by the inclusion of a large number of participating centres across Europe via a well-established collaborative paediatric TB research network.
Our data show that all immune-based tests evaluated in this study have insufficient sensitivity to be used as rule-out tests in children with suspected TB disease. Notably, the overall sensitivity of 83.8% of QFT-Plus assays observed in our study is substantially below the sensitivity thresholds suggested by the WHO target product profiles for new TB diagnostics (TB screening tests: optimal requirement >95%/ minimal requirement >90% sensitivity).21 Contrary to previous claims, our data indicate that QFT-Plus assays do not have greater sensitivity than previous generation IGRAs or the long-established TST. This was not only the case in the study population as a whole, but also in several subgroups analysed, stratified by gender, age and disease focus. However, it is possible that the number of patients with QFT Plus assay results was insufficient to detect minor gains in diagnostic sensitivity.
The large majority of published studies evaluating QFT-Plus have been done in adults, and a large proportion of those have focused on LTBI, rather than evaluating the assay in patients with TB disease.17 22 Of the studies that featured adults with TB disease, most included fewer than 100 TB patients, which limits the precision of the reported performance estimates.17 23 24 A recent meta-analysis on QFT-Plus in adults, which included 578 TB cases reported by six studies, estimated the assay sensitivity in adults with TB disease to be between 90% and 98%.16 To our knowledge, only six studies evaluating the performance of QFT-Plus in children with TB disease have been published so far,14–16 25–27 with the first four including fewer than 60 paediatric TB cases combined. The currently largest paediatric study, which was conducted in Spain and included 158 paediatric patients with TB disease (46.8% microbiologically-confirmed), reported a substantially lower sensitivity estimate (82.9% (95% CI 77.0% to 88.8%)) than most adult studies.14 Those data are consistent with our sensitivity estimate of 83.8% (95% CI 80.2% to 87.8%) in a far larger paediatric study population recruited from 16 European countries. Another study from the same group, which also included children with suspected TB who ultimately had alternative diagnoses, found that QFT-Plus assays had a specificity, sensitivity, positive predictive value and negative predictive value of 91.5%, 87.3%, 86.4% and 91.2%, respectively.26
We also found that there was a tendency for tests evaluated in our study to perform worse in patients with miliary and/or CNS TB, as well as in immunocompromised children. The former is concordant with the results of a recent study on TB meningitis in children from our network, which reported test sensitivities of 71.7% and 82.5% for QFT and T-SPOT.TB assays, respectively, highlighting that up to one in four children with CNS TB have false-negative IGRA results.28 The poor performance of IGRAs in patients with disseminated TB has previously been reported in adult patients, with one study reporting the sensitivity of the QFT-GIT in adults with miliary TB to be as low as 68%.29 The tendency for all four evaluated tests to perform worse in immunocompromised children is to be expected, considering that both the TST and IGRAs are based on the detection of functional immune responses directed against mycobacterial antigens. This observation also aligns with previous publications that have reported impaired IGRA performance in children with HIV infection and primary immunodeficiencies.18
Another key finding was that, overall, IGRAs performed similarly across all age groups, including in children <12 months of age, traditionally considered to be a group at higher risk of indeterminate assay results.11 16 18 However, on average quantitative IFN-γ responses in the QFT-Plus assay, both in TB1 and TB2 tubes, were lower in this particular age group than in the older age groups. Interestingly, in TST5 false-negative results were almost three times as common in children <12 months-of-age than in children >10 years-of-age (17.8% vs 6.3%), although this was not statistically significant. Also, the proportion of indeterminate QFT-GIT results in children <1 year was higher than in the older age groups, but this did not reach statistical significance.
Finally, our results highlight that there is an ongoing need to identify better immunological biomarkers (other than IFN-γ) that enable the development of improved immunodiagnostic TB tests for children.30–32 Promising biomarkers that have recently been described include mycobacteria-specific cytokine responses that have better performance characteristics than IFN-γ and may simultaneously facilitate the distinction between LTBI and TB disease, as well as polyfunctional MTB-specific T cells and MTB-specific antibody profiling.30 33–36
Our study has several limitations. First, the study was predominately retrospective, which may have introduced some selection bias. Second, only one IGRA was performed in the majority of cases, precluding head-to-head comparisons in individual patients. However, such direct comparisons are rarely performed in paediatric studies due to the large blood volume required for duplicate IGRAs. In some instances, the same individuals were included in estimates of different test sensitivities, which limits our interpretation of independent effects between assays. Third, our study did not include children with LTBI or patients with suspected TB who were subsequently diagnosed with another condition, thereby precluding estimates regarding test specificity. Lastly, although our study included a large cohort of children from Western and Eastern Europe, children from the latter were less represented, mainly due to limited use of IGRAs in that region. However, a key strength of this study is the inclusion of a very large number of children with TB disease, enhancing the precision of our sensitivity estimates, and the involvement of a large number of study sites in different geographical locations, making the results generalisable to routine paediatric practice. However, additional data are needed in children with malnutrition and those living with HIV infection.
In conclusion, our study shows that IGRAs, including the last generation QFT-Plus assay, have suboptimal sensitivity in children and adolescents with TB disease, particularly those with miliary and/or CNS TB and those with underlying immunocompromise, precluding their use as a rule-out test. QFT-Plus did not show greater sensitivity than previous generation IGRAs or the TST in our study population overall, as well as well-defined subgroups thereof. In light of our results, and considering the difficulty in obtaining microbiological confirmation of TB in children, the development of new immunodiagnostic tests that perform robustly across all age groups, ideally with the ability to distinguish between LTBI and TB disease, remains a key priority if the WHO TB elimination goals are to be achieved.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was reviewed and approved by the ptbnet Steering Committee, and the Human Research Ethics Committee of the Fondazione Policlinico Universitario A. Gemelli IRCCS of Rome, Italy (prot 29213/19, ID 2555). The study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments. No personal or identifiable data were collected during the conduct of this study. Written informed consent was obtained from the parents/guardians of children prospectively enrolled into the study; depending on local regulations, informed assent was additionally obtained from children above 12 years of age.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DB and AN-J are joint first authors.
Twitter @surf4children, @tonisoriano66
Correction notice This article has been corrected since it was published Online First. Changes have been made to some affiliations and the funding statement. Minor changes have also been applied to the tables and text.
Collaborators Laura Minguell (Hospital Universitari Arnau de Vilanova. Lleida, Spain), Estrella Peromingo (Department of Paediatrics, Hospital Universitario Puerta del Mar, Cádiz, Spain), David Gomez Pastrana (Department of Paediatrics, Hospital Universitario de Jerez, Jerez de la Frontera, Spain), Tomas Pérez-Porcuna (Unitat de Salut Internacional, Departament de Pediatria, Fundació Recerca Mútua Terrassa, Atenció Primària, Hospital Universitari Mútua de Terrassa, Universitat de Barcelona, Terrassa, Spain), Beatriz Soto (Hospital Universitario de Getafe, Madrid, Spain), Elena Colino Gil (Department of Paediatrics, Complejo Hospitalario Universitario Insular Materno—Infantil de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain), Mercedes Herranz-Aguirre (Sección de Enfermedades Infecciosas Pediátricas, Servicio de Pediatría, Complejo Hospitalario de Navarra, Pamplona, Spain), Cesar Gavilan Martin (Servicio de Pediatría, Hospital Universitario San Juan de Alicante, Spain), Eva María López-Medina (Pediatric infectious Disease Unit, Hospital Universitario y Politécnico La Fe, Valencia, Spain), Christine Bell (Central Manchester University Hospitals NHS Foundation Trust, Manchester, UK), Frances Child (Royal Manchester Children’s Hospital, UK), Inga Ivaškevičienė (Clinic of Children’s Diseases, Institute of Clinical Medicine, Vilnius University, Vilnius, Lithuania), Zulema Lobato (Department of Paediatrics, Hospital Sant Joan de Déu—Fundació Althaia, Manresa, Spain), Neus Rius (Hospital Universitari Sant Joan de Reus, Spain), Olga Calavia (Department of Paediatrics, Hospital Joan XXIII, Tarragona, Spain), Daniel Blázquez-Gamero (Pediatric Infectious Diseases Unit, Hospital Universitario 12 de Octubre, Madrid, Spain), Begoña Carazo (Pediatric Infectious Diseases Unit, Pediatrics Department, Hospital Materno Infantil de Málaga, Málaga, Spain), Maria Queralt Soler Campins (Department of Paediatrics, Consorci Sanitari de Terrassa, Terrassa, Spain), Cristina Calvo (Pediatric and Infectious Diseases Department Hospital Universitario La Paz, Madrid, Spain), Javier Korta Murua (Department of Paediatrics, Hospital Universitario Donostia, San Sebastián, Spain), Charlotte Buxbaum (Astrid Lindgren Children’s Hospital, Karolinska University Hospital Huddinge, Stockholm, Sweden), Ivan Pavić (Department of Paediatric Allergology, Pulmonology, Rheumatology and Clinical Immunology, Children’s Hospital Zagreb, Zagreb, Croatia), Cristina Alvarez (Department of Paediatrics, Hospital Universitario Marqués de Valdecillas, Santander, Spain), Elvira Cobo-Vazquez (Hospital Universitario Fundación de Alcorcón, Madrid, Spain), Beatriz Perez Gorricho (Pediatric Infectious Diseases Unit, Department of Pediatrics, Hospital Infantil Universitario Niño Jesús, Madrid, Spain), Sonia Rodriguez (Hospital Universitario Príncipe de Asturias, Alcalá de Henares, Spain), Ana Menasalvas (Department of Paediatrics, Hospital Virgen de la Arrixaca, Murcia, Spain), Maria Isabel Garrote Llanos (Pediatric Infectious Diseases Department, Hospital Universitario de Basurto, Bilbao, Spain), Sara Berhard-Stirnemann (Department of Paediatrics, Cantonal Hospital Aarau Children’s Hospital, Aarau, Switzerland), Marie Rohr (Department of Paediatrics, Hôpitaux Universitaires de Genève, Geneva, Switzerland), Christa Relly (Division of Infectious Diseases and Hospital Epidemiology, University Children’s Hospital Zurich, Zurich, Switzerland), Lourdes Garcia Rodriguez (Pediatria, Hospital de Mataró—Consorci Sanitari del Maresme, Barcelona, Spain), Maria del Pozo (Pediatrics Department, Hospital General Universitario de Albacete, Albacete, Spain), Irene Rivero-Calle (Translational Pediatrics and Infectious Diseases Section, Hospital Clínico Universitario de Santiago de Compostela, Spain), Alfredo Tagarro (Pediatrics Department, Hospital Universitario Infanta Sofía, San Sebastián de los Reyes, Madrid, Spain), Andrea Duppenthaler (Department of Paediatrics, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland), Isabelle Rochat Guignard (Service of Paediatrics, Department of Woman, Mother, Child, Lausanne University Hospital, University of Lausanne, Lausanne, Switzerland), Michael Buettcher (Paediatric Infectious Diseases, Department of Paediatrics, Lucerne Children’s Hospital, Switzerland), Elizabeth Whittaker (Section of Paediatric Infectious Diseases, Imperial College, London, UK), Paddy McMaster (Department of Paediatric Infectious Diseases, Northern Care Alliance NHS Group, Manchester, UK), Verdiana Vigliano (Catholic University of Rome, Italy), Cristina Russo (Bambino Gesù Children Hospital, Rome, Italy).
Contributors DB, MT, BS-G, AN-J conceptualised the study, wrote the first draft and the last version of the manuscript. All authors contributed to methodology, data collection, revision of initial draft and final version of the manuscript. MT and BS-G are joint last authors. DB is the author acting as guarantor.
Funding AN-J was supported by “Subvencions per a la Intensificació de Facultatius Especialistes” (Departament de Salut de la Generalitat de Catalunya, Programa PERIS 2016-2020) [SLT008/18/00193]. AHL is funded by the Spanish Ministry of Science and Innovation—Instituto de Salud Carlos III and Fondos FEDER (Contrato Río Hortega CM20/00128).
Competing interests DB participated in a Qiagen advisory board meeting on the use of IGRAs in children <5 years of age. The manufacturers had no influence on the study design, data collection, analysis or interpretation, writing of the manuscript or the decision to submit the data for publication. BS-G and MT have received support from Cepheid for a project on molecular TB diagnostics unrelated to the study reported here. MT has received QuantiFERON-TB assays at reduced pricing or free of charge for TB diagnostics projects from the manufacturer (Cellestis/Qiagen) in the past, and has received support for conference attendance from Cepheid.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.