Article Text

Abstract
Objectives To examine relationships between fitness, physical activity and psychosocial problems among English secondary school pupils and to explore how components of physically active lifestyles are associated with mental health and well-being.
Methods A total of 7385 participants aged 11–13 took a fitness test and completed self-reported measures of physical activity, attitudes to activity, psychosocial problems and self-esteem during the Fit to Study trial. Multilevel regression, which modelled school-level cluster effects, estimated relationships between activity, fitness and psychosocial problems; canonical correlation analysis (CCA) explored modes of covariation between active lifestyle and mental health variables. Models were adjusted for covariates of sex, free school meal status, age, and time and location of assessments.
Results Higher fitness was linked with fewer internalising problems (β=−0.23; 95% CI −0.26 to −0.21; p<0.001). More activity was also related to fewer internalising symptoms (β=−0.24; 95% CI −0.27 to −0.20; p<0.001); the relationship between activity and internalising problems was significantly stronger for boys than for girls. Fitness and activity were also favourably related to externalising symptoms, with smaller effect sizes. One significant CCA mode, with a canonical correlation of 0.52 (p=0.001), was characterised high cross-loadings for positive attitudes to activity (0.46) and habitual activity (0.42) among lifestyle variables; and for physical and global self-esteem (0.47 and 0.42) among mental health variables.
Conclusion Model-based and data-driven analysis methods indicate fitness as well as physical activity are linked to adolescent mental health. If effect direction is established, fitness monitoring could complement physical activity measurement when tracking public health.
- Adolescent
- Physical fitness
- Physical activity
- Well-being
- Mental
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
The youth inactivity crisis, and poor adolescent mental health, are pressing public health challenges. Only 22% of boys and 15% of girls achieve the daily hour of moderate-to-vigorous physical activity (MVPA) recommended by the WHO,1 2 and up to one in five young people will experience mental ill-health3: half of all disorders are established by age 14.4
Regular physical activity has a positive impact on mental health, but the relationship is complex and not fully understood.5 Poor mental health has numerous causes including biological, psychological and social-environmental factors, such as social and economic deprivation6: the benefits of exercise for mental health may depend on how individuals experience activity, and the context in which it takes place.7 In adolescent clinical samples, aerobic exercise programmes can treat depression and improve self-esteem, which can protect against the onset of disorders.8 9 In the general adolescent population, evidence of links between physical activity and mental health, while promising, is inconclusive.10 Studies involving large community samples have found variously that vigorous activity is unrelated to anxiety and depression but linked with better social functioning11; MVPA is associated with lower (but not clinically meaningful) levels of depression and anxiety, and greater well-being12; MVPA is linked to fewer emotional and peer-related problems in primary school children but more conduct and hyperactivity-inattention difficulties13; and meeting daily MVPA guidelines is related to fewer global psychosocial problems at clinically meaningful levels.14 Girls and boys appear to respond differently: more peer and emotional problems have been linked with lower activity among boys, but not girls.13
Cardiorespiratory fitness (CRF) is a modifiable risk factor linked to current and future physical health among adolescents, independent of physical activity.15–17 Much less is known about the role of CRF in adolescent mental health,18 although it has been linked to a reduced incidence of depression in young people, potentially via better brain health.15 19 Research linking fitness and psychosocial problems in community samples are sparse: two very recent studies found small but significant negative associations between fitness and psychosocial problems: the relationship was stronger among girls than boys.20 21
Evidence linking fitness and mental health would support calls to extend paediatric public health surveillance to include measures of both fitness and physical activity.22 23 Fitness tests linked to peak oxygen consumption provide objective, clearly defined measures capturing long-term active lifestyles, whereas accelerometry or self-report measures of physical activity provide 7-day snapshots influenced by circumstances, activity type and recall bias.24 Fitness also has potential to capture the interplay of other factors linked to mental health, including obesity.25
Understanding more about relationships between activity, fitness and mental health in young adolescents is therefore important. Our objectives in this study were to examine associations between psychosocial problems and physical activity, and, separately, psychosocial problems and CRF in a community sample of adolescents. Because evidence suggests these relationships might differ between girls and boys, and because deprivation can impact mental health, we also wished to explore whether associations vary with sex and socioeconomic status. Given the complex relationship between activity, fitness, contextual factors and mental health, we also used a data-driven approach to explore whether physically active lifestyles, including positive attitudes towards regular physical activity leading to higher fitness, are associated with good mental health, characterised by few psychosocial problems and positive self-esteem.
METHOD
Design
The study was a cross-sectional analysis of baseline data from the Fit to Study cluster-randomised controlled trial, registered with ClinicalTrials.gov, NCT03286725. Trial recruitment, methodology and consent procedures are reported elsewhere26 in line with the Consolidated Standards for Reporting Trials (CONSORT).
Participants
Baseline assessments of pupils aged 11–13 from British state secondary schools took place between June and September 2017, at the end of Year 7 and the start of Year 8. Schools provided participants’ sex, birth date and their eligibility for free school meals (eFSM), an indicator of socioeconomic disadvantage. The full sample recruited at baseline was n=16 017; male=7056; eFSM=3068.
Outcome measures
Cardiorespiratory fitness was assessed during school physical education (PE) lessons with the 20 m Multistage Fitness Test,27 validated in numerous studies.28 Scores were number of laps completed: pupils scoring at or above normative 50th percentile scores for boys and girls aged 12 were considered fit.29
Physical activity (past week) was measured with a validated, single-item measure.30 Participants reporting at least 60 min’ MVPA for each of the past 7 days were considered active; all others were inactive. Habitual physical activity (past 6 months) was measured with a single self-report item.31 In line with established methods,32 attitude to physical activity was the mean score of three items on a visual analogue scale (boring–fun; stressful–relaxing; dissatisfying–satisfying). Higher scores indicate better outcomes.
Psychosocial problems were measured with the Strengths and Difficulties Questionnaire (SDQ),33 valid and reliable in children aged over 1134 consisting of 25 items measuring five subscales: conduct problems, hyperactivity–inattention, peer–relationship problems, emotional symptoms and pro-social behaviour. We used combined conduct and hyperactivity scores (externalising) and peer and emotional scores (internalising) as primary outcome measures for model-based analyses because there is evidence that in low-risk samples, the more focused subscales might not tap into distinct aspects of mental health.35 We interpreted internalising scores ≥9 and externalising scores ≥11 as high/very high.35
Self-esteem was measured with the global and physical self-esteem subscales of the short Physical Self Description Questionnaire, validated for use among adolescents and typically used in PE contexts; higher scores indicate better outcomes.36 Cronbach’s alpha is reported for scales and subscales in table 1.
Cronbach’s alphas for psychosocial variables
Statistical analyses
Primary analyses included participants who completed all outcome measures. For secondary analyses, we used the full sample available at baseline imputing missing data to account for potential bias. Secondary analyses based on multiple imputations are reported in online supplemental material.
Supplemental material
Categorical analyses by sex and eFSM
The odds of scoring in the high/very high or typical category for internalising and externalising problems and the odds of being active (7 days) or fit (≥50th percentile score) by sex and eFSM status were calculated using multilevel logistic regression, controlling for school clusters.
Model-based analyses
We used multilevel linear regression, with random intercepts to account for school clusters, to explore associations between fitness, physical activity and internalising and externalising problems. Because assessments took place in both PE and form classes, we did not include random intercepts for class clusters. Data were z-scored to facilitate comparisons within and between models. The distribution of internalising and externalising scores was positively skewed: we applied a square-root transformation and a rank inverse normal transformation, respectively, to these data. We developed four separate models, with internalising and then externalising scores as outcome variables, and physical activity and then fitness as predictor variables. Then, using forced entry, we fitted four adjusted models, including fixed effects for sex, eFSM and their interaction terms, and age and nuisance covariates, which were term of fitness assessment, term of questionnaire assessment and location of questionnaire assessment. Where interactions were non-significant, we removed these terms and re-ran the model. Where significant interactions with sex and/or eFSM were present (p<0.0125; Bonferroni-corrected for four comparisons), we explored these by plotting their slopes. We obtained crude parameter estimates by developing unadjusted models with data that was transformed but not standardised. Analyses were conducted in R with the lme4 package.37
Reverse transformations
To derive an approximate value for change in internalising and externalising scores associated with a one-lap increase in fitness score and an additional day per week of activity, we multiplied the transformed estimates in each model by the SD of the distribution on the original scale.
Data-driven analysis of associations
We used canonical correlation analysis (CCA)—an approach which measures associations between two sets of variables, making no prior assumptions about relationships—to explore modes of covariation between physically active lifestyles and mental health. The active lifestyle variables were measures of activity, fitness, habitual activity and attitude to activity. The mental health variables were the conduct, hyperactivity, peer, emotional and pro-social sub-scales from the SDQ; global self-esteem and physical self-esteem. The CCA maximised the strength of correlation (Rc ) between a linear combination of active lifestyle measures and a linear combination of mental health metrics. For every covariation mode, we characterised the canonical cross-loading or the degree of influence that each variable exerted on its opposite canonical variate (Rs ). Better mental health would be indicated by negative Rs values for psychosocial problems and positive values for self-esteem. We took the mean squared error (MSE) as an estimate of the accuracy of the match between predicted and actual data sets. For significant CCA modes, we calculated the redundancy index or the amount of variance in one group of variables explained by the other group. Significance of CCA modes was assessed through permutations38; analyses were conducted using Matlab canoncor.
Patient and public involvement
Teachers advised on the feasibility of data collection, administered fitness tests and supervised questionnaire completion. Schools received trial progress reports. Teachers were invited to attend academic conferences.
RESULTS
After data cleaning, 7385 participants (female=4441; 60.1%; eFSM=1044; 14.1%) from 67 schools completed the questionnaire and fitness test (online supplemental material figure 1); 95.5% answered the questionnaire and 85.4% took the fitness test before the summer vacation; 93.8% completed the survey in school. Mean age at the start of the school year was 12.5 (SD 0.29) years. Mean scores on each variable and percentages in each category stratified by sex and eFSM status are presented in table 2.
Mean (SD) participant scores on all outcome variables (n=7385)
High internalising scores were significantly associated with sex but not eFSM: odds of a high score were 1.6 times greater for girls (table 3). The odds of high externalising scores were lower for girls and higher for disadvantaged pupils. The odds of being active daily were higher for boys but not for disadvantaged pupils. The odds of meeting or exceeding normative fitness levels were lower for eFSM pupils, but there was no significant difference between sexes.
ORs of psychosocial problems, activity and fitness by sex and disadvantage
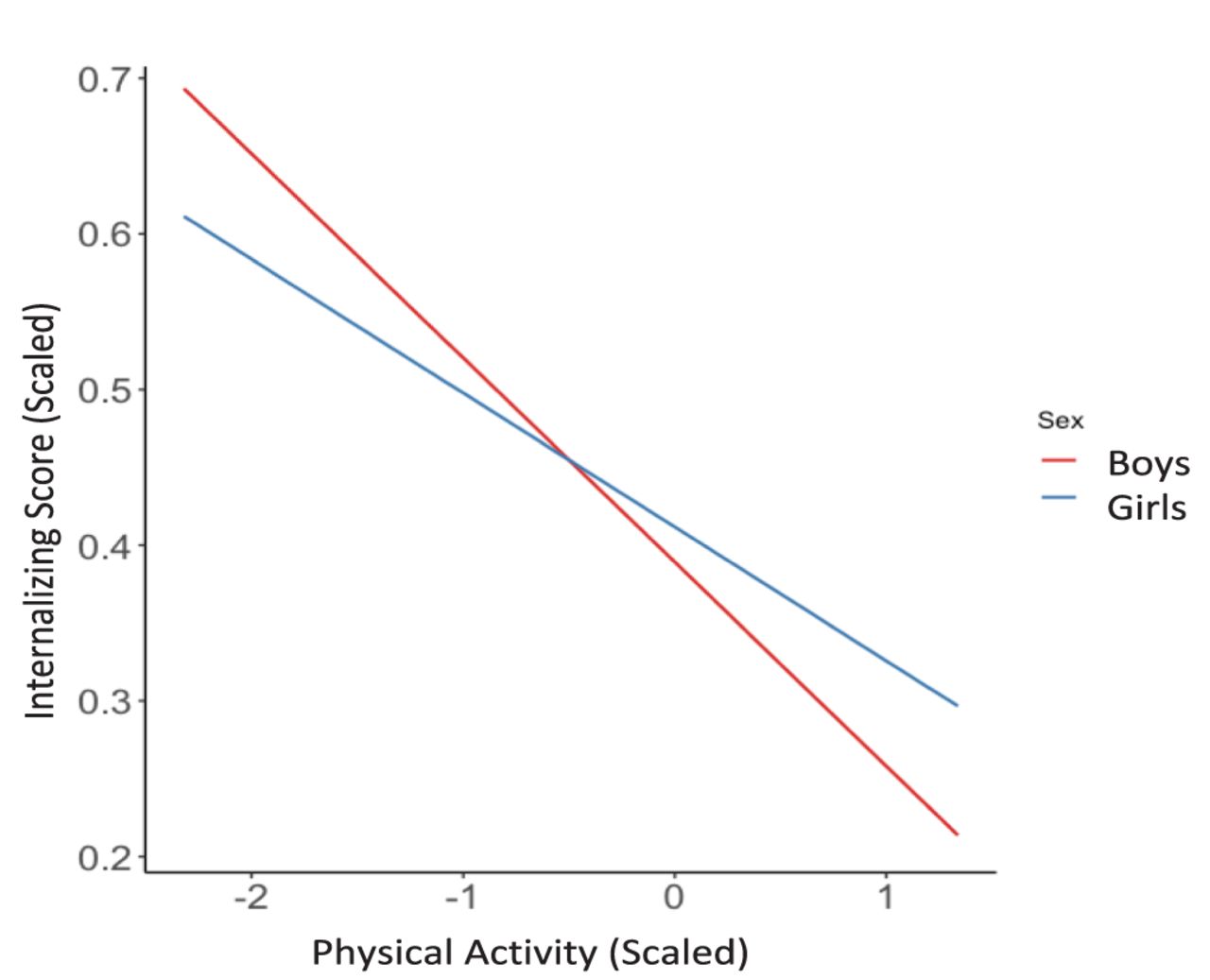
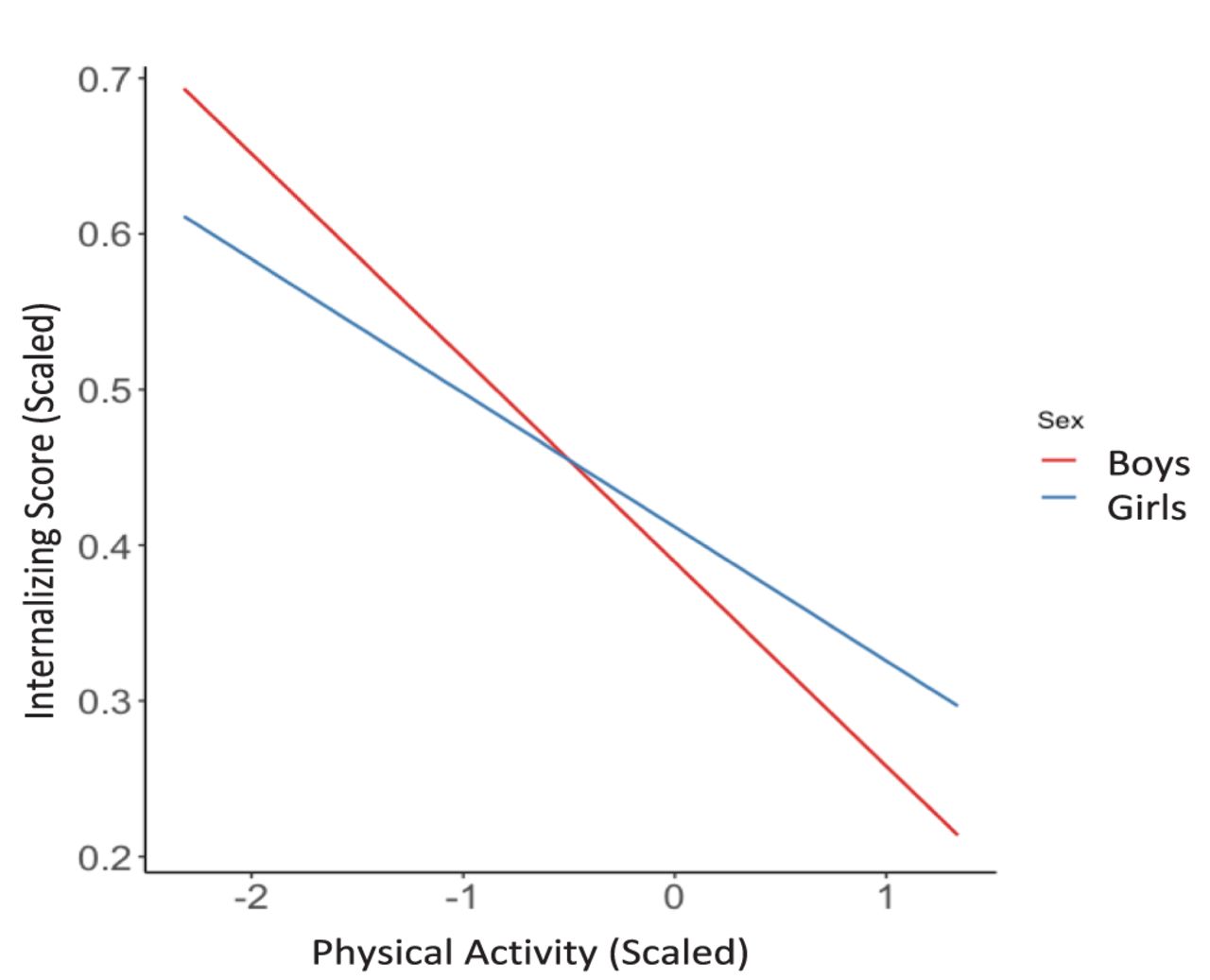
Models 1 and 2 examined internalising symptoms and their relationship with physical activity and fitness, respectively (table 4). There was a significant effect of sex on the relationship between internalising symptoms and activity: the favourable relationship was stronger for boys than girls (β=0.07; 95% CI 0.03 to 0.12; p<0.001). More activity was significantly associated with fewer internalising symptoms (β=−0.24; 95% CI−0.27 to −0.20; p<0.001). Figure 1 plots the interaction of physical activity and sex: for every unit increase in activity, boys showed a significantly larger reduction in internalising symptoms.
Estimates of associations between physical activity, fitness, internalising and externalising symptoms (n=7385)
Fully adjusted multilevel model including age, sex, eFSM, nuisance covariates and school effects; physical activity and internalising scores are z-scored; internalising symptoms are square-root transformed to account for positively skewed distribution.
Higher fitness was significantly related to fewer internalising symptoms (β=−0.23; 95% CI −0.26 to −0.21; p<0.001). There were no significant interactions between fitness and either sex or eFSM at the p=0.0125 threshold. School effects explained 2.8% of variance in internalising symptoms in both models. Model 1 explained 6.2% of variance in internalising symptoms over and above school effects, while Model 2 explained 7.3%.
Models 3 and 4 (table 3) examined externalising symptoms and their relationship with physical activity and fitness, respectively. More activity was significantly related to fewer externalising symptoms (β=−0.09; 95% CI −0.11 to −0.06; p<0.001). There were no significant interactions between sex, eFSM and activity. Higher fitness is significantly associated with fewer externalising symptoms (β=−0.07; 95% CI −0.09 to −0.04; p=0.002). There was no significant interaction of sex or eFSM at the p=0.0125 threshold.
School effects explained 3.0% of variance in externalising symptoms. Model 3 explained 3.1% of variance in externalising symptoms over and above school effects, while Model 4 explained 2.9%.
Reverse-transforming estimates for physical activity and fitness showed an extra day per week of physical activity is linked to internalising and externalising scores that are lower by 0.85 and 0.20, respectively. An additional lap on the fitness test is associated with internalising and externalising scores that are lower by 0.77 and 0.18.
In the full-imputed dataset, fitness and physical activity were significantly related to both internalising and externalising symptoms (p<0.001) but estimates were larger for fitness than for activity (online supplemental file). In the externalising models, estimates for fitness and physical activity were approximately twice the magnitude of those based on complete cases only. School effects explained similar variance in internalising and externalising symptoms.
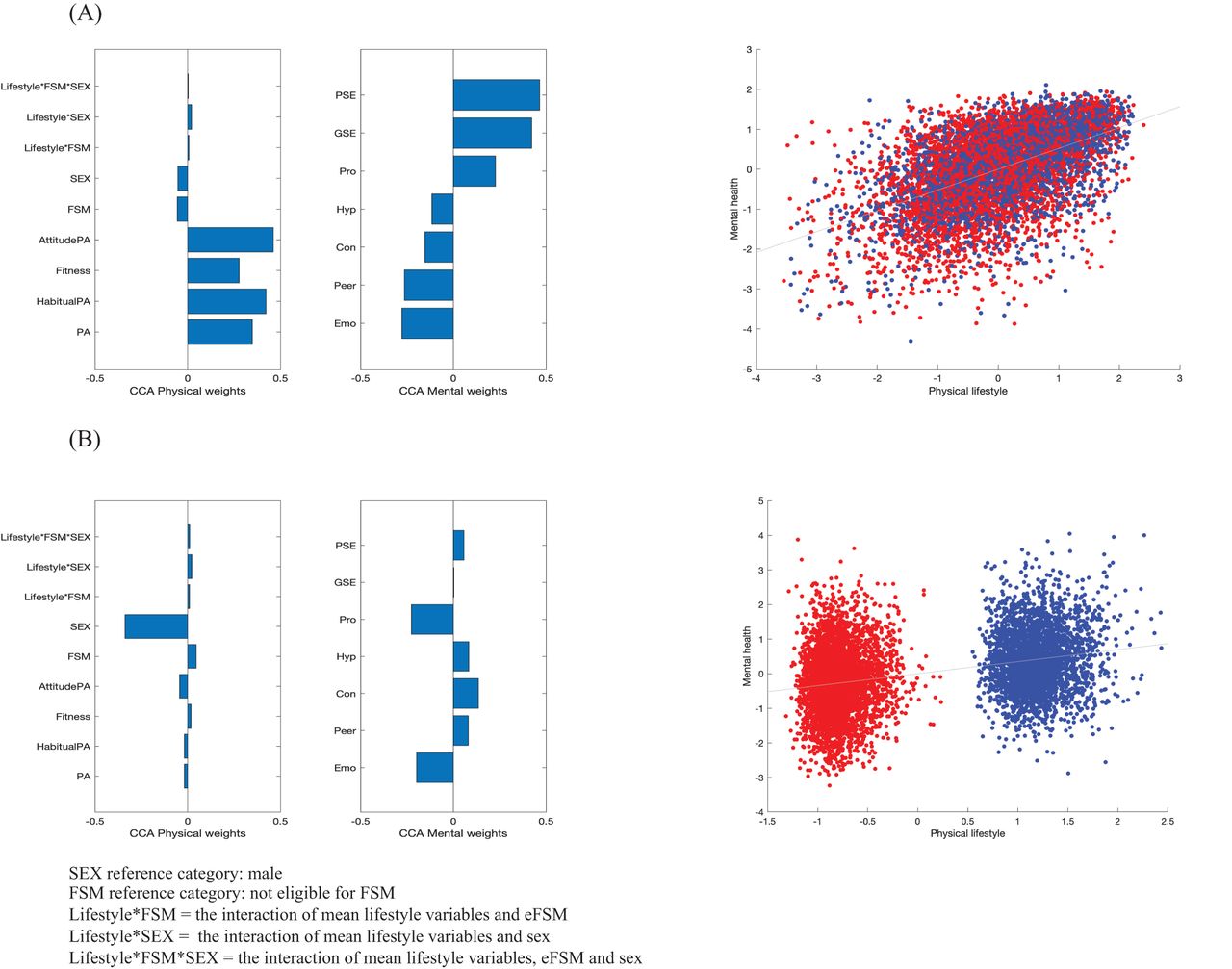
CCA identified two statistically significant and meaningful modes of covariation between physically active lifestyle and mental health factors. The first mode, (Rc =0.52, MSE=0.99, p=0.001), was characterised by high cross-loadings for positive attitudes to MVPA (Rs =0.46) and habitual activity (Rs =0.42) in the active-lifestyle variate, and physical self-esteem (Rs =0.47) and global self-esteem (Rs =0.42) in the mental health variate. Figure 2A presents variables’ cross-loadings (online supplemental file gives associated numerical data). In this mode, both physical activity (Rs =0.35) and fitness (Rs =0.28) were influential. Low levels of internalising difficulties (emotional Rs =−0.28 and peer Rs =−0.26) had higher cross-loadings than low externalising difficulties (conduct Rs =−0.15 and hyperactivity Rs =−0.12). The scatter plot shows a canonical correlation between lifestyle and mental health for both boys (blue) and girls (red).
{kind=link}
{kind=link}
(A) Canonical cross-loading of variables onto their respective variates in mode 1. (B) Canonical cross-loading of variables onto their respective variates in mode 2.
In the second mode (Rc =0.34, MSE=2.60, p=0.001), described in figure 2B (and online supplemental file), sex had high cross-loadings in the lifestyle variables (Rs =−0.34) while pro-social behaviour (Rs =−0.23) and emotional difficulties (Rs =−0.20) were prominent across mental health variables. The scatterplot showed a clear difference between girls (red) and boys (blue): girls have a different pattern of mental health to boys, with higher predicted scores for both pro-social behaviour and emotional difficulties.
The redundancy index, or the amount of explained variance, was 8% for active lifestyle variables given mental health variables and 11% for the mental health set given the active lifestyle set.
DISCUSSION
We believe this is the first study to show a significant relationship between CRF and mental health in a community sample of young British adolescents. Higher fitness, and more days per week of activity, are both associated with fewer psychosocial problems in this group. The relationship between activity and internalising symptoms was stronger for boys than for girls, but none of the other relationships we explored varied significantly with either sex or socioeconomic status. A physically active lifestyle is linked to better mental health: positive attitudes towards activity, and habitual activity, are important features of the relationship, together with positive self-esteem. These are important findings because they suggest that fitness assessments could complement the physical activity measures that are essential for public health monitoring.
Comparisons with other studies
Our results add to the sparse research linking fitness and psychosocial problems in the adolescent population. We found a significant relationship with both internalising and externalising problems after controlling for sex, although the effect size was larger for internalising symptoms. This aligns with previous research: a recent Canadian study found a small favourable association between CRF and internalising problems, but only among girls,20 while an Australian study of older adolescents found the link between internalising symptoms and fitness was significantly stronger among girls.21 Neither found a relationship with externalising symptoms.
Our findings that physical activity is favourably related to internalising and externalising symptoms supports previous research and strengthens the evidence of a favourable link between activity and mental health in the adolescent population.
Nevertheless, the range of measures and confounding variables under consideration make effect size comparisons difficult. In our study, the relationship between activity and internalising symptoms was stronger for boys, which aligns with previous findings that more peer and emotional problems have been linked with lower activity among boys, but not girls.13
We believe this is the first data-driven CCA to show that physically active lifestyles are linked to good mental health. Activity-positive attitudes and habitual activity were important features of the relationship, together with positive self-esteem, which can protect against onset of disorders.39 Our findings are supported by previous research highlighting favourable links between activity and physical self-esteem.40 A second mode of covariation revealed an association between sex and mental health: being female was linked to more pro-social behaviour but also more emotional difficulties, in line with UK norms.41
Possible explanations and implications
Physical activity, fitness and mental health are thought to be linked through several distinct mechanisms. CRF may promote stress resilience by optimising neuroendocrine and physiological responses to physical and also psychosocial stressors.42 Fitness may also contribute to improved mood via enhanced brain plasticity and growth factor expression.43 Separately, physical activity is thought to enhance mood and protect against depression. But these relationships appear to be bi-directional: cohort studies show that higher internalising scores, especially among boys, predict lower activity levels during adolescence.13
While our findings cannot prove causal relationships, our research indicates that interventions to boost fitness as well as activity, and promote positive attitudes to such behaviour, might have potential to reduce emotional and peer-related problems in particular among early adolescents from all socio-economic backgrounds, and especially boys. This is important, given that half of all disorders appear by age 14.4
The variance in psychosocial problems explained by our models (which include sex and eFSM status, and control for school effects, age and nuisance variables) is less than 10% in all cases. But unlike other hypothesised causes of poor mental health in this age group, such as genetic predisposition or social-environmental circumstances, low fitness and activity are particularly good targets for interventions in community settings, including schools.44 Previous studies have attempted to establish whether membership of a broad physical activity category—being ‘inactive’ or ‘active daily’ for example—has a clinically meaningful impact on psychosocial problems, sometimes defined as a one-point change in the Total Difficulties Score, which is the sum of internalising and externalising scores.12–14 We found that an extra day of activity and an extra lap on the fitness test is linked with internalising scores that are lower by approximately 0.8 and externalising scores by around 0.2. Such a difference might be critical for individuals at high risk of a clinical disorder, at the margin between slightly raised and high scores. Furthermore, there is growing support for a population approach to adolescent mental health that promotes well-being and healthy behaviours among all young people45: such an approach would aim to shift the entire distribution rather than targeting individuals at key cut-off points on the curve.
One potential explanation for the closer link that activity and fitness have with internalising symptoms is that regular activity offers an outlet for adolescents with hyperactivity-inattention and conduct problems: these challenging behaviours are sometimes associated with higher movement rather than the inverse.46 The relationship between female sex and mental health could explain why the favourable relationship between activity and internalising symptoms appears stronger for boys: overall, girls had greater odds of high internalising scores, and female sex, independent of activity and fitness levels, was associated with high emotional difficulties in one mode of covariation between active lifestyle and mental health.
Strengths and limitations
A key strength is the use of complementary univariate and multivariate analysis approaches to explore links between activity and mental health. Analyses revealed similar patterns of associations: in particular, activity and fitness are more strongly associated with internalising (peer and emotional) problems than with externalising (conduct and hyperactivity) symptoms. We accounted for potential sample bias by imputing missing data: secondary analyses showed favourable relationships between fitness, physical activity and mental health were robust.
Limitations were that we did not collect additional information about the intensity, duration or context of physical activity behaviour, or about sedentary behaviour. Although the multistage fitness test is a reliable and valid measure,47 PE lessons can be a sub-optimal testing environment. We used single-item self-report measures of physical activity and, although we adjusted regression models for a range of confounding factors, we acknowledge more may be present. Considering the context of activity—and inactivity—could deepen our understanding of how it relates to mental health: for example, team sport has been linked to good mental health48 while screen-based sedentary behaviour is associated with depressive symptoms.49 Cronbach’s alpha for the peer, conduct and pro-social subscales of the SDQ was <0.7, in line with evidence that, in community samples, these more focused scales might not reliably capture distinct aspects of mental health.35
Recommendations for future studies
Our design does not support conclusions about causality: the Fit to Study cluster-randomised controlled trial26 aims to establish causation. Future studies could explore the role of muscular fitness, and measure relationships between mental health and physical activity in different contexts, including leisure time and competition.
CONCLUSION
Fitness as well as physical activity is associated with fewer adolescent psychosocial problems. Fitness assessments could complement the physical activity measures that are essential for public health monitoring. A physically active lifestyle is linked with better overall mental health during early adolescence, a period of rapid developmental change when disorders are becoming established. Further evidence of effect direction is needed.
What are the new findings
Cardiorespiratory fitness, as well as physical activity, is linked to adolescent mental health.
Fitness is more strongly associated with internalising than externalising symptoms of psychological distress.
Physically active lifestyles incorporating positive attitudes to activity are linked to better mental health, characterised by higher self-esteem and fewer internalising problems.
How might findings impact practice in the future
Paediatric public health surveillance could include measures of fitness as well as physical activity.
Interventions targeting adolescent fitness could be tested for effects on both mental and physical health.
Acknowledgments
We thank the Fit to Study Investigators (URL: https://www.fit-to-study.org/investigators/), for helping plan and deliver the Fit to Study trial and particularly Emma Eldridge, Emily Curtis, Oliver Bushnell and Emily Plester. Thanks to Catharine Creswell, Lucy Bowes, Alan Stein, Kathryn Atherton and Josh de Leeuw for their advice. The authors are grateful to the teachers and pupils at participating schools for their time.
REFERENCES
Footnotes
Contributors HJ-B and HD conceived the study. CW, TW and NB acquired the data. TW, PS, TN, HJ-B and CW analysed and interpreted the data. CW drafted the manuscript. All authors critically reviewed the manuscript for important intellectual content and approved the final version for publication.
Funding This work was supported by the Education Endowment Foundation and The Wellcome Trust’s Education and Neuroscience Programme [grant number 2681]. HJ-B is funded by the Wellcome Trust (110027/Z/15/Z) and the NIHR Oxford Biomedical Research Centre. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z). HD is supported by the Elizabeth Casson Trust and the NIHR Oxford Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Ethics approval Central University Research Ethics Committee of the University of Oxford (R48879).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The authors agree to share anonymised data upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.