Article Text

Abstract
Background The incremental long-term prognostic value of high-sensitivity C-reactive protein (hsCRP) above troponin in a large real-world cohort of unselected patients presenting with suspected acute coronary syndromes (ACS) is unknown. We hypothesised that a mildly elevated hsCRP is associated with mortality risk in patients with suspected ACS, independent of troponin level.
Methods We used the National Institute for Health Research Health Informatics Collaborative data of 257,948 patients who had a troponin measured at 5 cardiac centres. We excluded patients with clinically abnormal white cell counts and hsCRP >15 mg/L to try limiting the population to those without overt infections, malignancies or systemic inflammatory conditions that may confound our analyses. Patients were divided into four hsCRP groups (<2, 2–4.9, 5–9.9 and 10–15 mg/L) and the association between hsCRP levels and all-cause mortality assessed.
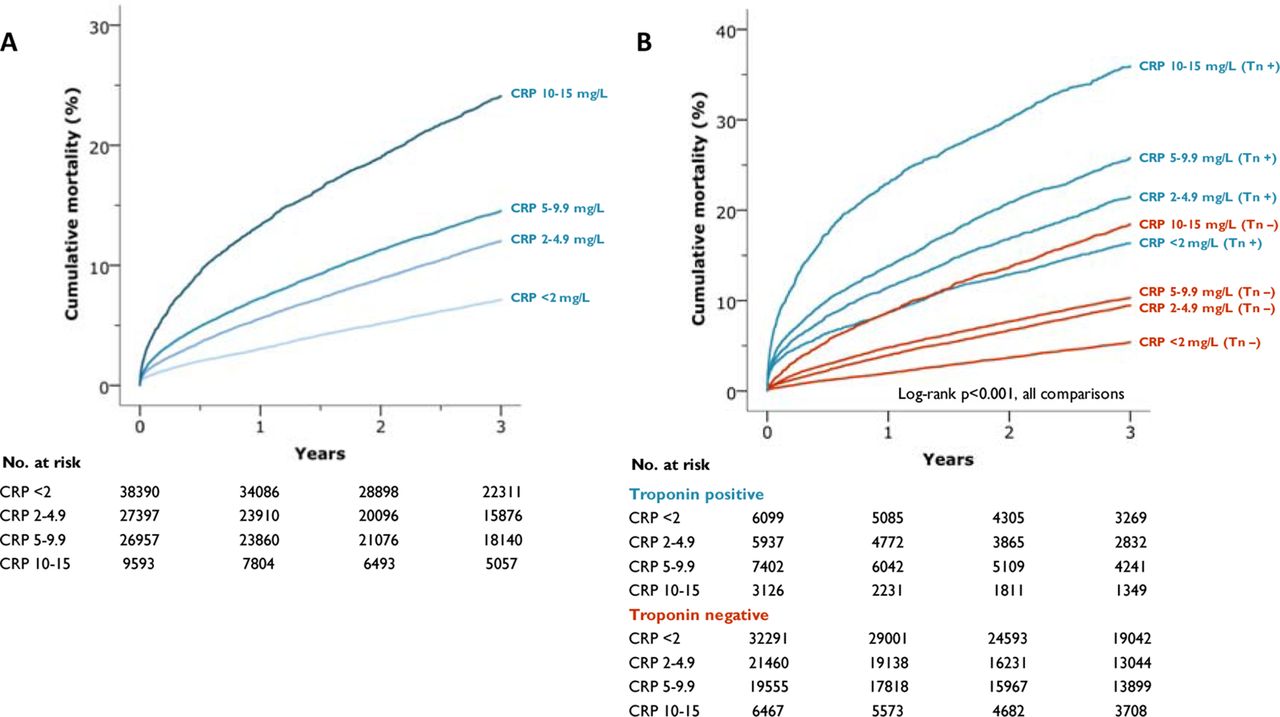
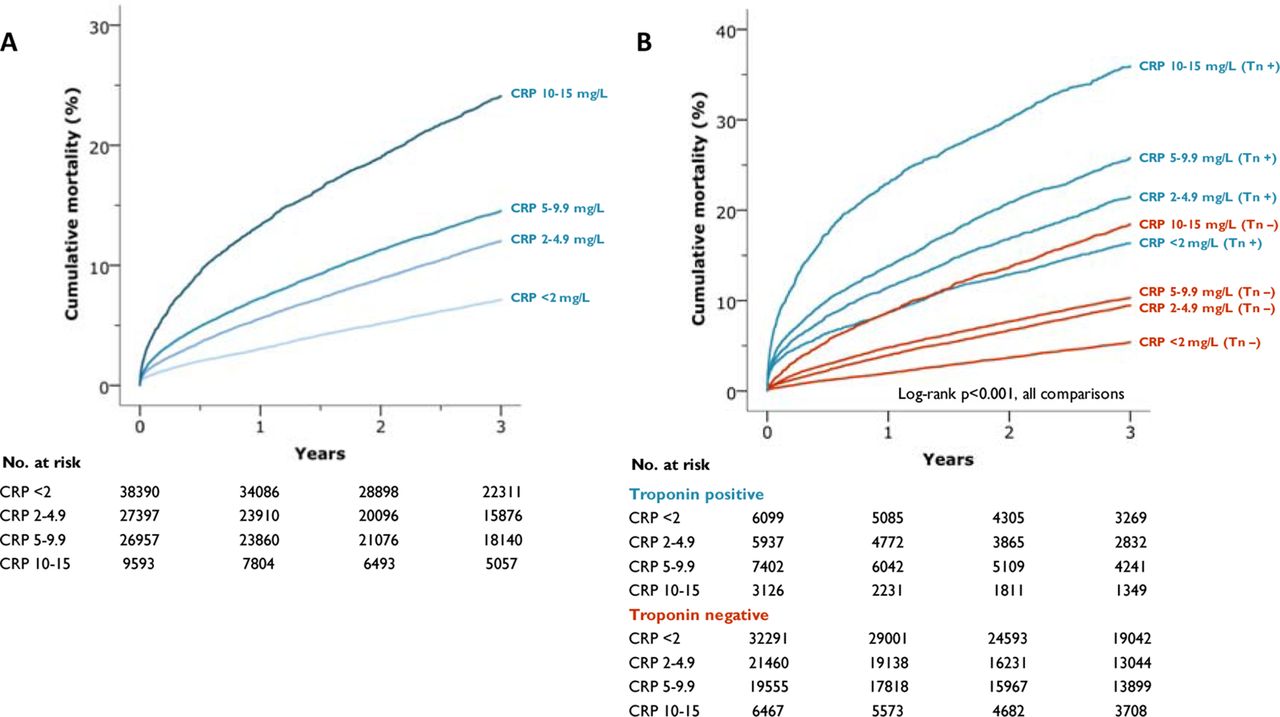
Results There were 102,337 patients included in the analysis (hsCRP <2 mg/L (n=38,390), 2–4.9 mg/L (n=27,397), 5–9.9 mg/L (n=26,957) and 10–15 mg/L (n=9,593)). figure 1A displays cumulative mortality per hsCRP group, revealing increasing mortality with each consecutive group. figure 1B further stratifies the groups according to dichotomised peak troponin level as positive or negative. This shows the greatest mortality for patients in the highest hsCRP group who also had a positive troponin assay (36.0% at 3 years).
In Cox regression analysis with time-dependent covariates, even mildly raised hsCRP was an independent predictor of mortality over time, after adjusting for age, gender, haemoglobin, white cell count, platelet count, creatinine and troponin positivity. There was a positive and graded relationship between hsCRP level and mortality at baseline, which remained at 3-years (hazard ratio (95% CI) of 1.32 (1.18–1.48) for those with hsCRP 2.0–4.9mg/L, and 1.40 (1.26–1.57), and 2.00 (1.75–2.28) for those with hsCRP 5–9.9 mg/L and 10–15 mg/L, respectively.
We explored whether inclusion of hsCRP could better reclassify the population into at-risk mortality groups. The association with 30-day, 1-year and 3-year mortality was assessed using three different risk models (model 1: age, gender, haemoglobin, creatinine; model 2: model 1 plus troponin (positivity versus negativity); model 3: model 2 plus hsCRP groups. For cumulative mortality at each time point, each successive model was better able to discriminate risk than its precursor (p<0.0001); such that inclusion of troponin and hsCRP gave the most robust risk discrimination. Model 3 achieved an AUROC >0.8 at 30 days, 1-year and 3-year mortality, surpassing the use of troponin on its own.
{kind=link}
Kaplan-Meier mortality curve by (A) hsCRP level and (B) hsCRP level and troponin positivity
Conclusion These multi-centre, real-world data from a large cohort of patients with suspected ACS identify hsCRP as a clinically meaningful prognostic marker in addition to troponin levels and point to its potential utility in selecting patients for novel treatments targeting inflammation.
Conflict of Interest No conflicts of interest