Article Text

Abstract
Antimicrobial resistance is a growing problem worldwide. Encouraging antimicrobial stewardship can help to reduce the negative consequences of inappropriate antibiotic use. This quality improvement project targets to do this by aiming to improve the proportion of 48-hour antimicrobial reviews completed and documented on two surgical wards at Darent Valley Hospital with a goal of 100% compliance.
This project used four PDSA (plan, do, study, act) cycles to achieve our aim: a trust-wide email; education sessions with junior doctors; sticker reminders in patient notes; presenting our study to surgical consultants and displaying posters on the wards.
The proportion of antimicrobial reviews completed at 48 hours in the patient notes increased from 18% to 77% over 19 weeks from 10 October 2018 to 20 February 2019. The most successful intervention was providing a presentation for consultants at an audit meeting in conjunction with displaying posters on the wards.
The most successful interventions (education sessions with junior doctors and presentation to surgical consultants alongside displaying posters on the wards) were found to be those that required minimal further input after their initial rollout. This project was carried out by medical students and is highly transferrable to other hospitals, and highlighted that a successful quality improvement project can be undertaken by any member of the healthcare team.
- antibiotic management
- quality improvement
- clinical practice guidelines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Prior to the start of this study, the uptake of 48-hour antimicrobial reviews on the surgical wards at Darent Valley Hospital (DVH) was considered to be at an unacceptably low level, thus demonstrating a lack of antimicrobial stewardship. The aim of this quality improvement project (QIP) was to improve the proportion of 48-hour antimicrobial reviews completed and documented on two surgical wards at DVH with a goal of 100% compliance.
DVH is located in Dartford, a commuter town for London. The majority of patients staying on the two surgical wards included in this study were prescribed at least one antimicrobial and had a short length of stay, an average of 5.1 days, meaning that there was a high turnover of patients throughout the duration of our study.1 The two surgical wards were classed as general surgery wards, although the majority of patients were lower gastrointestinal cases. The therapeutic guidelines used on the two surgical wards for antimicrobial prescriptions were in line with hospital and trust-wide policy. DVH employs a paper-based system for recording patient notes and patient drug charts with no electronic system available at present.
The issue of poor compliance with 48-hour antimicrobial review completion and documentation was raised by the hospital’s pharmacy department who identified this issue in their bimonthly audit of antimicrobial stewardship (Hospital Antimicrobial Prudent Prescribing Indicator) which identifies departments and standards requiring improvement. The pharmacy department viewed the current level of 48-hour antimicrobial review uptake as detrimental to patient care with the surgical wards consistently the lowest performing, so we attempted to tackle this problem by using the interventions described in this study.
Background
The misuse of antibiotics leads to the emergence of antimicrobial resistance, an important public health and patient safety issue, while concurrently reducing the efficacy of antimicrobial treatments against infection.2 Infections caused by resistant organisms are associated with poorer clinical outcome and a prolonged hospital stay when compared with infections caused by susceptible organisms.3 4
Antimicrobial stewardship enforces measures to reduce the adverse effects of antimicrobial use by reducing inappropriate antibiotic prescriptions.3 This encompasses a reduction in unnecessary antibiotic use, unsuitable use of broad-spectrum antibiotics and inappropriate dosage or duration of antibiotic use.5
From November 2011, the ‘Smart Start-Then Focus’ antimicrobial stewardship package encouraged documentation on the drug chart and in medical notes of the route, indication, does and duration of any antibiotic treatment. The rationale behind this is that antibiotics are often continued unnecessarily because clinicians caring for a patient do not have information specifying why the antibiotic was initially commenced, and the intended duration of antibiotic course.3
The ‘Smart Start-Then Focus’ initiative also suggested reviewing the clinical diagnosis and the need for continuing antibiotics by 48 hours. At this stage, a clear, active, antimicrobial stewardship decision should be made and documented (stop the antibiotic, switch from intravenous to oral, change antibiotic, continue and review again at 72 hours, change to outpatient parenteral antibiotic therapy).3 The fulfilment of this particular task is what we are trying to improve in our QIP.
A recent QIP aimed to improve the completion of 48-hour antimicrobial reviews in drug charts on a respiratory ward.6 This project was deemed to be successful, as demonstrated by an increase in completion of 48-hour antimicrobial reviews in drug charts, and a reduction in the number of days that patients were prescribed intravenous antibiotics for. Of the seven PDSA (plan, do, study, act) cycles carried out, the most efficacious were: educational talk by consultant, inclusion of 48-hour review status on daily handover and active ward pharmacy involvement. Interventions with less impact were visual prompts and magnets on the patient whiteboard.6 7
A recent audit demonstrated that consistent review of antibiotic prescriptions at 48 hours would improve adherence with the Department of Health’s ‘Smart Start-Then Focus’ guidance, and would improve patient care by allowing for a switch to oral therapy or completion of antibiotic course to take place earlier.8 This audit also estimated that with appropriate observance of 48-hour antimicrobial reviews, 1800 hospital bed days could be saved locally.8 In the context of the National Health Service (NHS) as a whole, the number of hospital bed days saved would be significantly greater, with an associated increase in patient safety and reduction in costs.
Measurement
Initial data collection formed the baseline measurement. This involved collecting data from two surgical wards at two points in time on consecutive weeks. Data were collected on the antimicrobials prescribed and whether they had been reviewed at 48 hours in the drug chart, whether the completion of a review had been documented in the patient notes and whether any changes had been made to the antimicrobial prescription as a result of the 48-hour review. In order to assess the success of our PDSA cycles, we would continue to collect data in these three domains 1 week after the implementation of an intervention.
The proportion of 48-hour antimicrobial reviews documented in patient notes was our primary process measure. The patient notes are where all information regarding a patient for the duration of their hospital stay accumulates, and is used as a reference point by all branches of the multidisciplinary team for any queries regarding a patient. It was deemed to be the most important place to document a 48-hour antimicrobial review as it would be easily accessible to all staff involved in the patient’s care, and in contrast to the patient’s drug chart, would be less likely to be changed during the patient’s stay in hospital, and provides more space for the prescriber to provide information on the indication and length of antimicrobial course which, following guidance from the ‘Smart Start-Then Focus’, would be useful for other clinicians in future management decisions.
The proportion of antimicrobial prescriptions changed at 48 hours was our secondary process measure as it would indicate whether changes in the primary process measure were leading to a positive change in practice, for example, switching from intravenous to oral antibiotic. As was highlighted by the ‘Start Smart-Then Focus’ initiative, an antimicrobial stewardship decision at 48 hours is vital to improving standards of patient care.6
Data were collected from all patients who were staying on the ward on the day on which data collection was taking place. Baseline data were collected on two dates in order to ensure an adequate sample size from which the baseline measurement could be made. Thereafter, data were collected 1 week after the implementation of each respective PDSA cycle. The four dates for data collection after each PDSA cycle are as follows: 26 November 2018, 5 December 2018, 13 February 2019 and 20 February 2019.
For the duration of the QIP, data were collected by a team of five medical students, with four medical students being involved with each round of data collection. The students were divided into two pairs, with each pair collecting the data for a ward; this took approximately 90 min. Prior to the start of the project, the medical students attended lectures at their university on how to successfully carry out a QIP in a clinical environment. The medical students then received further training and support from the QIP lead at DVH, as well as from the surgical consultant and pharmacists with whom they were working with closely for the duration of the project.
Design
This QIP implemented four PDSA cycles over a period of 19 weeks. The PDSA cycles were carried out on two surgical wards, led by medical students in conjunction with antimicrobial pharmacists and the microbiology team.
A process mapping exercise identified key areas amenable to demonstrate improvement. Additionally, the team shadowed ward rounds to establish how 48-hour antimicrobial reviews were completed in practice and to provide an opportunity to discuss the topic with clinical staff. The primary process measure, the proportion of antimicrobial reviews completed at 48 hours in patients’ clinical notes, was developed to quantify any improvement. Other measures were recorded to review improvements in adherence to national antimicrobial stewardship guidelines and as a surrogate measure of improvement in patient outcome.9
The PDSA cycles focused on raising awareness of antimicrobial resistance and stewardship, educating both junior and senior healthcare staff, and designing stickers and posters to serve as sustainable forms of reminders on the wards.
Strategy
PDSA cycle 1
A trust-wide informational email to raise awareness about the risk to patients and consequences to the hospital of not completing a 48-hour antimicrobial review, and provide information on what an antimicrobial review constitutes. This was chosen as the first intervention after initial discussions with hospital staff showed a general lack of awareness of the existence of the 48-hour antimicrobial review. The email was developed by the medical students and pharmacy team, and sent during the annual ‘Antibiotic Awareness Week’ to all clinical staff. The email communicated information on what a 48-hour antimicrobial review is, the benefits of 48-hour antimicrobial reviews and how to complete a 48-hour antimicrobial review. The email was sent out on 16 November 2018, with measurements collected on 26 November 2018 to assess the efficacy of PDSA 1.
Feedback from staff on the surgical wards suggested that the information provided in the trust-wide informational email was not easy to digest in the format in which it was presented. Staff receive a plethora of emails daily, and the email that was sent during PDSA cycle 1 was not particularly memorable or attention grabbing, and was found to be lost among the numerous other emails received by staff. After reflecting on PDSA cycle 1, the decision was made to more specifically target those directly involved in 48-hour antimicrobial reviews in future PDSA cycles.
PDSA cycle 2
Educational sessions with foundation year 1 (FY1) and foundation year 2 (FY2) doctors (newly qualified doctors who are completing their first 2 years of postgraduate training after receiving their formal medical qualification from a university) to inform them of the importance of the 48-hour antimicrobial review and highlight best practice. This intervention targeted FY1 and FY2 doctors as they were the members of staff most likely to carry out a review of antimicrobials, and therefore were felt to be the most important to educate on appropriate antimicrobial stewardship. The FY1 and FY2 doctors at DVH have weekly compulsory lunchtime teaching sessions, with attendance monitored by register. The educational session lasted approximately 20 min and involved a PowerPoint presentation delivered by medical students before the lunchtime teaching session commenced. Two educational sessions were delivered: an educational session for FY1 doctors on 27 November 2018, followed by an educational session for FY2 doctors on 28 November 2018. The content of the educational session included: an overview of antimicrobial resistance and its effect on clinical practice, the rationale behind completing a 48-hour antimicrobial review and how to complete a 48-hour antimicrobial review. Measurements were collected on 5 December 2018 to assess the efficacy of PDSA 2.
It was predicted that further awareness of the 48-hour antimicrobial review and encouragement for junior doctors to complete the review by making them aware of the advantages to both the patient and the hospital trust would lead to an increase in the uptake of 48-hour antimicrobial reviews.
Feedback highlighted that the FY1 and FY2 doctors to whom we were providing educational session for were undertaking 4-month rotations, so after this period would leave the surgical ward and be replaced by a new junior doctor. As a result, this was not deemed to be the most sustainable strategy as it would involve regular re-educating of junior doctors’ every time they change rotations. Consequently, we endeavoured to try to create more long-lasting interventions for our next PDSA cycles.
PDSA cycle 3
Provision of stickers detailing how to conduct an antimicrobial review that, placed in the drug chart and patient notes, remind doctors to carry out the 48-hour antimicrobial review. The stickers were designed by medical students and pharmacists, and then printed by the pharmacists. After the medical students consulted the nurse in charge for each surgical ward, it was agreed that from 6 February 2019 the nursing team would place the stickers in the patient notes for all patients who stay on the ward. Prior to starting this intervention, the nurses on each ward were given a brief talk by the medical students which detailed the purpose of the QIP and what was required of them in terms of distributing stickers. The stickers contained a reminder to review antimicrobials at 48 hours, provided the trust-wide criteria for switching an antibiotic from an intravenous to oral prescription and provided an area for a doctor to indicate that an antimicrobial review had been conducted and, if necessary, to indicate any reasons as to why an antimicrobial was not changed at 48 hours. Measurements were collected on 13 February 2019 to assess the efficacy of PDSA 3.
It was predicted that the stickers would prompt doctors to carry out a 48-hour antimicrobial review, leading to an increase in the uptake of 48-hour antimicrobial reviews. It was also hoped to be more sustainable than our previous interventions.
Feedback provided by nurses on the surgical wards highlighted that it was difficult for them to continue to place stickers in every drug chart and in all of the patients’ notes. The need to continually place stickers in the drug chart and patient notes was deemed to an unfeasible addition to the already heavy workload of the nurses on the surgical wards.
PDSA cycle 4
A presentation at the monthly surgical audit meeting attended by surgical consultants and placement of posters on the surgical wards to remind staff to carry out the 48-hour antimicrobial review. The presentation was made by medical students and endorsed by the surgical consultant who was supervising the students during the QIP. The presentation was jointly delivered by medical students and supervising consultant on 13 February 2019. The content of the presentation included: an overview of antimicrobial resistance and its effect on clinical practice, the rationale behind completing a 48-hour antimicrobial review, how to complete a 48-hour antimicrobial review and a discussion about how to improve adherence to 48-hour antimicrobial reviews at DVH. The consultants were encouraged to disperse the information provided in the presentation to their smaller clinical teams with whom they work closely. The posters were A3 in size and printed in colour. On 13 February 2019, the posters were placed on noticeboards around the ward and in areas where staff are likely to congregate, for example, the staff room. The location of poster placement had to be agreed with the ward manager beforehand. The posters provided a reminder to complete the 48-hour antimicrobial review and highlighted how to appropriately conduct an antimicrobial review. Measurements were collected on 20 February 2019 to assess the efficacy of PDSA 4.
It was predicted that presenting to surgical consultants would provide them with information to be disseminated to junior doctors and nurses, and posters would remind doctors to carry out the 48-hour antimicrobial review, both leading to an increase in the uptake of 48-hour antimicrobial reviews.
Our final intervention built on the feedback that had been received from our three previous PDSA cycles. Engaging senior staff who were prominent on the ward and providing blatant reminders for ward staff through the placement of posters on the surgical wards ensured that PDSA cycle 4 resulted in the highest level of our primary process measure.
Results
During the QIP, 175 prescribed antimicrobials, across 88 patient charts, were reviewed (see table 1). At baseline, 11 antimicrobials (18%) had evidence of a 48-hour antimicrobial review documented in the patient notes, and changes were made to 22 antimicrobial prescriptions (37%) at 48 hours. The primary process measure showed the proportion of antimicrobial reviews completed at 48 hours in the patients’ notes increased from 18% to 77% during the project, with an increase elucidated during each PDSA cycle (figure 1). The biggest increases were seen after PDSA cycle 2 (education sessions directed at junior doctors) and PDSA cycle 4 (surgical audit presentation and posters) with increases of 20% and 27%, respectively.

A run chart showing the effect of interventions on the uptake of 48-hour antimicrobial review in patient notes.
Measurement points
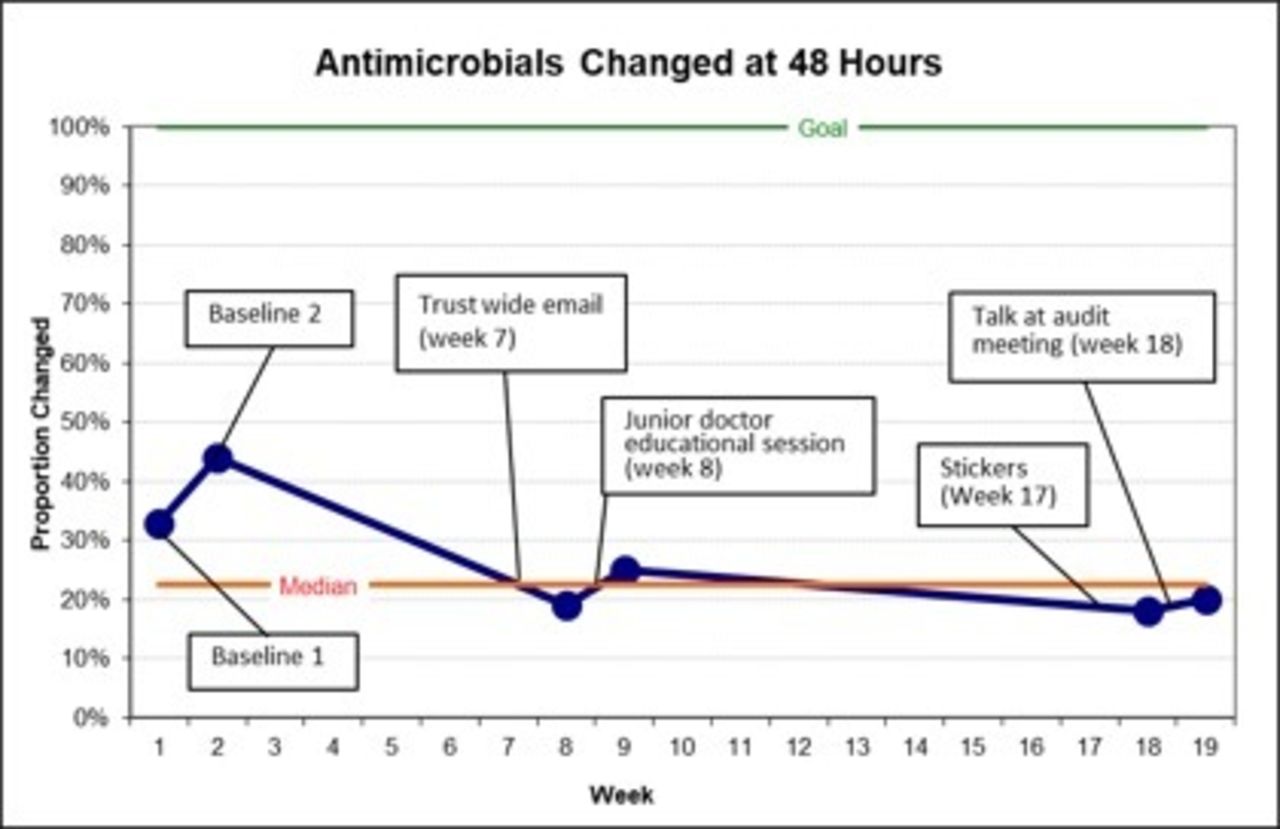
The secondary process measure, the proportion of antimicrobial prescriptions changing at 48 hours, was highest (37%) at the start of the project and fluctuated between 18% and 25% from the second to fifth measurement cycle (figure 2). An increase in changes to antimicrobial prescriptions was seen after the second and fourth intervention, mirroring the trend in the primary process measurement.
{kind=link}
{kind=link}
A run chart showing the effect of interventions on changes being made to an antimicrobial prescription at 48 hours.
PDSA 1
There was an increase in patient notes documentation from 18% to 27%. Despite the increase in the uptake of 48-hour antimicrobial reviews, there was a fall in the proportion of antimicrobials to which changes were made at 48 hours, suggesting that although drugs were being reviewed, further action was not being taken by doctors.
PDSA 2
There was an increase in patient notes documentation from 27% to 47%. The information we provided junior doctors regarding the positive effects the 48-hour antimicrobial reviews have on patient outcome gave rise to an increase in changes made to antimicrobials.
PDSA 3
Although a further increase in patient notes documentation is apparent, this cycle showed the least improvement. We had doubts as to how the intervention was being implemented by staff, and during our data collection, we found no evidence of the intervention being carried out, resulting in the decrease of changes made to antimicrobials.
PDSA 4
There was an increase in patient notes documentation to 77%. The surgical audit presentation ensured that surgical consultants were aware of our project, and posters placed around the two surgical wards reminded doctors to carry out reviews of antimicrobials which led to the proportion of antimicrobials documented in patient notes rising to its highest recorded level.
Lessons and limitations
The aim of this QIP was to improve the proportion of 48-hour antimicrobial reviews completed and documented on two surgical wards with a goal of 100% compliance. As our data were collected over a 19-week period, it was essential for our interventions to be sustainable over this period to see positive results at the end of our QIP, and beyond the completion of the project to ensure that any changes made could be maintained in the long term to improve the quality of patient care in the future. We found issues with the sustainability of our initial PDSA cycles and made attempts to correct this in PDSA cycle 3 and PDSA cycle 4 with interventions that did not require constant input. This was particularly notable as half of our interventions took place after the Christmas break, with the new year introducing a different cohort of staff as both nursing and medical staff joined the surgical wards as part of a new training rotation. However, new medical staff were exposed to PDSA cycles 1 and 2 (trust-wide email and education sessions with junior doctors). Furthermore, senior nursing staff and senior medical staff were retained which suggests their important role in maintaining antimicrobial review documentation, and provides an explanation as to why there was still an improvement in antimicrobial review documentation. The poor results experienced in PDSA cycle 3 highlighted the importance of implementing more sustainable interventions that are not affected by the turnaround of staff, or targeting interventions on staff who would remain on the surgical ward for a prolonged period of time such as the ward sister or surgical consultants.
Difficulty in engaging the ward staff was the most significant barrier to the success of the project. In our discussions with the ward staff, we learnt that our project was often considered surplus to the work carried out by an already overburdened workforce. This was problematic as staff collaboration was essential for the successful implementation of some interventions, for example, PDSA cycle 3 (stickers). This could have been overcome by involving surgical consultants at an earlier stage; with the support of senior staff, it was possible to bridge the gap with ward staff and implement more successful interventions. It is likely we were undermined due to our position as medical students, and if we held a more senior role within the trust (eg, junior doctor), or were seen to be working closely with senior hospital staff, there would have been a greater degree of engagement in our project.
The secondary process measure, the proportion of changes made to antimicrobial prescriptions, changed a little during our project and was below the baseline measurement by the end of the project. This is disappointing as it was hypothesised that an increase in 48-hour antimicrobial reviews being completed would result in more antimicrobial prescriptions being changed at 48 hours. On reflection, this may be explained by placing too much of an emphasis during PDSA cycles on improving compliance with 48-hour antimicrobial reviews without providing a thorough explanation as to why it was important and what changes we hoped to bring about, thus making the 48-hour antimicrobial review appear as a tick box exercise. There were efforts made to address this, such as in PDSA cycle 2 where there was discussion with the FY1 and FY2 doctors on the benefits of completing the 48-hour antimicrobial review, but again, its effect was limited. Another reason may be that before this QIP, antimicrobials were already being changed appropriately at 48 hours but not documented. A future project could try to establish how many antimicrobials could change to a more appropriate one and if this can be improved. This should take into account both guidelines and clinical indication, which may be hard to measure retrospectively. Our project aimed to measure guideline adherence with our secondary process measure; however, this was difficult to assess as we only collected data on one aspect of the guidelines. A potential solution to antimicrobials being changed without a documented review, which was beyond the scope of this project, is to implement a hard time-limiting prescription of antimicrobial, requiring a review at 48 hours, and if this is not completed, the prescription will be stopped.10
No significant issues were encountered with data collection. Before data collection began, the nursing team on the wards were made aware of our presence and we were never limited in our access to the ward or any documentation. In hospitals with electronic patient records and prescribing systems, data collection could be significantly streamlined and lead to an increase in the number of patients and wards reviewed. Furthermore, employing an e-prescribing system would aid compliance with conducting 48-hour antimicrobial reviews as this can incorporate features to remind clinical staff that a review requires completion.
Conclusion
This QIP was able to identify interventions that can be used to improve staff engagement with antimicrobial stewardship and assess the effectiveness of these on two surgical wards. At the end of our QIP, the proportion of the 48-hour antimicrobial reviews being documented in the patient notes was 77%. Despite not achieving the set target, the trust-wide email, and the surgical audit and posters were found to be successful interventions which have scope to be sustainable: they are not resource or labour intensive, require minimal input after implementation and ensure that senior staff are engaged with the project.
Similar to other studies in this area, this project found that senior doctor awareness and involvement is vital to promoting good practice with regard to antimicrobial prescriptions.6 The most impactful intervention with the most positive feedback was a presentation of our results to consultants at the monthly surgical audit meeting (PDSA cycle 4). This intervention is also the most likely to remain sustainable by concerning the most senior staff with the most authority and long-term impact on practices at DVH.
This project demonstrated that medical students can conduct a successful QIP while promoting best practice in antimicrobial prescriptions.9 This project is replicable to other wards in DVH which also have a requirement for the completion of a 48-hour antimicrobial review, and ultimately other Trusts, particularly if the lessons learnt are applied to future projects.
Future iterations of this project should try to accomplish the following in order to achieve and maintain improvement
Implement interventions that require minimal further input from ward staff once they have been put in place.
Recruit surgical consultants and other key stakeholders (eg, hospital antimicrobial stewardship lead).
Ensure that ward staff are aware of the rationale behind the project.
Acknowledgments
The authors would like to thank the staff of the surgery department at Darent Valley Hospital for their involvement in this study.
Footnotes
Contributors RSS: designed the study, was involved in the implementation of interventions, data collection, data analysis, drafting of the manuscript, writing the final manuscript, revised the manuscript for intellectual content and is responsible for the overall content of the study. KKR: designed the study, was involved in the implementation of interventions, data collection, data analysis, drafting of the manuscript, writing the final manuscript and revising the manuscript for intellectual content. JMSC, HHL and NJ: designed the study, were involved in the implementation of interventions, data collection, data analysis and drafting of the manuscript. MJ, RP and JN: designed the study, were involved in the implementation of interventions and oversaw the progress of the interventions in a supervision role for the five medical students (RSS, KKR, JMSC, HHL and NJ).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.