Article Text

Abstract
Introduction Laparoscopic distal gastrectomy (LDG) is regarded as a standard treatment for patients with clinical stage I–III gastric cancer. With the popularisation of the Da Vinci robotic system in the 21st century, robotic distal gastrectomy has been increasingly applied, and its potential advantages over LDG have been proved by several studies. Intraperitoneal anastomosis is a hot topic in research as it highlights the superiority of minimally invasive surgery and is safe and feasible. We intend to conduct this randomised clinical trial to focus on short-term outcomes and quality of life (QOL) in totally laparoscopic distal gastrectomy (TLDG) and totally robotic distal gastrectomy (TRDG) for patients with clinical stage I–III gastric cancer.
Methods and analysis This study is a prospective, multi-institutional, open-label randomised clinical trial that will recruit 722 patients with a 1:1 ratio (361 patients in the TLDG group and 361 patients in the TRDG group) from eight large-scale gastrointestinal medical centres in China. The primary endpoint is 30-day postoperative morbidity. The secondary endpoints include QOL, 30-day severe postoperative morbidity and mortality, anastomotic-related complication rate, conversion to open surgery rate, intraoperative and postoperative indicators, operative and total costs during hospitalisation, 1-year overall survival and disease-free survival. QOL is determined by the The European Organization for Reasearch and Treatment of Cancer Quality of Life Questionnare-Core 30 and Stomach22 (EORTC QLQ-C30 and STO22) questionnaires which are completed before surgery and 1, 3, 6 months, and 1 year after surgery. χ2 test will be used for the primary endpoint, while analysis of covariance will be used to compare the overall changes of QOL between the two groups.
Ethics and dissemination This trial was approved by the Ethics Committee of the Chinese PLA General Hospital. The trial’s results will be disseminated via peer-reviewed scientific journals and conference presentations.
Trial registration number ChiCTR2000032670.
- gastrointestinal tumours
- adult surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This trial is one of the few multi-institutional Randomized clinical trial (RCT) studies that focus on the difference in short-term outcomes and quality of life (QOL) between totally laparoscopic distal gastrectomy (TLDG) and totally robotic distal gastrectomy (TRDG) for patients with clinical stage I–III gastric cancer.
We use 30-day postoperative morbidity as the primary endpoint to compare short-term outcomes between TLDG and TRDG.
Clavien-Dindo classification is applied to define severe extent of complications and the type of complications is in accordance with the definitions of the Gastrectomy Complications Consensus Group.
We evaluate QOL quantified by EORTC-QLQC30 and STO22 questionnaires.
The main limitation in this study is that it will be relatively difficult to finish recruitment quickly and bring potential selection bias because the extra cost of robotic surgery is not covered by the Chinese national healthcare system.
Background
Gastric cancer is one of the most common malignant tumours and has high morbidity and mortality.1 Surgery is regarded as the most effective means to cure gastric cancer. Since Kitano et al2 reported the world’s first laparoscopic gastrectomy in 1994, minimally invasive surgery has rapidly developed and gradually matured because of its unique advantages, such as a minimal incision, faster recovery and better survival benefit.
China is a country with a high incidence of gastric cancer.3 The CLASS-01 study4 resulted in a significant breakthrough because its conclusion proved the safety and feasibility of laparoscopic distal gastrectomy (LDG) and the non-inferiority on the 3-year disease-free survival (DFS) of LDG compared with open distal gastrectomy for locally advanced gastric cancer in China. The KLASS-01 and JCOG-0912 studies also reached similar conclusions for early gastric cancer.5 6 These results show high-grade evidence that LDG can become a standard surgical option for patients with clinical stage I–III gastric cancer.
The Da Vinci robotic surgical system is a newly developed technique in the field of minimally invasive surgery. The application of robotic gastrectomy has rapidly increased, especially in East Asia, since it was first described in 2002.7 The robotic system can provide a wider operative field via three-dimensional visualisation, a stable operation platform, a flexible wrist swivel device, the ability to use remote control based on 5G, etc. Some studies reported that robotic distal gastrectomy (RDG) had less blood loss, retrieved more lymph nodes, lower rate of postoperative blood transfusion, lower intra-abdominal infectious complications rates, faster postoperative recovery and comparable short-term and long-term oncological outcomes compared with LDG regardless of early or advanced gastric cancer.8–11 Recently, Lu’s RCT study demonstrated that RDG had lower postoperative complication rate compared with LDG for clinical stage I–III patients.12 These results indicate the potential superiority of RDG. However, the currently available evidence on robotic gastrectomy is still limited, which need more evidence-based studies to explore the effect of RDG.
With the development of laparoscopic instrumentation and surgical skill, many surgeons have adopted intracorporeal anastomosis that can maximise the advantages of minimally invasive surgery. Based on laparoscopic or robotic technology, intracorporeal anastomosis seems relatively easy to perform and has shown satisfactory outcomes, such as reduced surgical injury and a shorter incision length. For anastomotic complication that surgeons are mostly concerned, no significant difference was found between intracorporeal and extracorporeal anastomosis in previous studies.13 14 In addition, intracorporeal anastomosis is feasible in obese patients.15 These merits have drawn the attention of a growing number of surgeons who apply this technique in RDG and LDG, that is, totally robotic distal gastrectomy (TRDG) and totally laparoscopic distal gastrectomy (TLDG).
At present, the safety and feasibility of TLDG and TRDG has been proven.16 However, no prospective study has compared short-term outcomes and quality of life (QOL) for TLDG and TRDG with intracorporeal anastomosis for clinical stage I–III patients to our knowledge. To evaluate how different surgical approaches affect short-term outcomes and QOL for patients with gastric cancer, it is necessary to carry out this multi-institutional randomised controlled trial. This study will provide high-grade evidence for reasonable clinical applications.
Methods and analysis
Trial design
This study is a prospective, multi-institutional, open-label randomised clinical trial using a parallel-arm design which will recruit 722 patients (361 patients in the TLDG group and 361 patients in the TRDG group) from eight large-scale gastrointestinal medical centres in China. Table 1 lists the medical centres involved in our study, and an explicit flow chart is shown in figure 1. This study aims to evaluate short-term outcomes and QOL for TLDG and TRDG for patients with clinical stage I–III gastric cancer. The study is designed on the hypothesis that TRDG is superior to TLDG in the aspect of the short-term outcome for patients with cTNM (tumour, node, metastases) I–III gastric cancer. Approximately 18 surgeons who are qualified to perform robotic surgery will participate in this study. They have rich experience with robotic and laparoscopic gastrectomy and perform over 50 TLDG and 50 TRDG before, which has crossed learning curve for the TRDG and TLDG operations.17 18 All patients will sign the consent form so that they can be recruited for this study.

Flowchart of the study.
Main medical centre that participated in clinical trial
Eligibility criteria
Inclusion criteria
Pathologically confirmed gastric adenocarcinoma by preoperative gastroendoscopy before the operation.
Tumours located in the middle or lower one-third stomach that need to undergo distal gastrectomy.
Age between 18 and 80 years.
Clinical tumour stage I–III with cT1-4aN0-3M0, according to the Eighth Edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual (TNM AJCC-8th tumour staging).19 We will use endoscopic ultrasonography (EUS) plus multidetector-enhanced CT to detect tumour invasion depth and number of suspicious metastatic lymph nodes.
ASA (American Society of Anaesthesiologists) score: Grade I or II.
Eastern Cooperative Oncology Group (ECOG) score: 0 or 1.
Patient consent obtained.
Exclusion criteria
Those with severe mental disorders, which are defined as the mental disorder which patients’ social adaptation and other functions are seriously impaired, and they cannot fully understand their health status or objective reality, or they cannot deal with their own things, including cerebral organ psychosis, schizophrenia, affective psychosis, mental retardation, schizoaffective psychosis and paranoid psychosis.
Women who are pregnant or breast feeding.
History of abdominal surgery (except for laparoscopic cholecystectomy).
History of gastrectomy, endoscopic submucosal dissection (ESD),endoscopic mucosal resection (EMR) or stump gastric cancer.
History of unstable angina pectoris or myocardial infarction within the past 6 months; cardiac functional grade: New York Heart Association (NYHA) classification ≥Grade III.
Chemotherapy or radiotherapy before the operation.
History of other malignant tumours within the past 5 years (except for papillary thyroid carcinoma).
Diameter of perigastric lymph nodes over 3 cm based on preoperative abdominal CT or Positron Emission Tomography-Computed Tomography (PET-CT).
Need to combine other organ resection because of tumour aggression.
Severe respiratory disease (forced expiratory volume in one second <50%).
Accepted continuous steroid therapy 1 month before this study.
Randomisation and blinding
Patients will be enrolled by the oncologists on the team. All patients enrolled in this study will conform to the inclusion and exclusion criteria. Data such as age, sex, Body Mass Index (BMI), ECOG score, ASA score and other baseline characteristics will be recorded in a previously designed form and sent to the central data centre before randomisation. Then, the data manager will acquire a random number from a website-based randomisation system that uses the central dynamic and stratified method with the stratification factors including participating site (eight hospitals), patient age (≤60 or >60 years), sex (female or male), BMI (<25 or ≥25 kg/m2) and clinical TNM stage (I or II or III). Eligible patients will be randomised into the TLDG or TRDG group with a 1:1 ratio. Because it is difficult to ensure blinding between the surgeons and patients, the group allocation will not be concealed. The scientific nurses, whose assignment is to record the patients’ postoperative index, and pathologists will be blinded.
Treatments
The principles and surgical procedures for TLDG and TRDG are based on the Japanese Gastric Cancer Treatment Guidelines 2018 (V. 5) and CLASS-01 standard protocol.20 21 The explicit treatments are as follows:
Trocar placement and abdominal exploration
A longitudinal incision approximately 1 cm long is made below the umbilicus. Then, the skin and lift abdominal wall are cut so that a pneumoperitoneum needle can be inserted into the abdominal cavity. After establishing pneumoperitoneum with 12 mm Hg of pressure of carbon dioxide, the pneumoperitoneum needle is extracted and placed into a 10 mm trocar for abdominal exploration. Under TV monitoring, two 5 mm trocars are placed in the right abdomen, and 12 and 5 mm trocars are placed in the left upper abdomen trocar. In the TRDG group, the Da Vinci Xi surgical system with four robotic arms will be used as a replacement for laparoscopy. Before the operation, the robotic arm will be installed and adjusted to the proper situation by the surgical team. The other surgical principles and protocols are identical between the TLDG and TRDG groups.
Lymph node dissection
According to the definition of the Japanese Gastric Cancer Treatment Guidelines 2018, the extent of D1 lymph node dissection contains No. 1, 3, 4sb, 4d, 5, 6 and 7 lymph nodes. The extent of D1+ or D2 lymph node dissection will include No. 8a and 9 or No. 8a, 9, 11p and 12a lymph nodes based on the D1 dissection. How to select the appropriate lymph node dissection area depends on the clinical tumour stage. The explicit extent of lymph nodes dissection is presented in table 2. Taking D2 lymph node dissection as an example, the specific operating steps are as follows: The gastrocolic ligament along the superior border of the transverse colon is cut, and the lesser omentum sac is entered. The ultrasound knife is turned left to the splenic and colonic ligament area, the left gastroepiploic vein and artery are detached, and then the No. 4sb lymph nodes are dissected. Next, the surgeons proceed directly to the hepatocolic ligament where they expose the head of the pancreas, strip the anterior lobe of the transverse mesentery and detach the right gastroepiploic artery and gastrocolic trunk so that the No. 4d lymph nodes can be easily dissected. The stomach is pulled to the left upper abdomen, and the area of the gastric and pancreatic wall are exposed so that the left gastric artery and vein can be found and ligated. The No. 7 lymph nodes are then dissected. Next, the coeliac trunk, proximal common hepatic artery and proximal splenic artery are dissociated, and the No. 8a, 9 and 11p lymph nodes are dissected. The gastric omentum is cut off, and the proper hepatic artery, right gastric artery and distal part of the common hepatic artery next to the inferior margin of the hepatic venous ligament are exposed. The right gastric artery is cut and ligated, and the No. 5 and 12a lymph nodes are cleaned. The stomach is pulled down to the right, the cardia is exposed, and the No. 1 and 3 lymph nodes are dissected along the lesser curvature.
The extent of lymph nodes dissection
Range of tumour resection
To obtain a better prognosis, a sufficient tumour edge should be ensured by the surgeons before specimen resection. The range of tumour resection is also in accordance with the Japanese Gastric Cancer Treatment Guidelines 2018.20 For T1 tumours, 2 cm is sufficient for the gross resection margin. For T2 or deeper tumours with an expansive growth pattern, we stipulate that the proximal end of the localised tumour has a margin of more than 3 cm for type 1/2 tumours and of more than 5 cm for type 3/4 tumours. If the tumour cutting edge cannot meet the requirement and there is doubt whether the margin will have positive results, intraoperative frozen pathology of the cutting edge needs to be performed to exclude positive results.
Gastrointestinal reconstruction
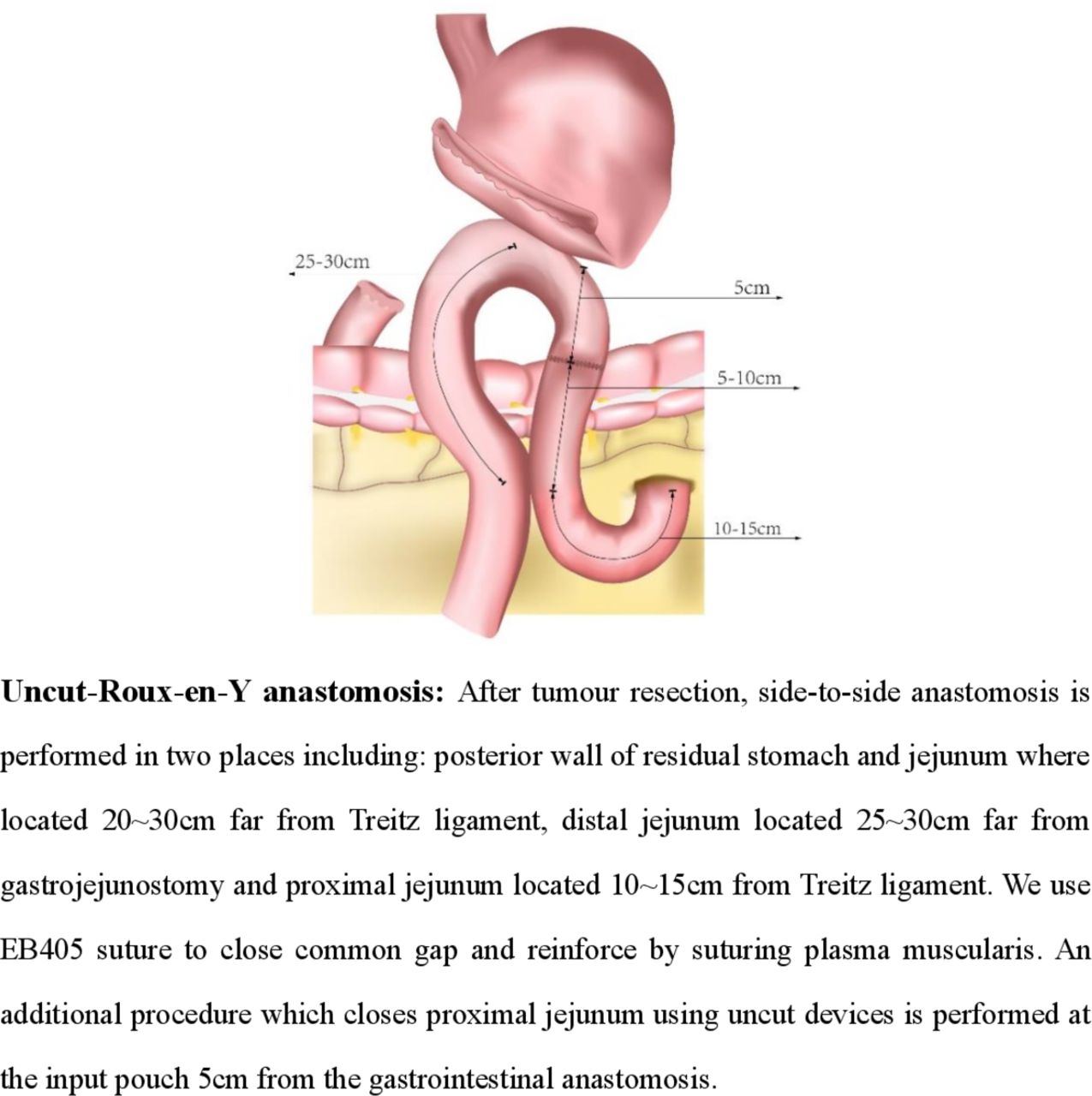
After tumour resection, gastrointestinal reconstruction should be performed by intracorporeal anastomosis. We stipulate to perform uncut Roux-en-Y reconstruction after tumour resection because its safety and good postoperative recovery has been proven by previous study,22 and it has been adopted as the regular reconstruction method in all medical centres participating in our study. The protocol for intracorporeal reconstruction refers to guidelines established by the gastrointestinal surgery group from the surgical branch of the Chinese Medical Association,23 and a schematic diagram of gastrointestinal anastomosis is shown in figure 2. A less than 5 cm longitudinal incision at the epigastrium can be used for removing specimens and for assistive poles in uncut Roux-en-Y reconstructions.
{kind=link}
{kind=link}
Schematic diagram of gastrointestinal anastomosis.
Scheme of postoperative recovery
The application of the enhanced recovery after surgery (ERAS) has widely gained acceptance after gastrointestinal surgery. Chinese surgeons gradually paid more attention to the important status of ERAS and drafted a consensus and guideline aiming to unify the standard criteria.24 In this study, postoperative protocol in hospitalisation is in accordance with this guideline and consensus of participants in this study which is illustrated in table 3, including the following: (1) Nasogastric tube: It is recommended to pull it out in postoperative day 1 (POD1). (2) Abdominal drainage tube: It can be removed in POD3 when drainage fluid is clear and <100 mL/day, or anastomotic status is good, or no abdominal infection is found. (3) Urinary catheter: It should be removed in POD1. (4) Oral feeding: We stipulate that patients can acquire clear fluid diet in POD1-2, semiliquid diet in POD3–4 and soft blended diet in POD5 if tolerable, and then gradually transit to normal diet based on the premise of patient’s tolerance and no severe complication (including anastomosis leakage, ileus, high risk of gastroplegia, etc). (5) Movement: We encourage patients early ambulation last for 1 hour/day in POD1 and make appropriate scheme of movement. The time of ambulation should properly expend based on patients’ status and need 4 hours/day in POD7. (6) Discharge: Patients could be discharged from hospital in POD7 accorded with discharged criteria (without postoperative complication and primary disease that needs current intervention).
ERAS pathway after TLDG and TRDG
Outcomes
The primary endpoint is 30-day postoperative morbidity, including anastomosis-related complications (bleeding, leakage or stenosis), duodenal stump leakage, wound-related complications (fat liquefaction, hernia, infection), ileus, intra-abdominal bleeding, gastric paralysis, pancreatic fistula, lymphorrhagia, etc. Complications related to other organs, such as respiratory, cerebrovascular, cardiovascular, renal or hepatic disease, should also be recorded. The definition of complications after gastrectomy conforms to guideline of the Gastrectomy Complications Consensus Group.25 The level of severity of complications is in accordance with the Clavien-Dindo classification system,26 which has been widely used in similar clinical studies.4–6
The secondary endpoints are mentioned below. First is QOL, which has been quantified by Chinese versions of the EORTC QLQ-C30 and STO22 questionnaires.27 The EORTC QLQ-C30 questionnaire has 30 items that can be divided into 15 domains, including five functional domains (physical, role, cognitive, emotional and social), three symptomatic domains (fatigue, pain, and nausea and vomiting), six additional symptomatic domains (dyspnoea, appetite loss, sleep disturbance, constipation and diarrhoea) and one global-health domain. The EORTC QLQ-STO22 questionnaire is specially designed for patients with gastric cancer. It contains five symptomatic domains (pain, dysphagia, reflux, eating restrictions and anxiety) and four additional domains (dry mouth, body image, taste problems and hair loss). The two questionnaires mentioned above will be completed by patients and collected by data managers before surgery and 1 month, 3 months, half a year and 1 year after surgery. All individual scores will be added together and transferred to the centesimal system for unified quantification.
Meanwhile, other crucial indicators are also crucial and should be enrolled in secondary endpoints, including (1) severe 30-day postoperative morbidity: a severe grade of postoperative complication is defined as Clavien-Dindo Classification ≥IIIa; (2) 30-day postoperative mortality: all events that cause patient death during the perioperative day will be recorded; (3) rate of anastomotic-related complications: full thickness defects of gastro-jejunal, jejuno-jejunal anastomoses and duodenal stump that are defined by patients’ symptoms and imageological examinations; (4) total number of lymph nodes retrieved and the number of metastatic lymph nodes retrieved: data from pathological reports will be screened and calculated; (5) rate of conversion to open surgery: inability to continue the current surgery because of intraoperative conditions and the need to transfer to open surgery will be recorded; (6) intraoperative indicators including operation time, estimated blood loss and time of reconstruction; and (7) postoperative indicators including time of first flatus time, postoperative and total length of hospital stay; (8) operative and total costs during hospitalisation: operative costs include the cost of the operating room in relation to the operative time and all required supplies, anaesthesia, laboratory and related blood transfusion costs when required. Hospitalisation costs include the costs associated with room and board, the length of hospital stay (including intensive care, medications, blood transfusion, parenteral nutrition and radiology charge) and costs for surgical visits (programmed and emergency); (9) survival status including 1-year overall survival (OS) and 1-year disease-free survival (DFS). OS means the length of time after surgery that patient survives without death caused by any circumstance. DFS means the length of time after surgery that the patient survives without any signs or symptoms of cancer.
Sample size
We summarised previous studies that referred to the 30-day postoperative morbidity of TLDG. According to these data, the incidence rate of complications after TLDG ranged from 11.8% to 19.0%.28–30 Thus, we set the proportion in the TLDG group as 16.5%. For RDG, Lu’s RCT study showed that patients in the RDG group reduced postoperative morbidity compared with LDG group (9.2% vs 17.6%, p=0.039).12 As the incidence rates in the TRDG group range from 4.7% to 15.9% in retrospective studies16 31 32 and given the proficiency of surgeons who perform robotic gastrectomy and the reasonable cost-effectiveness of robotic surgery, 9.0% is the expected 30-day postoperative morbidity in the TRDG group in this study. PASS V.15.0 software was used to calculate sample sizes of 307 with a 1:1 ratio in each group, achieving 80% power to detect a difference between the group proportions of 7.5%. Taken together, 722 patients need to be recruited into this study (361 patients in the TLDG group and 361 patients in the TRDG group) in view of a 15% dropout rate. The test statistic used is the two-sided Z-test with unpooled variance. The significance level of the test is 0.05.
Data collection
We designed a case report form (CRF) for researchers to fill in with the information of the patients during the study. A brief subject timetable is summarised in table 4. When patients are enrolled in this study, two data management staff members and one independent quality monitor will be assigned to collect relevant data, including imageological reports (CT or PET-CT), gastric EUS reports, pathological reports, laboratory tests (complete blood count, blood biochemistry, tumour biomarkers, etc) and QOL questionnaires. Perioperative data will be registered by scientific nurses and monitored by the staff of the contract research organisation (CRO) company. After discharge, a 1-year follow-up, which contains QOL questionnaires, periodic physicals, laboratory examinations every 3 months and abdominal CT every 6 months at the outpatient department, will begin on time. Gastroscopy will be arranged for 1 year after the operation to evaluate the condition of the remnant stomach and anastomosis. For patients with pathological tumour stage II or higher, adjuvant chemotherapy with a 6-month scheme of SOX (oxaliplatin: 130 mg/m2 intravenous drip d1; S-1: 40 mg/m2 po two times per day d1–14, repeated every 21 days) or XELOX (oxaliplatin: 130 mg/m2 intravenous drip d1; capecitabine: 1000 mg/m2 po two times per day d1–14, repeated every 21 days) will be used under the guidance of experienced oncologists. The frequency of chemotherapy and adverse events during chemotherapy will be acquired by telephone call and recorded on a CRF document. We use Common Terminology Criteria for Adverse Events (CTCAE) V.4.0 formulated by National Institutes of Health National Cancer Institute to classify adverse events during the adjuvant chemotherapy.33
Schedule of enrolments, interventions and assessments
Statistical analysis
SPSS V.26.0 will be used to perform statistical analysis. Intention-to-treat analysis and per-protocol analysis will be applied to patients who are included in this study regardless of whether they finish the trial and patients who complete the trial protocol and follow-up, respectively. Continuous variables will be presented as mean±SD, and categorical variables will be presented as numbers (percentages). Data with a skewed distribution will be presented as medians (IQR). The Student’s t-test is used to demonstrate the statistical difference of the continuous variables, while the χ2 or Fisher’s exact test apply to present the difference of the categorical variables such as the primary endpoint. The Wilcoxon rank-sum test will be used for non-parametric data. Analysis of covariance with repeated measures will be used to compare the two groups of patients with respect to overall changes in their short-term QOL after the surgery. A difference in QOL>10 points in this study was considered as clinical relevant.34 To evaluate the differences in 1-year DFS and OS, Kaplan-Meier curves will be drawn and compared by log-rank test. The p value is two-sided, and we define a significant difference as when the significance level is less than 0.05.
Data monitoring, auditing and interim analysis
We invited an independent professional CRO company to manage and monitor experimental data throughout our study. Each cooperating centre has set up a data monitoring committee with three people who are not participating in this study and are specialised in data collection and supervision. When half of the patients are randomised, an interim analysis to evaluate the safety and feasibility of both surgical approaches will be conducted by an independent statistician. If we find that the 30-day morbidity in TLDG or TRDG is significantly higher than that in open distal gastrectomy which reported in previous RCT trials,4 5 the study will be halted and we will reconsider its safety discreetly.
Discussion
Distal gastrectomy operated by laparoscopic4–6 or robotic system8–11 have been regarded as the alternative surgical approaches with their safety and comparable oncological results compared with open distal gastrectomy proved by previous studies currently. Intracorporeal anastomosis after distal gastrectomy has several advantages such as less abdominal incision and faster postoperative recovery which has been performed increasingly by surgeons with abundant experience. However, whether TRDG is better than TLDG on short-term outcomes or not is still controversial because of the situation of less previous studies to our knowledge.
This study is the first non-blinding, multi-institutional randomised clinical trial that focus on the short-term outcome and QOL between RDG and LDG with intracorporeal uncut Roux-en-Y anastomosis.22 32 We aim to prospectively compare the short-term difference between TLDG and TRDG via objective and subjective indexes so that we could provide comprehensive reference for rational clinical application. Meanwhile, initial oncological results such as 1-year OS and DFS will also be presented in this trial.
Some limitations need to be declared in this clinical trial. First, we mainly focus on the disparity of short-term outcomes and QOL between TLDG and TRDG. Even though we will fulfil 1-year follow-up by telephone or outpatient department, long-term oncological outcomes are not described in this study. Further study can be conducted based on the current results. Moreover, because the extra cost of robotic surgery is not covered by the Chinese national healthcare system, it will be relatively difficult to finish recruitment quickly. Meanwhile, the level of health and fitness can be higher for patients that can financially afford robotic surgery, which could make them less prone to develop any complications. It could bring potential selection bias to the extent.
Even so, it is inevitable to conduct this study because of the increasing volume of TRDG and TLDG in China. We anticipate that this multi-institutional RCT study will take 2 years to complete and provide Chinese data and experience for clinical popularisation and lay the foundation of the further studies.
Patient and public involvement
Neither patients nor the public will be involved in the design, recruitment, measurement of outcomes or conduct of the study. We will disseminate the trial results via peer-reviewed journals and conference presentations rather than notifying every single patient. Indicators of subjective feelings, such as first flatus time and questionnaires about QOL, will be acquired by patients’ self-report.
Ethics and dissemination
This study was approved by the Chinese PLA General Hospital Ethics Committee, which conforms to Chinese legislation and the Declaration of Helsinki (approval number: S2020-257-01, approval date: 23 June 2020). Written informed consent will be obtained from all of the patients or their authorised surrogates. We have registered the study on http://www.chictr.org.cn (trial number: ChiCTR2000032670). Because of the epidemic status of COVID-19, our initial meeting was delayed unfortunately and it will be conducted on 25 April 2021. This study is planned to start on 1 May 2021 and to be completed at the end of May 2023.
Trial results will be disseminated via peer-reviewed scientific journals and conference presentations.
References
Footnotes
Contributors All authors made substantial contributions to the intellectual content of this paper. BW and LC conceived and designed this study. HC and BC are the co-first authors who participate in trial design and write this article. HX, JC, GL, ZC, WL, TX, HD and KZ participate in the design of the study and are main principals in charge of multi-institutional coordination. YT is responsible for ethical supervision.
Funding This study was funded in part by the National Key Research and Development Project (2019YFB1311505), National Natural Science Foundation of China (81773135); Outstanding Youth Specialised Foundation of Chinese PLA General Hospital (2017-JQPY-003); Health Cultivating Foundation for Capital Citizens (Z171100000417023) and Nursery Foundation of Chinese PLA General Hospital (18KMZ02). All above-mentioned foundations provided financial support on data collection and statistical analysis.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.