Article Text

Abstract
Objectives We aimed to evaluate recompensation factors among patients with decompensated cirrhosis.
Design A multicentre retrospective case–control study was conducted. Data were collected from and compared between groups of patients with recompensated and acute decompensated cirrhosis. Univariable and multivariable logistic regressions were used to select indicators associated with recompensation among patients with decompensated cirrhosis with different complications. A decision tree with 10-fold cross-validation was used to develop the model to identify patients with recompensation. We followed the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) guideline for development and reporting of the new model.
Setting The study was conducted in six tertiary public hospitals in Chongqing, China.
Participants This study included 3953 patients with decompensated cirrhosis.
Results In the total sample of included patients, there were 553 patients with recompensation and 3400 patients with acute decompensation, including 1158 patients with gastrointestinal bleeding, 1715 patients with a bacterial infection, 104 patients with hepatic encephalopathy and 423 patients with ascites. The most relevant indicator of recompensation selected by the decision tree model was albumin, with a threshold of 40 g/L. Total protein, haemoglobin, basophil percentage, alanine aminotransferase, neutrophil-to-lymphocyte ratio and diabetes were also selected to subsequently distinguish patients. The terminal nodes with a probability of recompensation was 0.89. The overall accuracy rate of the model was 0.92 (0.91–0.93), and it exhibited high specificity (86.9%) and sensitivity (92.6%).
Conclusions The occurrence of recompensated cirrhosis could be identified by albumin, total protein, haemoglobin, basophil percentage, alanine aminotransferase, neutrophil-to-lymphocyte ratio and diabetes. These simple variables may help clinicians develop a treatment plan to encourage patients with decompensated cirrhosis to recompensate.
- hepatology
- risk management
- hepatobiliary disease
Data availability statement
Data are available on reasonable request. The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The data contain more than 3000 patients with decompensated liver cirrhosis from six centres, making it the largest data sample for analysing recompensation indicators.
The indicators included in the model are available in the information systems of hospitals at all levels, which makes our indicators easier to apply in clinical and even community hospitals.
The knowledge of recompensated indicators may be useful for supporting different prevention strategies, so as to reduce the occurrence of acute decompensation.
The cut-off values of the model in other regions need further external validation.
Introduction
Patients with decompensated cirrhosis have a poor prognosis, and are more likely to undergo hospital readmissions, liver transplantation, death or hepatocellular carcinoma.1 In patients with acute decompensated cirrhosis without acute-on-chronic liver failure (ACLF), the 28-day mortality rate was 4.6%, which increased to 12.6% at 3 months, 18.3% at 6 months, and 27.6% at 1 year. In addition, acute decompensated cirrhosis occurs in up to 15% of cirrhotic patients each year.2
Fortunately, due to aetiology control, effective treatment or prevention, some patients with decompensated cirrhosis may no longer have decompensation-related complications, for a long period of time, which is considered to be ‘recompensation’.3 4 Some studies have shown that patients with decompensated cirrhosis have improved transplant-free survival rates, Child-Turcotte-Pugh and model for end-stage liver disease scores after receiving antiviral treatment.5–10 For patients with alcoholic decompensated cirrhosis listed for liver transplantation, the model for end-stage liver disease score less than 20 and serum albumin greater than or equal to 32 g/L at enrollment were independent predictors of recompensation/withdrawal from the transplant list.11
Despite that, controversies remain regarding the evaluation time, evaluation indicators, and influencing factors of recompensation. Currently, research data on the recompensation markers of decompensated cirrhosis is scant. Better identification and understanding of recompensation in patients with decompensated liver cirrhosis is very important for the design of preventive interventions that reduce the overall burden. Hence, the purpose of this study was to describe the clinical characteristics of patients with recompensation and to determine the clinical variables relevant to recompensation.
Patients and methods
Patient and public involvement statement
This was a retrospective study. Therefore, the patients and the public were not directly involved in the design and conception of this study.
Patients and definitions
This was a multicentre retrospective case–control study. Consecutive follow-up patients with decompensated cirrhosis came from six hospitals: the Second Affiliated Hospital of Chongqing Medical University, Yongchuan Hospital of Chongqing Medical University, the Third Affiliated Hospital of Chongqing Medical University, University-Town Hospital of Chongqing Medical University, the People’s Hospital of Tongliang District and the Southeast Hospital of Chongqing. Clinical data of patients treated between January 2014 and October 2019 were collected using electronic medical record systems.
The inclusion criteria were as follows: (1) diagnosis of decompensated liver cirrhosis based on clinical, biochemical, ultrasonographic and/or endoscopic findings and (2) age ≥18 years old. The exclusion criteria were as follows: (1) patients with liver cancer or other active malignancy; (2) ACLF, the diagnosis of which was based on the criteria from the consensus recommendation of the Asian Pacific Association for the Study of the Liver12; (3) congestive heart failure, chronic kidney disease or other significant chronic extrahepatic disease; (4) selective admission, such as reasons for hospitalisation that were either to perform liver biopsy, endoscopy with potential band ligation or an evaluation for liver transplantation or (5) more than 20% of the data missing for the patients or indicators.
Acute decompensated cirrhosis was defined as the rapid development of one or more major complications of liver disease, such as ascites, encephalopathy, gastrointestinal haemorrhage and bacterial infection, requiring hospitalisation.13–17 Recompensated cirrhosis was defined as clinically stable outpatients with either controlled ascites or previously treated decompensation events who were in a stable clinical state for at least 1 year.3
Ascites was recorded as the primary reason for admission if this was the sole criterion for admission and infection was absent.
Hepatic encephalopathy as characterised by altered mental status or neuropsychiatric abnormalities in the presence of liver cirrhosis after exclusion of other causes.18
Gastrointestinal bleeding was defined as the development of an upper and/or lower gastrointestinal haemorrhage of any aetiology.15
Bacterial infection was defined in cases of spontaneous bacterial peritonitis, pneumonia, cellulitis, biliary tract infection, urinary system infection and spontaneous bacteraemia.17 None of the included patients developed acute decompensated cirrhosis due to bacterial infection alone.
In the presence of more than one contributory factor, the main cause of admission was defined as follows: (1) in patients admitted with gastrointestinal bleeding in the presence of ascites, bacterial infection or hepatic encephalopathy, gastrointestinal bleeding was considered the main cause because it frequently causes bacterial infection or hepatic encephalopathy; (2) in the absence of bleeding at admission, bacterial infection was the main cause of hospitalisation and (3) in patients with hepatic encephalopathy and ascites, the main cause was the former.19 The principal cause of hospitalisation was subsequently assessed independently by two subspecialist physicians.
Treatment
Standard medical therapies were used for all patients after diagnosis, such as antiviral therapy and symptomatic and supportive therapies.
Data collection
Demographic, clinical and routine laboratory data were recorded during the first contact visit to the hospital. Demographic characteristics included age and sex. The aetiological characteristics, including hepatitis B virus (HBV)/hepatitis C virus (HCV) infection, autoimmunity and alcohol consumption, were assessed from the medical history. Clinical data included complications related to liver cirrhosis and comorbidities (such as hypertension and diabetes). Laboratory analyses included red cell counts, white cell counts, platelet counts, haemoglobin, basophil percentage, eosinophil percentage, total protein, albumin, direct bilirubin, indirect bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl aminotransferase (γ-GT), alkaline phosphatase (ALP), neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio. Data from patients with recompensated cirrhosis were recorded during the first contact visit. For patients with acute decompensated cirrhosis, data were obtained within 24 hours of the initial diagnosis.
Statistical analysis
All statistical analyses were conducted using R software (V.4.0.2). All data were presented as counts with percentages for categorical variables and medians (IQRs) for continuous variables. We followed the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) guideline for development and reporting of the new model.20 For variables with omission rates <20%, the mean imputation was used. χ2 and Kruskal-Wallis tests were used when appropriate to evaluate the significance of differences in distributions between patients with recompensation, patients with gastrointestinal bleeding, patients with bacterial infection, patients with hepatic encephalopathy and patients with ascites. Indicators with p<0.05 were subsequently included in the univariate logistic regression to identify the factors associated with recompensation, followed by multivariate analysis using those factors with p<0.05 in the univariate logistic regression analysis.
We combined the factors in each multivariate regression analysis and used decision trees to select recompensation indicators. The decision tree algorithm selected the most relevant of these clinical variables, their position within the decision tree and their optimal cut-off values. The model was fitted using the R software (V.4.0.2) rpart package with the settings minsplit=20 and maxdepth=6. A 10-fold cross-validation was used to reduce overfitting and to assess the discrimination ability of the model by estimating the corresponding sensitivity and specificity of the model and computing the overall accuracy rate along with a 95% CI for this rate (using binom.test) and a one-sided test to see if the accuracy is better than the ‘no information rate,’ which is taken to be the largest class percentage in the data.21 22 All tests were considered statistically significant when p<0.05.
Results
Baseline characteristic of patients
In the total sample of included patients, there were 553 patients with recompensation and 3400 patients with acute decompensation, including 1158 patients with gastrointestinal bleeding, 1715 patients with a bacterial infection, 104 patients with hepatic encephalopathy and 423 patients with ascites. The aetiology of liver cirrhosis in these patients was 1955 (49.5%) positive for HBV, 190 (4.8%) positive for HCV, 573 (14.5%) for alcohol abuse, 245 (6.2%) for autoimmunity and 990 (25%) for other causes. The median age was highest among the patients with ascites, while the proportion of male patients was highest among the patients with hepatic encephalopathy. The median red cell counts, platelet counts, haemoglobin, basophil percentage, eosinophil percentage, total protein, albumin, lymphocyte-to-monocyte ratio and proportion of patients with other aetiologies were highest among the patients with recompensation, while the median white cell counts, direct bilirubin, ALT, AST, γ-GT, proportion of patients with HBV infection and proportion of patients with autoimmunity were highest among the patients with bacterial infection. The proportion of patients with alcoholic cirrhosis, hypertension, diabetes, the median indirect bilirubin and ALP levels were highest among the patients with hepatic encephalopathy, while the median NLR was highest among the patients with gastrointestinal bleeding (table 1).
Baseline characteristics of patients
Factors associated with recompensation in patients with gastrointestinal bleeding
Of the 1158 patients with gastrointestinal bleeding, multivariate logistic regression showed that alcoholic cirrhosis (OR: 0.146, 95% CI, p=0.001), other aetiologies (OR: 2.986, 95% CI, p<0.001), hypertension (OR: 0.036, 95% CI, p<0.001), diabetes (OR: 0.216, 95% CI, p<0.001), haemoglobin (OR: 1.043, 95% CI, p<0.001), basophil percentage (OR: 3.447, 95% CI, p<0.001), total protein (OR: 1.151, 95% CI, p<0.001) and NLR (OR: 0.843, 95% CI, p<0.001) were factors related to recompensation (table 2).
Univariate and multivariate logistic regression analysis on factors associated with recompensation for patients with decompensated cirrhosis of gastrointestinal bleeding
Factors associated with recompensation in patients with bacterial infection
Of the 1715 patients with a bacterial infection, multivariate logistic regression showed that alcoholic cirrhosis (OR: 0.129, 95% CI, p<0.001), autoimmune-related cirrhosis (OR: 0.445, 95% CI, p=0.044), hypertension (OR: 0.016, 95% CI, p<0.001), diabetes (OR: 0.225, 95% CI, p<0.001), haemoglobin (OR: 1.021, 95% CI, p<0.001), basophil percentage (OR: 1.752, 95% CI, p=0.003), total protein (OR: 1.083, 95% CI, p<0.001), albumin (OR: 1.125, 95% CI, p<0.001), ALT (OR: 0.996, 95% CI, p=0.024) and NLR (OR: 0.841, 95% CI, p<0.001) were significantly correlated with recompensation (table 3).
Univariate and multivariate logistic regression analysis on factors associated with recompensation for patients with decompensated cirrhosis of bacterial infection
Factors associated with recompensation in patients with hepatic encephalopathy
Of the 104 patients with hepatic encephalopathy, multivariate logistic regression showed that alcoholic cirrhosis (OR: 0.041, 95% CI, p<0.001), other aetiologies (OR: 3.139, 95% CI, p=0.007), hypertension (OR: 0.004, 95% CI, p<0.001), diabetes (OR: 0.101, 95% CI, p<0.001), haemoglobin (OR: 1.027, 95% CI, p=0.016), total protein (OR: 1.163, 95% CI, p<0.001) and albumin (OR: 1.116, 95% CI, p=0.014) were associated with recompensation (table 4).
Univariate and multivariate logistic regression analysis on factors associated with recompensation for patients with decompensated cirrhosis of hepatic encephalopathy
Factors associated with recompensation in patients with ascites
Of the 423 patients with ascites, multivariate logistic regression showed that age (OR: 0.972, 95% CI, p<0.001), alcoholic cirrhosis (OR: 0.158, 95% CI, p<0.001), other aetiologies (OR: 2.167, 95% CI, p<0.001), hypertension (OR: 0.047, 95% CI, p<0.001), diabetes (OR: 0.255, 95% CI, p<0.001), total protein (OR: 1.101, 95% CI, p<0.001), albumin (OR: 1.131, 95% CI, p<0.001), ALT (OR: 0.992, 95% CI, p=0.014) and NLR (OR: 0.872, 95% CI, p=0.002) were associated with recompensation (table 5).
Univariate and multivariate logistic regression analysis on factors associated with recompensation for patients with decompensated cirrhosis of ascites
Tool to evaluate recompensation
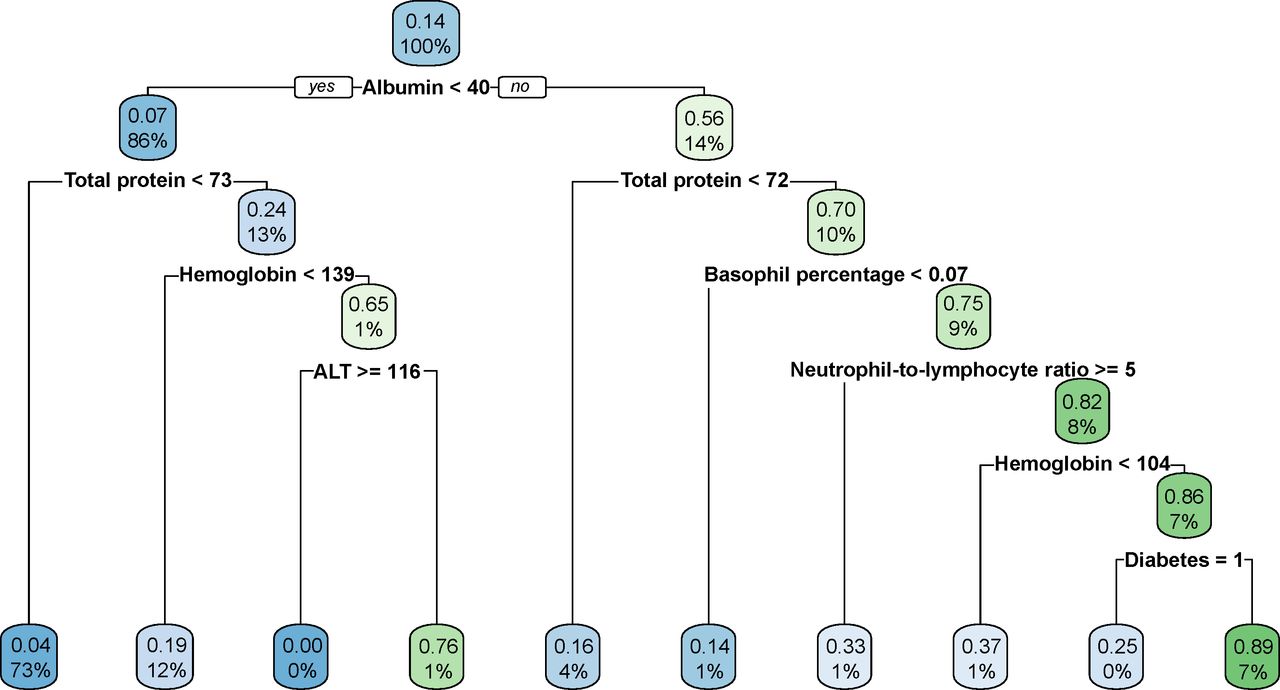
A decision tree was fitted to illustrate the observed associations and to detect other specific subgroups and relationships that may not be available through multivariate regression analysis. The variables which were statistically significant in the multivariate logistic regression from gastrointestinal bleeding group, bacterial infection group, hepatic encephalopathy group and ascites group were combined, and a decision tree was employed to determine the index correlations with recompensation in patients with decompensated cirrhosis. The most relevant indicator of recompensation selected by the decision tree model was albumin, with a threshold of 40 g/L (figure 1). Total protein, haemoglobin, basophil percentage, ALT, NLR and diabetes were also selected to subsequently distinguish patients. The overall accuracy rate of the model was 0.92 (0.91–0.93), with high specificity (86.9%) and sensitivity (92.6%).

{kind=link}
Decision tree plot for identifying recompensated cirrhosis. Each node shows the percentage of patients classified and their probability of recompensation (also represented by the colours and colour intensity). The blue colour represents acute decompensated cirrhosis. The green colour represents recompensated cirrhosis. The intensity of the colour indicates the accuracy of the classification of each category, the more intense the colour, the higher the accuracy.
If a patient with decompensated cirrhosis has serum albumin equal to or greater than 40 g/L, total protein equal to or greater than 72 g/L, basophil percentage equal to or greater than 0.07, NLR less than 5, haemoglobin equal to or greater than 104 g/L, and has no history of diabetes, then he/she has 89% probability to be discriminated as being recompensation. This is an example of an interpretation from figure 1.
Discussion
Recompensation is a special phase of decompensated liver cirrhosis. After a period of effective treatment, the liver function can meet the patients’ daily activities, and there will be no complications related to decompensated liver cirrhosis.4 Until now, there has been a lack of a comprehensive evaluation index to identify patients with a ‘recompensation advantage.’ In this study, we analysed the recompensation-related factors of different complications of decompensated liver cirrhosis and combined these factors to establish a decision tree based on the presence of several routine laboratory indicators and comorbidities. It has demonstrated that albumin, total protein, haemoglobin, basophil percentage, ALT, NLR and diabetes is associated with recompensation for patients with decompensated cirrhosis. The level of albumin was the most important indicator. The algorithm generally had good accuracy with high specificity and sensitivity.
The proposed decision tree included three liver function indexes (albumin, total protein and ALT). Many studies have suggested a correlation between albumin and the prognosis of cirrhosis, with low serum albumin concentration being an important factor in the poor prognosis of cirrhosis.23–25 For patients with alcohol-related liver disease on the liver transplantation waiting list, model for end-stage liver disease score <20 and albumin ≥32 g/L at entry were found to be the optimum cut-off points for predicting withdrawal from the transplantation list after recompensation.11 Long-term use of albumin has a low hospital admission rate and mortality due to tension ascites or complications, such as hepatic encephalopathy, spontaneous peritonitis, bacterial infections other than spontaneous peritonitis, renal insufficiency, type 1 hepatorenal syndrome and side effects caused by potential diuretics, such as hyponatraemia and hyperkalaemia.24 25 In our study, the cut-off value of albumin was 40 g/L, which was consistent with the results of the ANSWER study and indicated that only sufficient albumin concentrations can play a protective role.24 ALT is generally considered to be an indicator of liver damage due to steatosis and inflammatory responses.26 Severe impairment of liver function may lead to the risk of hepatic encephalopathy.27
Our study found that regardless of whether there was gastrointestinal bleeding, the level of haemoglobin in patients with decompensated liver cirrhosis was a relevant factor for recompensation. Anaemia is another factor that has been recently characterised as a predictor of poor outcomes in patients with cirrhosis, including ACLF occurrence in outpatients with liver cirrhosis, and hepatocellular carcinoma induced death.28–32 Bothou et al found that a low level of haemoglobin was a strongly and independent predictor of hospital admission in outpatients with decompensated liver cirrhosis.33 The mean value of haemoglobin reported by Bothou et al was 134 g/L. Anaemia can predict the development of ACLF in outpatients with cirrhosis, the median value was 108 g/L.29 Thus, improving anaemia is a therapeutic target for maintaining the stability of decompensated liver cirrhosis, and it is very probable that for patients with cirrhosis even mild anaemia should be treated. The pathophysiology of patients with liver cirrhosis may be related to anaemia, which leads to arterial hypotension and tachycardia, resulting in circulatory dysfunction. However, the specific mechanism needs to be investigated in future studies.
NLR is a novel indicator of systemic inflammation and has recently been reported to predict the outcome of patients with decompensated cirrhosis.34–36 The PREDICT study indicated that patients with stable decompensated cirrhosis had less systemic inflammation compared with pre-ACLF patients who exhibited systemic inflammation with rapid progression (leading to the development of ACLF and death within 90 days) and unstable decompensated cirrhosis patients who were readmitted at least once during 90 days but did not progress to ACLF.21 Our research indicated that the NLR was markedly higher in patients with acute decompensated cirrhosis with gastrointestinal bleeding, bacterial infection and ascites compared with that in patients with recompensation. An NLR equal to or greater than five is more likely to classified as acute decompensated liver cirrhosis. These findings clearly suggest that the systemic inflammatory response is predictive of a poor prognosis. Therefore, clinicians should pay significant attention to the prevention of infections, which could avoid secondary complications (further development of decompensation, recurrent infections, ACLF and death) of cirrhosis.37
Basophils may induce and expand inflammation by producing specific cytokines and proteases and are related to T helper 2 immune responses.38 39 However, their role in decompensated liver cirrhosis has rarely been reported. Our study found that the increase in the basophil percentage is an evaluation index of recompensation, especially for the occurrence of gastrointestinal bleeding or bacterial infection. We speculate that basophils may regulate local and systemic inflammatory responses and shape innate and adaptive immune responses to prevent acute decompensation, but the specific mechanism needs further study.
Diabetes is closely related to complications of liver cirrhosis. Diabetes may be related to an increased risk for the existence of covert hepatic encephalopathy and the development of overt hepatic encephalopathy in patients with liver cirrhosis.40 Uncontrolled diabetes is associated with an increased risk of infection, an enhanced propensity for renal insufficiency, and a variety of other related complications.41 Diabetes increases the risk of rehospitalisation within 30 or 90 days for patients with decompensated cirrhosis.42 43 These results are in line with our study that diabetes is a risk indicator for acute decompensation, and patients with decompensated cirrhosis without diabetes are more likely to have recompensation.
The strengths of our study
As far as we know, this was the first study for including patients who did not experience acute decompensation within 1 year as recompensation. Compared with the previous study, the patient’s condition was stable for a longer period of time. Furthermore, we combined logistic regression and decision tree to screen recompensation indexes, and proposed cut-off values of different indicators, which was more convenient for clinical application.
Limitations
Our study has several limitations. First, since our study of factors associated with recompensation in cirrhosis is unique, there were no other cohorts that could available for external validation. We will conduct a prospective study to further evaluate the effectiveness of this new model. Second, we did not compare known models, such as the Child-Turcotte-Pugh, model for end-stage liver disease, or chronic liver failure-consortium acute decompensation scores. Because our model neither includes subjective clinical symptoms, such as hepatic encephalopathy and the severity of ascites, nor indicators that cannot be detected in community hospitals, such as international normalised ratio. We only included the most widely used laboratory indicators and comorbidities. The study from the real world makes our indicators easier to apply in clinical and even community hospitals. Besides, we performed 10-fold cross-validation to reduce overfitting of the model. Third, these thresholds have not yet been validated in the external cohort. Therefore, the difference between these cut-off values may be related to the difference in the prevalence of cirrhosis among the studied populations.
Conclusions
This study showed the level of albumin, total protein, haemoglobin, basophil percentage, ALT, NLR and the history of diabetes is related to recompensation in patients with decompensated cirrhosis. The decision tree algorithm identified albumin with a threshold of 40 g/L as the indicator that most influenced the occurrence of recompensation. The knowledge of recompensated indicators may help support the development of different prevention strategies to reduce the incidence of acute decompensation.
Data availability statement
Data are available on reasonable request. The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Ethics approval
This study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University. Due to its retrospective nature, this study required no conformed consent. All methods were performed in accordance with ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Acknowledgments
We acknowledge Yidu Cloud Technology Company Ltd. for their contribution in the technology and data platform support and AJE (www.aje.com) for English language editing.
References
Footnotes
Contributors Study concept and design: XX, HW, WZ and BQ; acquisition of data: XX, HW, YW and JW; Analysis and interpretation of the data: XX, HW, WZ and BQ; drafting of manuscript: XX; critical revision of the manuscript for intellectual content: all authors; statistical analysis: XX, HW and WZ; study supervision: BQ.
Funding This work was supported by Chongqing Science and Health Joint Project (Grant no. 2020MSXM026). Intelligence Medicine Project of Chongqing Medical University (Grant no. YJSZHYX202001). The Natural Science Foundation of Chongqing (Grant cstc2019jcyj-bshX0010).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.