Article Text

Abstract
Background Missed opportunities for diagnosing cancer cause patients harm and have been attributed to suboptimal use of tests and referral pathways in primary care. Primary care physician (PCP) factors have been suggested to affect decisions to investigate cancer, but their influence is poorly understood.
Objective To synthesise evidence evaluating the influence of PCP factors on decisions to investigate symptoms of possible cancer.
Methods We searched MEDLINE, Embase, Scopus, CINAHL and PsycINFO between January 1990 and March 2021 for relevant citations. Studies examining the effect or perceptions and experiences of PCP factors on use of tests and referrals for symptomatic patients with any cancer were included. PCP factors comprised personal characteristics and attributes of physicians in clinical practice.
Data extraction and synthesis Critical appraisal and data extraction were undertaken independently by two authors. Due to study heterogeneity, data could not be statistically pooled. We, therefore, performed a narrative synthesis.
Results 29 studies were included. Most studies were conducted in European countries. A total of 11 PCP factors were identified comprising modifiable and non-modifiable factors. Clinical judgement of symptoms as suspicious or 'alarm' prompted more investigations than non-alarm symptoms. ‘Gut feeling’ predicted a subsequent cancer diagnosis and was perceived to facilitate decisions to investigate non-specific symptoms as PCP experience increased. Female PCPs investigated cancer more than male PCPs. The effect of PCP age and years of experience on testing and referral decisions was inconclusive.
Conclusions PCP interpretation of symptoms as higher risk facilitated testing and referral decisions for possible cancer. However, in the absence of 'alarm' symptoms or ‘gut feeling’, PCPs may not investigate cancer. PCPs require strategies for identifying patients with non-alarm and non-specific symptoms who need testing or referral.
PROSPERO registration number CRD420191560515.
- primary care
- public health
- general medicine (see internal medicine)
- oncology
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All research data supporting this publication are provided within this article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To our knowledge, this is the first study that has examined a range of primary care physician (PCP) factors affecting testing and referral decisions in a cancer context.
We identified the role PCP factors play in managing ‘alarm’ symptoms and make recommendations for improving testing and referral decisions for patients with non-alarm and non-specific symptoms.
We were unable to perform a meta-analysis due to heterogeneity of outcomes among studies.
Introduction
Diagnostic error, which encompasses missed, delayed and incorrect diagnosis, is a major patient safety concern in primary care1. Cancer is among the most frequently missed diagnoses in this setting internationally.2–4 Improving patient safety in primary care has been identified by the World Health Organization (WHO) as a priority.5 Achieving a timely cancer diagnosis can be challenging due to low cancer incidence among populations presenting to primary care,6 patient comorbidity7 8 and overlapping symptoms between cancers (eg, abdominal symptoms can herald oesophageal, colorectal or renal cancer),9 as well as more commonly occurring benign conditions.10
Clinical guidelines, such as the National Institute for Health and Care Excellence (NICE) NG12 (2015) guidelines for suspected cancer which are based on patient risk factors and symptoms most predictive of cancer,11 are used in several countries to promote timely recognition and referral of symptoms warranting investigation.12 Despite reductions in diagnostic delay across multiple cancer sites since implementation of these guidelines in the early 2000s,13 14 around one-quarter of patients with cancer (including those with symptoms of relatively high predictive value; ‘alarm’ symptoms henceforth) in an analysis of over 17 000 cases from the English National Cancer Diagnosis Audit, were deemed to have had avoidable diagnostic delay.15 Such patients often have three or more consultations before referral to secondary care for further investigation,16 in addition to poor prognosis and experiences of healthcare.17
Notwithstanding the inherent difficulty of diagnosing cancer, approximately half of cancer-related diagnostic errors identified from English National Cancer Registries and closed malpractice claims in the USA, have been attributed to PCP delay or failure to recommend an appropriate test or referral.3 7 15 Unexplained PCP variation in use of dedicated urgent referral pathways after adjusting for case-mix,18 patient and practice factors,19 has suggested potential involvement of factors related to the PCP.20 However, the PCP factors contributing to decisions to investigate cancer, and the potential benefits and disadvantages such factors may confer to decision making is poorly understood. Therefore, in this systematic review, we aimed to identify and determine the influence of PCP factors on testing and referral decisions for symptoms suggestive of cancer.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.21
Search strategy
We searched Medline, Embase, CINAHL, PsycINFO and Scopus for relevant articles from 1 January 1990 to 31 March 2021. We restricted the search from 1990 to coincide with increased public investment for primary care cancer research.22 Search queries were developed for Medline (online supplemental material 1) and adjusted according to the conventions of each database. Search terms comprised free text words and Medical Subject Headings informed by key words in titles and abstracts of relevant literature known to the authors,23–25 with input from an information specialist.
Supplemental material
Eligibility criteria
Studies were included if they were conducted in a developed country and investigated or described the influence of PCP factors on outcomes of testing and referral decisions during the diagnostic workup of adult patients (aged ≥18 years) with symptoms indicative of any cancer. We defined PCP factors as attributes that have been the object of interest regarding physician performance and competence, specifically focusing on the characteristics and attributes of physicians in clinical practice settings or the community.26 PCPs encompassed general practitioners and family physicians who have first patient contact and assume overall responsibility for coordinating patient care.27 We did not limit studies by symptom type or thresholds of cancer risk (ie, the positive predictive value of symptom profiles) because we wanted to understand how PCP factors contribute to the management of undifferentiated symptoms that are characteristic of presentations in primary care. As inferring the effect of PCP factors on individual PCP testing behaviour from associations derived in aggregate can be problematic, studies contributing quantitative data were only included if data were reported at the level of the PCP. Systematic reviews were excluded, but where relevant to our review question were used as a source of additional primary articles. We excluded commentaries, letters and editorials. There were no language restrictions.
Study selection
Citations retrieved by the search were imported into Rayyan QCRI.28 Following removal of duplicates, titles and abstracts were screened against eligibility criteria by VH. SWDM independently screened an initial 10% of titles and abstracts after which the inter-rater reliability (IRR) between reviewers was calculated using Cohen’s Kappa coefficient. The resulting coefficient value of 0.66 reflected substantial agreement and exceeded our minimum a priori IRR cut-off of ≥0.61,29 therefore, the remaining titles/abstracts were screened by VH alone. Full texts of potentially relevant studies were independently assessed by VH and AY to determine final inclusion. Reference lists of included studies and systematic reviews were hand-searched for additional articles not retrieved by the database searches. Discrepancies between reviewers were resolved through discussion or adjudicated by SA/FMW when agreement could not be reached.
Data extraction
Separate data extraction spreadsheets for quantitative and qualitative data were developed and piloted in Excel. Three authors (VH and AY/SA) independently extracted data relating to study characteristics, PCP factors, test and referral type, study results/findings, and cancer using the relevant data extraction spreadsheet. For quantitative studies, VH and AY extracted findings regarding the frequency of PCPs use of diagnostic tests and referrals and subsequent cancer diagnoses, along with odds ratios, hazard or risk ratios, or other statistical measures reported for each PCP factor. For qualitative studies, VH and SA extracted primary data (ie, participant quotations and authors’ verbatim summaries and interpretation) with the accompanying themes and subthemes to preserve context for data synthesis. Inconsistencies in data extraction between VH and AY/SA were resolved through discussion.
Critical appraisal
Quality of included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Tools as they incorporate appraisal checklists for different study designs.30 VH and AY/SA independently rated each criterion of the relevant checklist for each included study, and discrepancies were resolved through discussion. As JBI checklists for different study types have a different number of criteria, we summarised study quality using a similar approach taken in a previous systematic review.31 The total score for each study was calculated as a percentage and classified as ‘low’ (0%–45%), ‘fair’ (≥46%–69%) or ‘high’ quality (≥70%).31 Studies were not excluded on the basis of low quality.
Data analysis and synthesis
Due to heterogeneity of study outcomes we were unable to statistically pool data. Therefore, we performed a narrative synthesis. We used a convergent segregated approach whereby quantitative and qualitative data were analysed separately before being thematically synthesised.32
Quantitative data were initially organised according to the PCP factor label given in included studies. Qualitative data were manually coded for PCPs’ perceptions of PCP factors on decisions to investigate cancer that could potentially be grouped into descriptive categories.
Definitions and/or descriptions of PCP factors from quantitative and qualitative studies were compared to determine the similarity of identified constructs. Data for each construct was iteratively grouped and checked by FW/SA until categories of PCP factors became clear. Final labels for each PCP factor were refined following team consensus meetings (table 1).
Quantitative and qualitative findings for each PCP factor were then separately examined. The direction and magnitude of effect (for quantitative data) and PCPs’ perceptions (for qualitative data) of PCP factors, were summarised in textual format for every PCP factor. Quantitative and qualitative textual summaries were juxtaposed and subsequently combined into a new descriptive narrative that encapsulated findings from each study.33
Finally, PCP factors were organised into over-arching themes according to the extent to which they were deemed to be modifiable or non-modifiable. Modifiable factors were factors considered to be susceptible to individual control or being changed with intervention. Non-modifiable factors were viewed to be outside the purview of individual control and less susceptible to adjustment. Findings for each PCP factor were interpreted in the context of the methodological limitations of each study from the critical appraisal. Only PCP factors for which there were a minimum of two studies were synthesised.
Description of PCP factors identified from included studies
Patient and public involvement
This systematic review was undertaken as part of the CanTest Collaborative research programme funded by Cancer Research UK. This programme involves close collaboration with a panel of PPI representatives whose views informed the design of this study, data analysis and data interpretation.
Results
Search results
The search yielded a total of 7938 studies. After deduplication, titles and abstracts of 4135 studies were screened; 3721 did not meet inclusion criteria and were excluded. We reviewed the full text of 82 studies retrieved from the search, with a further nine identified through hand-searching reference lists of included articles. 29 studies (19 quantitative and 10 qualitative) met inclusion criteria and were included in the final synthesis (see figure 1).

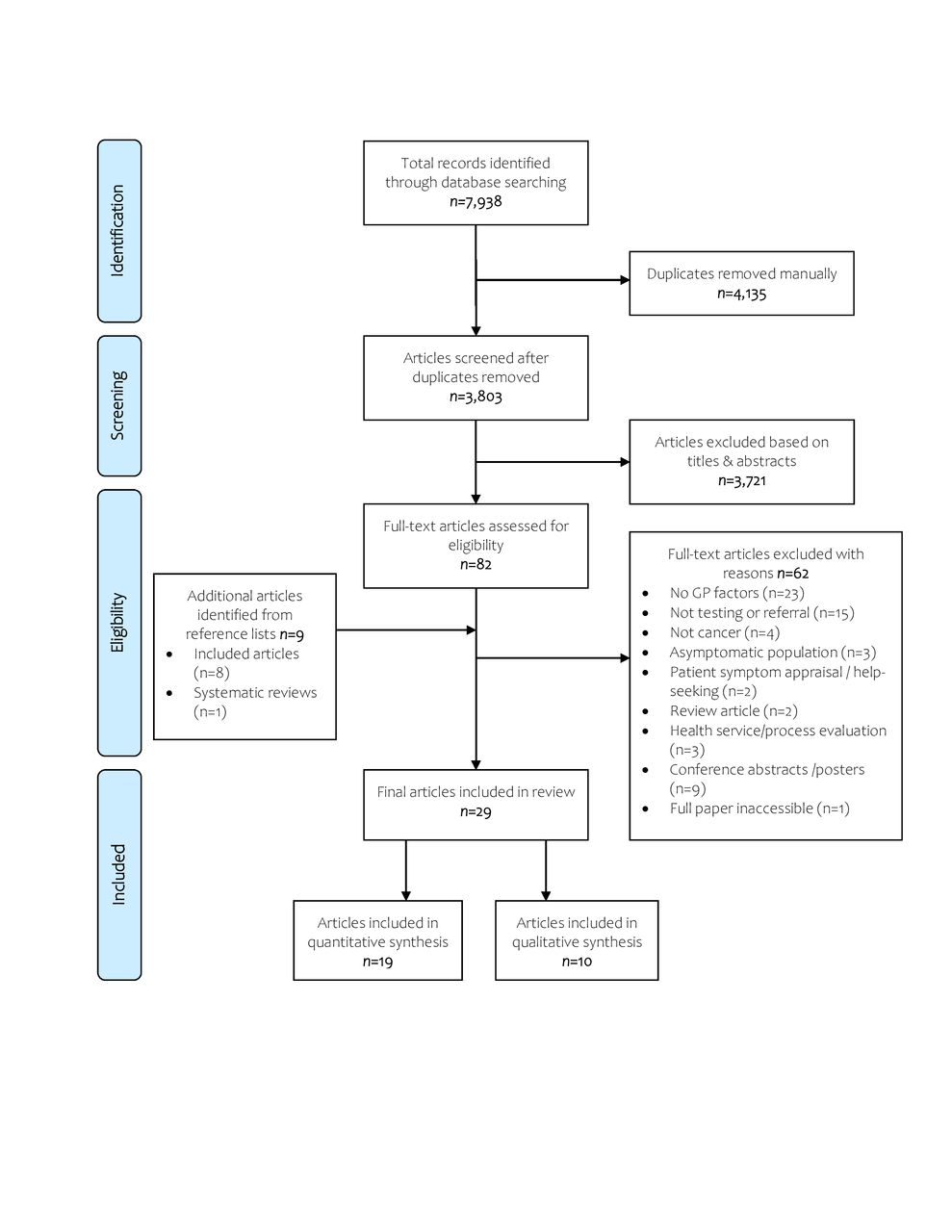{kind=link}
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The included quantitative studies consisted of 13 cross-sectional studies25 34–45 and two experimental studies,23 46 of which 11 used vignette-based methods;23 25 35–39 42 44–46 three were prospective cohort studies,47–49 and one was a retrospective cohort study (online supplemental material 2).49 Qualitative data came from five interview studies,50–54 two focus group studies,55 56 two cross-sectional survey studies57 58 and one retrospective cohort of free-text primary care consultation data.59 Of these 29 included studies, 11 were conducted in the UK,23 25 34 37 43 44 50 51 54 55 57 six in Denmark,40 41 45 47 60 61 two across 20 countries within the European Union,39 58 two each in Australia,35 46 the USA,36 38 and Norway,49 53 and one each in the Netherlands,59 Sweden,52 Spain,56 and across Australia and the UK.42 Together, studies reflected a total of 10 300 PCPs (8000 from quantitative studies, 2300 from qualitative studies) and testing and referral decisions for 15 100 patients.
Supplemental material
The most common diagnostic action evaluated was urgent referral37 41–43 51 54 55 57 60 or direct referral to diagnostic testing centres,34 40 45 50 imaging tests,48 or other specialty services.35 46 Additional investigations included use of appropriate investigations for the cancer,23 25 36 38 39 any diagnostic action,47 49 50 52 53 58 or referral in general.56 59 Testing and referral decisions were mainly made in the context of symptoms generally suggestive of the target cancer(s).35 36 38 41 47 48 55 58–60The remaining studies examined decision making for symptoms at high-,46 49 low-,25 34 39 40 50 and mixed-risk of cancer (based on the positive predictive value of symptoms in national guidelines),23 37 42 44 or did not provide details of symptomatic context.43 45 51–54 56 57 Cancers studied were colorectal,36 37 42 43 52 54 55 59 lung,23 44 46 55 61 ovarian,38 60 a mixture of cancers,25 35 39–41 58 and any cancer.34 45 47 50 51 53 56 57
Quality of included studies
Twelve studies were assessed as high quality,23 25 34 36 37 39 45–47 49 50 53 11 were fair quality,35 38 40 41 44 48 51 52 55 59 60 and six were low quality (online supplemental material 2).42 43 54 56–58
The main quality issues for quantitative studies related to poor reporting of sample characteristics,40 41 43 47–49 60 failure to identify or adjust for confounding,38 42 43 49 and hindsight bias due to knowledge of the diagnosis at the point of assessment of PCP factors.40 41 49 There were also concerns about several studies using vignettes which were not adequately realistic of patient cases seen in clinical practice and lacked evidence of validation.25 35 37 46 57 Qualitative studies were limited by insufficient evidence of researcher reflexivity and positionality,50–55 57 59 suboptimal presentation of participants’ voices55 56 59 and failure to indicate whether ethical permissions were obtained or waived.56
Recall and social desirability bias was also a concern across study types where assessment of the exposure by PCPs was examined retrospectively,40 41 49 or based on PCPs reflections of their clinical practice.50–54
PCP factors
A total of 11 PCP factors were identified (table 1). Non-modifiable PCP factors comprised demographic characteristics. Modifiable PCP factors included clinical reasoning processes, dealing with uncertainty, and professional role and involvement in continuing medical education. The evidence for these 11 PCP factors is summarised below (quantitative and qualitative findings for each factor are presented separately in online supplemental materials 3 and 4, respectively).
Supplemental material
Supplemental material
Non-modifiable factors
Demographic characteristics
Sex (n=7)
Most studies suggested that female PCPs more often investigated possible cancer compared with male PCPs,37–39 46 48 though findings were predominantly descriptive. Being female was associated with increased odds of urgent specialist review for patients with a lung nodule on CT (OR 1.87, 95% CI 1.36 to 2.56, p≤0.001)46 and referral of symptoms suspicious of colorectal cancer.37 Compared with male PCPs, females more frequently recommended appropriate investigations for ovarian cancer38 and symptoms of any possible cancer,39 but these differences were not statistically significant. There was also no observable trend between PCP sex and use of investigations for lung cancer,23 48 nor was there an association with estimation of cancer risk at urgent referral.45
Age (n=5)
The effect of age on decisions to investigate possible cancer was inconclusive. In two studies in Australia/UK and the USA, younger PCPs (aged 30–39 years) were most likely to recommend specialist referral for colorectal cancer42 and request appropriate investigations for ovarian cancer.38 However, in another study conducted in the UK, younger PCPs overall used relevant investigations for lung cancer less frequently than PCPs older than 45 years.23 Odds of urgent referral increased with age in one study. PCPs 60–69 years were significantly more likely to recommend urgent referral (OR 15.4, 95% CI 4.4 to 53.8, p≤0.001) than those 30–39 years (OR 2.8, 95% CI 1.5 to 5.2, p≤0.001).42 PCPs 60 years and above tended to estimate cancer risk at referral to be higher than PCPs younger than 45 years, though this finding was non-significant.45 There was also no difference in mean age at referral between PCPs using and not using direct CT referral for lung cancer.61
Years of experience (n=10)
Evidence regarding the influence of years of experience was also mixed. Compared with those less experienced, PCPs with upwards of 10 years of experience were more likely to make a specialist referral for symptoms of ovarian35 and colorectal cancer,42 and initiate diagnostic action in general.39 PCPs trusted their clinical judgement with increasing experience and became more willing to investigate when they were suspicious of cancer, regardless of colleagues opinions of their decisions.50 52 However, one study found PCPs with less than 6 years of experience were most able to differentiate presentations at risk thresholds of 3% or more requiring urgent referral compared with PCPs with 18–36 years of experience.44 A further three studies found no observable influence of years of experience on decisions to test and refer for possible cancer.23 25 38
Modifiable factors
Clinical reasoning processes
Clinical judgement (n=7)
Clinical judgement of symptoms as suspicious or alarming consistently led to more investigations across multiple cancer sites.41 43 47 49 51 57 60 When PCPs were suspicious of cancer they were more likely to recommend imaging investigations (OR 3.95, 95% CI 2.80 to 5.57) or make a referral (OR 2.56, 95% CI 2.22 to 2.96) compared to when symptoms were interpreted as not suspicious.47 Symptoms that did not provoke suspicion60 or were interpreted as non-alarm41 were less likely to be urgently referred. PCPs had difficulty discerning the appropriateness of using urgent referral pathways when patients symptoms did not clearly match referral criteria which was perceived not to accommodate individual clinical judgement.57
‘Gut feeling’ (n=7)
The presence of ‘gut feeling’ did not lead to increased referral rates, but doubled the odds of a cancer diagnosis within 6-months when PCPs decided to act on this feeling.34 40 ‘Gut feeling’ was perceived to facilitate management of symptoms that were not definitive55 57 and become more accurate with experience.50 55 Justifying referral of patients with concerning symptoms not meeting referral criteria on the basis of ‘gut feeling’ was challenging as it was perceived to not be sufficient indication for referral among hospital specialists.50 53 57 PCPs’ assessment of cancer risk at referral was not influenced by ‘gut feeling’.45
First diagnostic impressions (n=2)
In one vignette study, PCPs whose first diagnostic impressions were of possible cancer were more likely to recommend investigation than PCPs whose initial impressions did not include cancer (OR 1.98, 95% CI 1.10 to 3.57, p≤0.01).25 Further, odds of a cancer diagnosis doubled when PCPs verbalised cancer as a possibility after reading the reason for the patients presentation compared with when they did not mention cancer.25 Failure of PCPs to reconsider initial diagnostic hypotheses could herald suboptimal testing strategies and delayed colorectal cancer diagnosis. False reassurance from positive response to medication, intermittent symptoms, misleading test results, and comorbidity were reported to contribute to failure of PCPs to consider alternative diagnostic hypotheses.59
Assessment of cancer risk (n=2)
The relationship between PCPs’ assessment of cancer risk and use of investigations was unclear. In a prospective cross-sectional study, higher estimation of cancer risk did not result in higher referral rates but did lead to a concomitant increase in the likelihood of a cancer diagnosis.40 Findings from a Danish vignette survey suggested that PCPs overestimate cancer risk as approximately one-third of PCPs' anticipated cancer risk at referral for a hypothetical patient to exceed 50%.45
Dealing with uncertainty
Attitude to uncertainty and risk (n=4)
Findings for this PCP factor were inconsistent. Survey responses on the Tolerance for Uncertainty scale suggested that PCPs most tolerant of uncertainty were the least confident in their assessment about the possibility of an underlying cancer at urgent referral compared to PCPs with the lowest tolerance for uncertainty.45 PCP responses to the Physician Risk Attitude scale and 'levels of anxiety due to uncertainty' and 'concern about bad outcome' domains in the Physician Reaction to Uncertainty scale, was not associated with assessment of cancer risk at referral.45 Another study found that decisions to test for ovarian cancer were not affected by PCPs attitude to risk.38 Diagnostic uncertainty was viewed as integral to clinical practice,53 but could lead younger doctors who were less comfortable with uncertainty to investigate unnecessarily.51 53
Fear of malpractice (n=4)
The potential influence of fear of malpractice diverged by study type. In two quantitative studies, PCPs concerns about malpractice did not influence selection of tests for ovarian cancer,38 nor did PCPs consider fear of malpractice to influence their decisions to use urgent referral pathways.43 In contrast, qualitative studies suggested that previous experience of complaints from patients or colleagues for suboptimal testing decisions could affect PCPs future diagnostic approach.56 Defensive testing was considered the only strategy available to PCPs concerned about litigation for reassuring patients and protecting themselves medicolegally.50
Professional role and involvement in continuing medical education
Attitude to role as gatekeeper (n=3)
Evidence for this PCP factor was predominantly descriptive. PCPs believed their role was to act in the best interests of the patient, advocate for patients healthcare needs with hospital specialists,51 and make appropriate management decisions.45 PCPs' attitudes were not associated with their assessment of cancer risk at referral.45 In their role as gatekeeper, PCPs had mixed encounters with hospital specialists when trying to make a referral on the basis of ‘gut feeling’. They described productive dialogue with specialists via telephone ahead of a referral, but were reluctant to write ‘gut feeling’ into the referral letter.50
Participation in continued medical education (n=4)
In one US vignette study, PCPs involved in clinical teaching were 1.04-fold more likely to use relevant tests for ovarian cancer compared with PCPs not participating in educational activities.38 Across three interview studies, PCPs wanted more educational opportunities to better differentiate symptoms that could be due to cancer.51 54 58 Frequent training on the latest evidence regarding the predictive value of symptoms for cancer was viewed as important51 as lack of clarity about when to suspect cancer was believed to have contributed to incorrect non-referral of patients in their practice.54 58
Discussion
Summary of principal findings
We identified a number of non-modifiable and modifiable PCP factors potentially influencing testing and referral decisions for cancer. Of the PCP factors deemed modifiable, we found most evidence for ‘clinical judgement’ and ‘gut feeling’. PCP judgement of symptoms as suspicious or ‘alarm’ led to more investigations for possible cancer than symptoms judged to be non-alarm. The presence of ‘gut feeling’ at referral increased the likelihood of a subsequent cancer diagnosis. PCPs relied on ‘gut feeling’ to guide decisions to investigate non-specific symptoms. Patients’ symptoms could not always be easily reconciled with clinical guidelines, making it difficult for PCPs to determine the appropriateness of referral. Clinical guidelines offered limited scope for PCPs to act on ‘gut feeling’ or clinical judgement when symptoms did not fit referral criteria. Female PCPs tended to investigate cancer more than male PCPs. The effect of years of experience was inconclusive, but more experience was perceived by PCPs to improve the reliability of ‘gut feeling’. The evidence for the remaining PCP factors was insufficient to derive clear conclusions.
Strengths and limitations
To date, research evaluating possible reasons for inconsistencies in PCPs use of suspected cancer referral pathways20 have primarily focused on the influence of patient,62 practice16 63 and health-system factors.64 65 By summarising quantitative and qualitative evidence for PCP factors, this review builds on existing knowledge regarding the range of factors affecting PCPs decisions to investigate cancer and highlights PCPs’ perspectives regarding the potential value of those factors in clinical practice. Our search strategy covered a variety of terms for PCP factors increasing the likelihood that all relevant studies were identified. We used a transparent approach to derive PCP factors which could be useful for developing uniform definitions of these factors that can be applied in future primary care cancer research.
However, this study does have some limitations. While we attempted to synthesise data for PCP factors representing similar constructs, heterogeneity in labelling of PCP factors between studies, which were seldom defined, may have affected construct validity. For example, studies reporting clinical suspicion and 'gut feeling' did not always adequately define these terms or describe how they were assessed, making it difficult to determine which construct was actually measured. Additionally, we did not limit evaluation to PCP factors assessed as a primary or secondary outcome, so findings for years of experience, age and sex, in particular, should be interpreted with some caution. These factors were typically examined ad hoc and may not be sufficiently powered to detect a true relationship with testing and referral decisions. While clinical decision making occurs in the context of the patient agenda and wider health system,66 67 a number of included studies did not adjust analyses for confounding from patient or health system factors, potentially obscuring the true relationship of PCP factors (notably those relating to PCP demographic characteristics, ‘clinical judgement’, attitude to uncertainty/risk and fear of malpractice) with testing and referral decisions.
Dichotomising factors as modifiable or non-modifiable may obfuscate the complex and dynamic mechanisms through which PCP factors influence decision making, and the extent to which these factors may be modifiable in practice. For example, PCPs’ interpretation of symptoms as ‘alarm’ or non-serious (ie, ‘clinical judgement’) may be due to variations in PCP knowledge of referral criteria for suspected cancer or application of cognitive shortcuts (eg, availability heuristic, overconfidence). Although there is scope for these respective components to be improved through interventions such as clinical updates or metacognitive practices that highlight the impact of errors in cognition on patient care,68–70 knowledge of clinical guidelines may be more susceptible to adjustment than PCPs use of heuristics which is influenced by personality traits that are more difficult to modify.71 ‘Gut feeling’ is associated with empathy72 and underpinned by clinical knowledge and experience.73 74 Thus, the ability of PCPs to access and leverage 'gut feeling' in interventions for enhancing empathy75 may be more instinctive to some PCPs than others. Though years of experience is not modifiable, clinical experience may be more important and mutable through simulated diagnostic experiences that increase exposure to presentations that could be due to cancer.76
The overall conclusiveness of our findings is also limited by methodological weaknesses of studies using retrospective (eg, interview, medical record review) methods that are susceptible to recall, social desirability and hindsight bias.
Comparison with existing literature
That PCPs were less likely to investigate symptoms judged to be ‘non-alarm’ comports with existing literature which reports longer diagnostic intervals for lower risk symptoms not meeting urgent referral criteria across cancer sites77 and non-investigation or delayed investigation of patients with gynaecological cancers presenting to primary care with non-specific symptoms.78 A recent systematic review and meta-analysis examining the influence of ‘gut feeling’ in the diagnosis of cancer similarly found ‘gut feeling’ to be highly predictive of cancer (OR 4.24, 95% CI 2.26 to 7.94) and linked with PCP experience.74 In the same review ‘gut feeling’ also led to more referrals74 which was not supported by our findings. This inconsistency may be due (in part) to differing interpretations of PCP factors constituting 'clinical judgement' and ‘gut feeling’ (for example, we deemed clinical suspicion in two similarly included studies47 49 to reflect 'clinical judgement' rather than ‘gut feeling’). Qualitative studies of cancer patients symptom appraisal suggest patients use vocabulary when communicating their symptoms that differs from biomedical terms familiar to PCPs,79–81 which may explicate the difficulties PCPs experienced reconciling patients’ symptoms with referral criteria. A cross-sectional observational study of English practices found that practices with majority male PCPs were less likely to urgently refer for suspected cancer,82 which accords with our finding that female PCPs were more inclined to investigate patients with symptoms of possible cancer.
Unanswered questions and future research
Future research in this area would benefit from standardised definitions and reporting of PCP factors. In the UK, the amalgam ‘clinical suspicion/gut feeling’ is indicated for expedited referral to non-specific symptom pathways, and NICE NG12 (2015)11 urgent referral criteria recommends clinical judgement is used when making appropriate testing decisions.11 34 However, the extent to which 'clinical suspicion' or 'clinical judgement' (both assessed as ‘clinical judgement’ in this review) and ‘gut feeling’ reflect distinct or overlapping constructs is unclear. Research is needed that elucidates how PCPs appraise symptoms as suspicious or non-suspicious to determine patient eligibility for referral. Consideration should be given to the subsequent impact on decisions to investigate possible cancer when symptoms are not described in biomedical terms. PCP factors are multidimensional and comprise contributory components that may be more modifiable than others. Disentangling the potential involvement of such components for ‘clinical judgement’ and ‘gut feeling’ could foster more understanding of these constructs and facilitate identification of factors to target in future interventions. Testing and referral decisions may be driven by aspects of PCP gender as opposed to sex, but empirical evidence for the effect of sociocultural vs biological factors is lacking.83 Since suboptimal decisions to investigate cancer are likely precipitated by a combination of factors,84 future research should examine possible interactions between PCP factors (and patient and health system factors). This is pertinent given the potential for reverse causality among some PCP factors.
Implications for policy and practice
As the majority of studies in this review were conducted in European countries, our findings have most applicability for countries where PCPs are gatekeepers to specialty services. Our findings have implications for improving the management of symptomatic patients with cancer in general rather than a specific cancer type. This is of clinical import as patients may be at lower risk of an individual cancer but higher risk of an underlying cancer overall.34 85 In the absence of clinical judgement of symptoms as ‘alarm’ or ‘gut feeling’, PCPs may not investigate patients in a timely manner. Novel pathways for non-specific symptoms (eg, SCAN pathway in Oxford86) that are currently in development in the UK, will be important for circumventing perceived barriers to acting on 'clinical judgement' or ‘gut feeling’ for symptoms not meeting urgent referral criteria. However, supplementary strategies are needed that support PCPs to recognise and investigate patients with non-alarm and non-specific symptoms that need referral. The challenge for policy-makers will be to determine how to enhance the utility of clinical guidelines for investigation of possible cancer by operationalising clinical suspicion/judgement and ‘gut feeling’, and ensuring recommendations refrain from reinforcing language siloes between patients and PCPs that may create opportunities for suboptimal testing decisions and diagnostic delay.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All research data supporting this publication are provided within this article.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sammerriel
Contributors VH, MT, JE and FMW designed the study; VH developed and performed the search; VH, AY and SWDM screened the search results; VH, AY and SA extracted the data; VH drafted the manuscript with input from JU-S and FMW; all authors critically assessed and contributed to manuscript revisions. FMW is guarantor of this work.
Funding This review is supported by the CanTest Collaborative which is funded by Cancer Research UK (C8640/A23385), where VH is a PhD student, SWDM is a Clinical Research Fellow, FMW is Director, and MT and JE are associate directors. SA is supported by Cancer Research UK grants (C12292/A20861).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.