Article Text

Abstract
Objective Test whether Sudarshan Kriya Yoga (SKY) was non-inferior to cognitive processing therapy (CPT) for treating symptoms of post-traumatic stress disorder (PTSD) among veterans via a parallel randomised controlled non-inferiority trial.
Setting Outpatient Veterans Affairs healthcare centre.
Participants 85 veterans (75 men, 61% white, mean age 56.9) with symptoms of PTSD participated between October 2015 and March 2020: 59 participants completed the study.
Interventions SKY emphasises breathing routines and was delivered in group format in a 15-hour workshop followed by two 1-hour sessions per week for 5 weeks. CPT is an individual psychotherapy which emphasises shifting cognitive appraisals and was delivered in two 1-hour sessions per week for 6 weeks.
Measures The primary outcome measure was the PTSD Checklist-Civilian Version (PCL-C). The secondary measures were the Beck Depression Inventory-II (BDI-II) and Positive and Negative Affect Scale (PANAS).
Results Mean PCL-C at baseline was 56.5 (±12.6). Intent-to-treat analyses showed that PCL-C scores were reduced at 6 weeks (end of treatment) relative to baseline (SKY, −5.6, d=0.41, n=41: CPT, −6.8, d=0.58, n=44). The between-treatment difference in change scores was within the non-inferiority margin of 10 points (−1.2, 95% CI −5.7 to 3.3), suggesting SKY was not inferior to CPT. SKY was also non-inferior at 1-month (CPT–SKY: −2.1, 95% CI −6.9 to 2.8) and 1-year (CPT–SKY: −1.8, 95% CI −6.6 to 2.9) assessments. SKY was also non-inferior to CPT on the BDI-II and PANAS at end of treatment and 1 month, but SKY was inferior to CPT on both BDI-II and PANAS at 1 year. Dropout rates were similar (SKY, 27%, CPT, 34%: OR=1.36, 95% CI 0.51 to 3.62, p=0.54).
Conclusions SKY may be non-inferior to CPT for treating symptoms of PTSD and merits further consideration as a treatment for PTSD.
Trial registration number NCT02366403.
- Anxiety disorders
- Depression & mood disorders
- MENTAL HEALTH
- Clinical trials
- COMPLEMENTARY MEDICINE
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This paper reports a non-inferiority trial, a preferred design when efficacious treatments have been established.
The control condition, cognitive processing therapy, is a recommended first-line treatment for post-traumatic stress disorder.
Outcomes were evaluated at end of treatment and at 1-month and 1-year follow-ups.
Power was limited by the moderate sample size (n=85).
Introduction
Post-traumatic stress disorder (PTSD) is a debilitating condition that can develop after exposure to a traumatic event.1 Symptoms include re-experiencing, avoidance, negative alterations in cognition and mood, and increased arousal and reactivity.2 The lifetime prevalence of PTSD is estimated at 24.5% in veteran populations.3
Veterans Affairs (VA)/Department of Defense (DoD) clinical practice guidelines recommend evidence-based, trauma-focused therapies including prolonged exposure therapy, cognitive processing therapy (CPT) and eye movement desensitisation and reprocessing as first-line treatments for PTSD.4 These therapies typically show large effect sizes (>1.0).5 However, up to two-thirds of individuals retain a PTSD diagnosis post treatment and dropout is a significant problem.6 7 Other treatments are urgently needed, and there are compelling reasons for considering complementary and integrative health (CIH) modalities such as yoga and meditation.8 CIH interventions can be effective,9 10 less stigmatising and are popular.11 However, a review of the literature reveals several limitations: small–medium effect sizes9 10 and methodological concerns regarding controls, small sample sizes, randomisation, blinding and reporting. More high-quality, well-controlled studies are needed.
Sudarshan Kriya Yoga (SKY) involves routines of breathing at various rates, to varying degrees of depth, and in varying postures12 and while it is not trauma-focused, preliminary research suggests that SKY is efficacious in reducing symptoms of PTSD in military veterans for up to a year,13–15 and in survivors of mass disasters.16However, it should be noted that the military veteran studies are particularly limited in their significance due to small sample sizes. Breathing is unique relative to other physiological processes: it normally operates unconsciously but through training can be consciously controlled to rapidly impact emotion.12 16 SKY is also effective for treating symptoms frequently comorbid with PTSD including depression,17 anxiety18 and insomnia.19
Published studies suggest SKY is effective in reducing symptoms of PTSD,14 15 but it has not been compared with established trauma-focused therapies. We aimed to test the efficacy of SKY by comparing it to a standard therapy in veterans with symptoms of PTSD. We used a threshold of 38 on the PTSD Checklist (PCL-5) to determine eligibility, which is indicative of PTSD. However, we did not limit participants to individuals who met full criteria for PTSD on a diagnostic interview or to individuals whose symptoms of PTSD were the primary mental health concern. This is similar to prior studies of SKY13–15 and the way SKY is offered by Project Welcome Home Troops (PWHT), a non-profit organisation outside the VA. When a gold-standard control condition is available, a non-inferiority design is appropriate for such comparisons.20 We chose CPT21 as the control as it is a first-line manualised trauma-focused psychotherapy recommended by VA/DoD,4 and its putative top-down mechanism of action—change in cognitive beliefs leading to change in PTSD symptoms—contrasted strongly with the putative bottom-up mechanism of SKY—changes in breathing and physiology leading to change in PTSD symptoms. We chose individual CPT which is more effective than group CPT22 and consists of 12 sessions delivered either twice weekly for 6 weeks or weekly for 12 weeks. We used the 6-week version. SKY was delivered by PWHT instructors who provided the intervention in the usual format: in groups with an initial 5-day workshop. We included five extra weeks of SKY instruction to match the duration of CPT.
The primary aim was to test the hypothesis that SKY was not clinically inferior to CPT at end of treatment using the PTSD Checklist-Civilian Version (PCL-C).23 We hypothesised these effects would be maintained at 1-month and 1-year post treatment. Secondary outcomes of depression (Beck Depression Inventory-II: BDI-II)24 and affect (Positive and Negative Affect Schedule: PANAS25) were included to test the hypothesis that SKY was not clinically inferior to CPT on these outcomes. Finally, we hypothesised dropout rates would be similar across treatments.
Methods
This parallel groups randomised controlled non-inferiority trial with a 1:1 allocation ratio was conducted in a research setting at a western VA healthcare centre. Its procedures were reported in detail previously26 (online supplemental file 1) and key elements are repeated here.
Supplemental material
Participants
Participants were recruited through flyers posted at VA sites, presentations at VA outpatient treatment centres, clinician referral, mail and local advertisements. Inclusion criteria were: (1) aged≥18 years, (2) veteran of the armed forces and (3) scoring≥38 on the PCL-527 on initial telephone screening which is above the threshold score of 31–33 indicating a diagnosis of ‘probable PTSD’28), but not necessarily meeting full PTSD criteria.1 Exclusion criteria were: (1) participation in another study, (2) intention to begin another behavioural therapy treatment during the study, (3) psychotropic medication started ≤8 weeks prior to screening (4) mania or psychosis within the past 6 months, (5) suicidal or homicidal intent within the past 60 days, (6) substance dependence (other than nicotine) within the past 30 days, (7) seizure disorder and (8) severe traumatic brain injury. Items 4–5 were assessed using the Mini International Neuropsychiatric Interview V.7.029 and items 3, and 6–7 were assessed during an initial telephone screening. Remaining criteria were assessed, informed consent was obtained, and a health history was taken during an on-site screening visit (online supplemental table 1).
Subsequent assessments were conducted in interview rooms by staff blinded to treatment on four occasions (baseline, end of treatment, 1-month follow-up, 1-year follow-up: (online supplemental table 1). Baseline assessments (PCL-C, PANAS, BDI-II, Clinician-Administered PTSD Scale for the Diagnositc and Statistical Manual of Mental Disorders-5 (DSM-5) (CAPS-5)) and randomisation occurred when sufficient participants had been recruited and ≤1 week before treatment began.
Randomisation occurred by each participant blindly drawing a sealed envelope out of a box containing an equal number of envelopes for each treatment. In the event that a cohort had an odd number of participants, the study coordinator alternated which treatment the extra envelope contained. Treatment proceeded over a 6-week period in 10 cohorts (average 9.2 participants per cohort, range 6–12) (figure 1). The measures administered at baseline were readministered at 6 weeks (end of treatment), ≤1 week following the last treatment session. Follow-up assessments (PCL-C, PANAS, BDI-II) occurred 1-month and 1-year post treatment. Participants were reimbursed at the end of treatment and 1-year assessments.

Consolidated Standards of Reporting Trials flow diagram. CPT, cognitive processing therapy; ITT, intent to treat; SKY, Sudarshan Kriya Yoga.
Procedures
Cognitive processing therapy
CPT was given individually by one of three therapists in 12 60-min sessions twice per week for 6 weeks30 31 for a total of 12 contact hours. The ‘cognitive only’ version,32 which excludes a written trauma account,33 was used. Sessions (online supplemental table 2) were delivered by a licensed psychologist or a postdoctoral clinical psychology fellow, all of whom were certified by the VA’s national CPT training initiative. The licensed clinical psychologist provided weekly supervision to the fellows and received weekly consultation from a clinical psychologist employed by the study VA’s outpatient PTSD treatment clinic.
All sessions were audio recorded, and study CPT clinicians were trained to criterion in rating therapist adherence and competence according to a standard protocol.34 No clinician rated their own session. Adherence was defined as the percentage of components executed and was 91%. Competence was defined as therapists’ skill in delivering these components on a 0 (not executed) to 6 (textbook quality) scale. Mean (SD) competence was 4.4 (1.1) for unique and essential elements and 4.3 (0.8) for essential but not unique elements, which were comparable to prior published trials.35
Sudarshan Kriya Yoga
SKY was provided in group format (3–6 participants) in a large conference room by two of four SKY instructors from PWHT who were knowledgeable about military culture and the SKY technique. We included an initial 5-day intensive group workshop (3 hours per day) as used by PWHT. As treatment dropout often increases over time, we deemed that equating treatment duration to CPT (ie, 6 weeks) was important for determining non-inferiority. We therefore included 10, 60-min sessions twice per week (online supplemental table 3), yielding a 6-week treatment. SKY involved 25 hours of contact time.
Five different breathing techniques were taught: (1) alternate nostril breath, (2) straw breathing, (3) three-stage victory breath, (4) bellows breath and (5) SKY breath which is a cyclical breathing exercise guided by an audio CD, consisting of slow, medium and fast breath cycle rates (see12 26 for details). Sessions closed with a meditation/rest phase. Homework was optional but strongly encouraged and consisted of a shorter version of the SKY breath routing.
SKY sessions were video recorded and SKY therapists rated a random sample of 20% of treatment video tapes (45 of 225 treatment hours) and recorded whether the instructors adhered to the protocol using a checklist of the main elements. SKY sessions had a 95.8% adherence rate.
Measures
PTSD Checklist-Civilian Version36
Primary outcome measure given at baseline, end of treatment, 1-month and 1-year post treatment . A 17-item self-report measure for assessing PTSD symptom severity in the past month corresponding to DSM-IV criteria for PTSD. Scores range from 17 to 85 with higher scores reflecting greater severity. We used the civilian version to assess symptoms from both military and non-military trauma. The PCL shows good temporal stability, internal consistency, test–retest reliability and convergent validity.37 We selected the PCL-C as the primary outcome measure over the subsequent PCL for DSM-5 (PCL-5) version because at the start of the study clinically significant improvement in scores had not been established for the PCL-5.
Post-traumatic Stress Disorder Checklist-527
Used at screening to assess eligibility. A 20-item self-report measure assessing PTSD symptom severity in the past month corresponding to DSM-5 PTSD criteria. Scores range from 0 to 80 with higher scores reflecting greater severity.
Beck Depression Inventory II24
Secondary outcome measure given at baseline, end of treatment, 1-month and 1-year post treatment. A 21-item self-report measure that assesses depression symptom severity. Items are rated on a 4-point scale according to how much the symptom bothered the respondent over the prior 2 weeks. Scores range from 0 to 63 with higher scores reflecting greater severity.
Positive and Negative Affect Schedule25
Secondary outcome measure given at baseline, end of treatment, 1-month and 1-year post treatment. A 20-item self-report measure assessing positive and negative mood states over ‘the past few weeks’ on a 5-point scale. Scores for positive and negative affect range from 10 to 50 with higher scores reflecting stronger affect.
Clinician-Administered PTSD Scale for DSM-538
Used to determine PTSD diagnostic status at baseline and end of treatment. A semistructured clinical diagnostic interview for the assessment of PTSD using DSM-5 definitions.1 Severity scores range from 0 to 80 with higher scores reflecting greater severity. Administered by study staff trained in its administration. Concerns about scoring were addressed via a weekly consensus conference with a licensed clinical psychologist (RJS-H).
Homework compliance log
A daily log recording time spent doing homework, for example, CPT reading handouts, SKY breathing exercises.
Mini International Neuropsychiatric Interview (V.7.0)29
Used at screening to assess exclusion criteria. A brief structured clinical interview to screen for current and lifetime DSM-5 and International Classification of Diseases-10 (ICD-10) mental health disorders.
Patient and public involvement
Patients and the public were not formally involved in the conception, design or dissemination of the study.
Statistical analysis
Non-inferiority margins were defined a priori to be equal to suggested minimum clinically meaningful differences: 10-points for the PCL-C39 and 3 points for the BDI-II40 and PANAS.25 The statistical analysis of non-inferiority can be conducted by using either hypothesis testing or CIs, or most rigorously by using both methods.20 We used both methods. For non-inferiority hypothesis testing, alpha was set at 0.025 for these one-sided tests of non-inferiority.20 Therefore, for example, SKY would be determined to be non-inferior to CPT if there was at least a 97.5% chance that improvements in SKY on the PCL-C were not more than 10 points less than improvements in CPT. Alternatively, SKY would be determined to be inferior to CPT if there was a greater than 2.5% chance that improvement in SKY on the PCL-C was more than 10 points less than improvement in CPT. For the CI approach to non-inferiority testing, the CI for the difference between the two interventions was calculated. If the interval crossed the boundary (is greater than the non-inferiority margin) then non-inferiority cannot be claimed.20
Power was set to 80% and type I error to p=0.025.20 Power analyses determined that ≥30 treatment completers per group were needed, and dropout was predicted to be ≤22%.6 15 We therefore estimated 76 participants needed to enter treatment for 80% power at end of treatment (actual number entered treatment=85).
Data were analysed by a statistician blind to treatment using intent to treat (ITT) and per-protocol procedures. Treatment completion was defined as ≥75% treatment sessions attended.41 Missing data in the ITT analyses used the ‘last observation carried forward’ methodology.42 43 Within-group Cohen’s d effect sizes were calculated as the mean change divided by the baseline SD44 and statistical significance was assessed using 2-sided t-tests (α=0.05). Dropout was compared across treatments using logistic regression modelling (α=0.05), using an a priori definition of dropout as attending <75% of treatment hours.
Results
The study was conducted between October 2015 and March 2020 and 85 veterans enrolled (44 CPT, 41 SKY: figure 1). Most participants were men (88%), white (61%) and had military combat experience (56%) (table 1 and online supplemental table 4).
Baseline demographic and clinical characteristics for each group
Primary outcome (PCL-C)
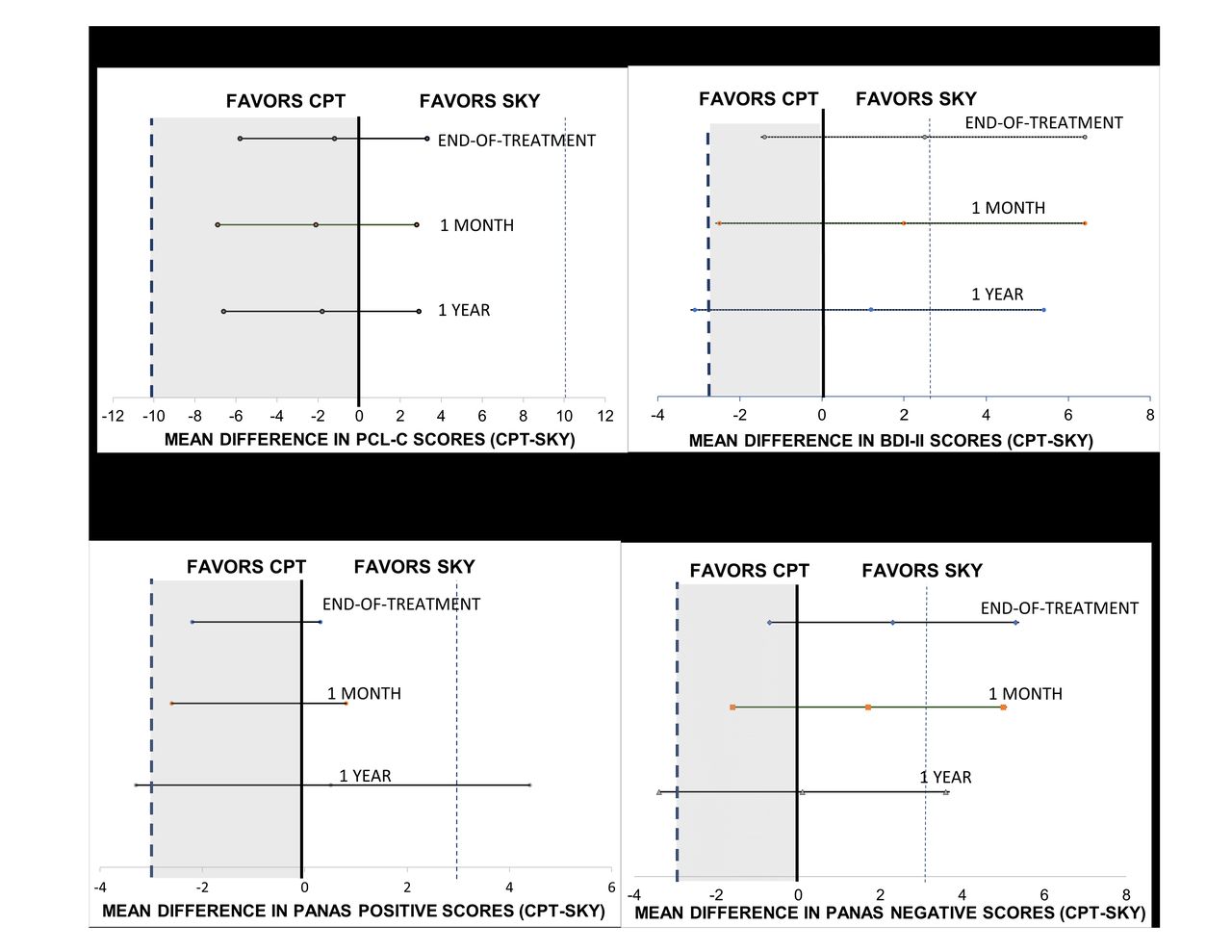
At baseline, the mean (SD) PCL-C was 56.5 (12.6). Within-group ITT analyses showed mean PCL-C scores were significantly reduced by end of treatment (table 2) (CPT, −6.8, 95% CI −10.3 to –3.33, t=3.96, p<0.003, Cohens d=0.58), (SKY, −5.6, 95% CI −8.56 to –2.56, t=3.75, p<0.0006, Cohens d=0.41). Moreover, the mean difference in PCL-C change scores between SKY and CPT at end of treatment (−1.2, 95% CI −5.7 to 3.3) met criteria for non-inferiority for SKY (table 3, figure 2a). Note that the mean change in PCL-C score in each group was lower than the minimum clinically meaningful difference of 10-points chosen for the PCL-C non-inferiority margin. Non-inferiority was also found at 1-month and 1-year following treatment (table 3, figure 2a).
Mean (SD) scores for primary and secondary outcomes for the two treatment conditions at all time points (intent to treat)
Non-inferiority tests (intent to treat)
{kind=link}
{kind=link}
Two-sided 95% CIs of the mean difference in outcome scores between treatments at the end of treatment, 1 month, and 1 year. Vertical dashed lines indicate the non-inferiority margin for Sudarshan Kriya Yoga (SKY). Grey-tinted regions indicate values which favour cognitive processing therapy (CPT) but for which SKY can be considered non-inferior: (A) post-traumatic check list (PCL-C), (B) Beck Depression Inventory-II (BDI-II), (C) Positive and Negative Affect Scale (PANAS)—Positive, (D) Positive and Negative Affect Scale—Negative.
Secondary outcomes
Depression (BDI-II)
The baseline BDI-II score was 24.9 (12.1), indicating moderate depression.24 ITT analyses showed scores generally improved by end of treatment (EOT) in both groups (CPT, −3.6, 95% CI −7.0 to –0.3, t=−2.21, p=0.03, Cohens d=0.33), (SKY, −6.1, 95% CI −8.3 to –4.0, t=−5.78, p<0.0001, Cohens d=0.90) (tables 2 and 3). The mean between-group difference (2.5, 95% CI −1.4 to 6.4) at end of treatment met non-inferiority criteria for SKY (table 3, figure 2b). Improvements in BDI-II were stable at 1 month. At 1-year improvement in SKY was greater than CPT but the CI extended beyond the non-inferiority margin. Therefore, we concluded that SKY was inferior to CPT at this time point (table 3, figure 2b).
Affect (PANAS)
PANAS positive
ITT analyses (table 2) found that changes from baseline to end of treatment were small in CPT (0.3, 95% CI −1.5 to 2.1, t=0.31, p=0.76, Cohens d=0.05), but improved significantly in SKY (2.5, 95% CI 0.6 to 4.3, t=2.73, p<0.01, Cohens d=0.43). At end of treatment, the mean difference in change scores between SKY and CPT (−2.2, 95% CI −4.7 to 0.3) met non-inferiority criteria for SKY (table 3). Non-inferiority was also found at 1 month, but at 1-year SKY was statistically inferior to CPT using both CI and t-tests (table 3, figure 2c).
PANAS negative
ITT analyses showed a similar pattern to PANAS positive (table 2). Negative affect was not significantly reduced by CPT (−0.9, 95% CI −3.5 to 1.8, t=−0.65, p=0.52, Cohens d=0.10) but was by SKY (−3.2, 95% CI −4.6 to –1.7, paired t=−4–42, p<0.0001, Cohens d=0.69). Analyses met non-inferiority criteria for SKY at end of treatment (2.3, 95% CI −0.7 to 5.3) and 1 month (table 3). At 1 year, improvements were similar across treatments, but the CI included the non-inferiority margin; therefore, SKY was statistically inferior to CPT at this time point (figure 2d).
Dropout
Dropout was 30.6% (figure 1) and was similar across treatments (CPT: n=15, 34%, SKY: n=11, 27%) (difference in proportion=0.07, 95% CI −0.12 to 0.27, p=0.47). Logistic regression analysis showed dropout was not significantly related to treatment (p=0.54) or education (p=0.67) but was related to age (p<0.01) reflecting higher dropout by younger participants (online supplemental table 5). Of note, all in-person study procedures were completed before the onset of the COVID-19 pandemic.
Of 26 participants who dropped out, 9 did not attend any sessions. We explored dropout among the subset of participants who attended at least one treatment session. Among those who did so, a χ2 test indicated dropout was higher in CPT (n=12, 29%) than SKY (n=3, 9%) (difference in proportion=0.2, 95% CI 0.03 to 0.37, p=0.03). Logistic regression showed dropout was marginally related to treatment (p=0.06) (online supplemental table 5) but not education (p=0.48), and again, was higher in younger participants (p<0.05).
PTSD diagnosis
Baseline CAPS scores suggested 55 of the 85 participants (65%) met DSM-5 criteria for PTSD2 (CPT=65.9%, SKY=63.4%). For those participants who met PTSD diagnosis at baseline and whose CAPS data were available for both time points (n=41), 61.0% retained a PTSD diagnosis at end of treatment (CPT=65%, SKY 57%: χ2=0.27, p>0.05).
Homework
Participants in both groups reported high rates of homework completion on weeks in which they attended at least one session (CPT 99.4%, SKY 84.9%). Homework completion for CPT was higher than for SKY (χ2=25.6, p<0.01).
Adverse events
Two adverse events were reported. One individual in the CPT condition reported being distressed by the assignments and dropped out of treatment. We followed-up and determined the individual was not at imminent risk of harm. A second individual in the CPT condition was admitted to hospital for suicidal ideation. Neither event was unexpected, and both were probably related to study participation. No adverse events were reported in SKY.
Completer analyses
Prespecified per protocol analyses (≥75% treatment sessions) for primary and secondary outcome measures were consistent with ITT analyses at all time points, except the per protocol analysis for PCL-C at 1 month which showed SKY was inferior to CPT (online supplemental tables 6–8).
The mean change in PCL-C for CPT completers (n=29) was −8.4 (95% CI –13.2 to –3.7, Cohens d=0.67), and for SKY (n=30) was −7.7 (95% CI –11.5 to –3.9, Cohens d=0.76). Treatment effect sizes were far larger for completers than non-completers, especially in SKY group (CPT: 0.67 vs 0.37, SKY: 0.76 vs 0.02).
Discussion
This two-group randomised clinical trial examined the efficacy of SKY on symptoms of PTSD, depression, and affect in veterans. The ITT analysis supported our hypotheses: SKY was significantly non-inferior to CPT on the primary outcome of symptoms of PTSD (PCL-C) at end of treatment, 1 month, and 1 year following treatment. SKY was also significantly non-inferior to CPT on secondary outcome measures of depression (BDI-II) and affect (PANAS) at end of treatment and 1 month but was statistically inferior to both measures 1 year after treatment. As hypothesised, dropout rates were similar across treatments and were higher in younger participants.
PCL-C scores were reduced in both groups at end of treatment by a magnitude that is considered to indicate ‘reliable change’ (5–10 points) in symptom severity.45 It has been proposed that the strongest test of non-inferiority is to use both ITT and per protocol analyses.20 In the present study, per protocol analyses were largely consistent with ITT analyses, supporting our conclusion of non-inferiority. A more conservative non-inferiority margin (8.8 points on the PCL) has been used previously.46 The results of the present study would have led to the same conclusion of non-inferiority had we used this margin. The finding that SKY reduced symptoms of PTSD is consistent with previous studies13–16 and a recent meta-analysis10 which concluded that yoga or meditation produced small–medium effect sizes for PTSD (mean effect size=0.39, 95% CI 0.22 to 0.57). Although the effect size of SKY was smaller than reported in other veteran studies,13–15 those studies were either smaller or less well controlled than the current study. Likewise, the effect size of CPT in our study was smaller than sometimes reported. Normative effect sizes can be difficult to define, but veteran studies using the PCL-C to measure CPT outcomes have reported effect sizes of between 1.0247 and 1.39.48 Such comparisons are important because non-inferiority studies that do not achieve the expected control effect size raise questions about validity.49 The study was designed without the need for a PTSD diagnosis at baseline; therefore, a floor effect is possible. CPT therapists received standard CPT training via the VA’s national CPT rollout initiative and additional ongoing weekly consultation throughout the study. Ratings of CPT therapists’ adherence and competence were comparable to those of prior published trials. As a result, our findings may reflect ‘VA CPT-as-usual’. In support of this conclusion, our effect sizes for completers (≥75% treatment sessions) were similar to that found in a study of male veterans completers (≥75% treatment sessions) receiving VA treatment as usual50 who showed a pre–post change of 8.2 points on PCL-C with an approximate effect size of d=0.70. Regardless, a focus on effect size can overshadow other important factors such as non-response rates which can leave up to two-thirds of patients with a PTSD diagnosis after CPT treatment.7 By this metric, the CPT non-response rate of 65% reported here was typical of CPT treatment.7
SKY was effective (and non-inferior to CPT) at reducing symptoms of depression in the presence of symptoms of PTSD. Moderate depression at baseline improved by end of treatment to mild–moderate depression and remained stable at 1 month. Although other SKY studies have shown similar effects,16 51 prior veteran studies were small.14 15 The effects of CPT on depression were consistent with prior studies involving active-duty servicemembers or veterans (effect size 0.8–1.121 22 48). Similar to the present study, follow-up at 3 months48 and 6 months22 revealed residual symptoms of moderate depression.
The PANAS showed SKY was effective at reducing negative affect and increasing positive affect up to 1-month post treatment. At 1-year post treatment, SKY was classified as inferior to CPT due to the heterogeneity of SKY response. The decrease in PANAS negative affect supported the BDI-II findings, while the increase in positive affect suggests the alleviation of depression was not simply an absence of negative affect. Supporting this notion, there is evidence that PANAS positive and negative affect are moderately independent.52
As expected, the completer analysis showed that PCL-C outcome improved with attendance. However, the difference between SKY completers versus non-completers was particularly striking (d=0.76 vs d=0.02, respectively). This finding may reflect treatment modality: CPT administration could be tailored to an individuals’ attendance, whereas SKY could not, and suggests that if adherence to SKY can be maintained the effect size may be medium to large.
Dropout rates across the two treatments were similar. The CPT dropout rate of 34% was similar to other CPT veteran studies (16%–35%7) while the SKY rate of 27% was higher than previous veteran studies (0–9%13–15) perhaps due to the extended SKY protocol used in the current study. Dropout was higher in younger participants across both treatments, as previously reported41 but was not related to education as previously observed.41 Our exploratory analysis of participants who attended at least one treatment session indicated that dropout after attending at least one session was significantly lower in SKY than CPT. One explanation is that participants who experienced at least the first session of SKY tended to find the treatment more acceptable than CPT and completed treatment. However, this conclusion is speculative and needs further investigation.
The study has several strengths. First, we used a non-inferiority randomised controlled design, which is preferable to a superiority design when an existing treatment has been established to be effective and the experimental treatment has other potential advantages.20 Second, we used a first-line PTSD treatment as a control, which set a high bar to conclude non-inferiority. Third, individuals with significant symptoms of PTSD were included regardless of whether they met full criteria for PTSD and whether their symptoms were their primary concern, making this a broadly representative sample. Indeed, many individuals have clinically significant symptoms yet fall short of meeting diagnostic criteria.53 Fourth, assessors were blind to treatment. Finally, the study included a 1-year follow-up which was completed by a relatively large portion of participants, providing valuable information about therapeutic durability.
There were several limitations. First, SKY involved more hours of instruction than CPT (25 vs 12 hours) which may have favoured SKY. Second, CPT’s effect size was smaller than sometimes reported and we discuss possible reasons for this. There were differences between the two groups in the background of providers, with SKY being delivered by the primary proponents of SKY for veterans. What we report here may best generalise to ‘VA treatment-as-usual’ for CPT and the Project Welcome Home Troops’ ‘Power Breath’ workshop for SKY. We also acknowledge that the primary outcome measure (PCL-C) relates to the now outdated DSM-IV definition of PTSD and has now been superseded by the more recent PCL-5. Finally, while the results were promising for SKY, the sample size (n=85) was moderate, indicating a need for further efficacy studies of SKY for symptoms of PTSD.
We found preliminary evidence that SKY may be non-inferior to CPT for treating symptoms of PTSD and negative mood in veterans. This finding is qualified by a somewhat smaller than typical effect size in the control condition, CPT. Although SKY has previously been shown to have therapeutic value, this is the first trial we are aware of comparing SKY to an established, first-line trauma-focused therapy. We conclude that SKY deserves further clinical and research consideration as a treatment for PTSD and may be appropriate for individuals seeking a non-trauma-focused therapy.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Stanford University institutional review board (#32252). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the participants for their time. We also thank Rachael H. Cho, Marcelle A. Friedman, and Jennifer Hanft for assistance with data collection. We thank Shannon Wiltsey Stirman, PhD for training in CPT fidelity rating. We thank Project Welcome Home Troops, and particularly Leslye Moore, Denise Marcus, and Denise Richardson, for their generous support throughout the project in providing SKY.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design of study: PJB, JMZ, CSR, LCL, EMS. Acquisition of data: PJB, JST, RJS-H, DCM, TA, MW, ASB. Analysis and/or interpretation of data: PJB, RJS-H, BH, LCL. Drafting the manuscript: PJB, RJS-H. Revising the manuscript critically for important intellectual content: PJB, RJS-H, DCM, TA, CSR. Approval of the version of the manuscript to be published: all authors. PJB is the guarantor.
Funding Funded by a Department of Veterans Affairs RR&D Merit Review (1 I01 RX001485-01: PJB). DCM,TJA and RJSH received advanced fellowship funding from the Veterans Health Administration, Office of Academic Affiliations. Funding bodies have not, and will not, participate in the study design, the collection, management, analysis, or interpretation of data, nor the writing of findings for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.