Article Text

Abstract
Introduction Neurodevelopmental delays and cognitive impairments are common in youth living with HIV. Unfortunately, in resource-limited settings, where HIV infection impacts millions of children, cognitive and neurodevelopmental disorders commonly go undetected because of a lack of appropriate assessment instruments and local expertise. Here, we present a protocol to culturally adapt and validate the Penn Computerized Neurocognitive Battery (PennCNB) and examine its validity for detecting both advanced and subtle neurodevelopmental problems among school-aged children affected by HIV in resource-limited settings.
Methods and analysis This is a prospective, observational cohort study. The venue for this study is Gaborone, Botswana, a resource-limited setting with high rates of perinatal exposure to HIV and limited neurocognitive assessment tools and expertise. We aim to validate the PennCNB in this setting by culturally adapting and then administering the adapted version of the battery to 200 HIV-infected, 200 HIV-exposed uninfected and 240 HIV-unexposed uninfected children. A series of analyses will be conducted to examine the reliability and construct validity of the PennCNB in these populations.
Ethics and dissemination This project received ethical approval from local and university Institutional Review Boards and involved extensive input from local stakeholders. If successful, the proposed tools will provide practical screening and streamlined, comprehensive assessments that could be implemented in resource-limited settings to identify children with cognitive deficits within programmes focused on the care and treatment of children affected by HIV. The utility of such assessments could also extend beyond children affected by HIV, increasing general access to paediatric cognitive assessments in resource-limited settings.
- HIV & AIDS
- infectious disease/HIV
- delirium & cognitive disorders
- paediatric neurology
- paediatric infectious disease & immunisation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- HIV & AIDS
- infectious disease/HIV
- delirium & cognitive disorders
- paediatric neurology
- paediatric infectious disease & immunisation
Strengths and limitations of this study
This protocol aims to culturally adapt and validate a computerised neurocognitive battery in 200 HIV-infected, 200 HIV-exposed uninfected and 240 HIV-unexposed uninfected children in Botswana.
This protocol involves the local expertise of patients and stakeholders to inform cultural adaptations and translations.
The study proposes to use a multimethod framework for validation of the neurocognitive battery, including reliability, structural validity, concurrent validity and criterion validity.
The study also aims to develop a brief screening measure to identify children in need of further neurocognitive evaluation.
The study is limited by the lack of a gold-standard cognitive assessment in Botswana to which we can compare.
Background
Approximately 1.8 million children worldwide are living with HIV.1 Although the incidence of HIV-related encephalopathy decreased with the introduction of combined antiretroviral therapies (cART),2 3 children and adolescents living with HIV still evidence neurodevelopmental delays and cognitive dysfunction. Cognitive deficits are primarily found in attention, information processing speed, episodic memory, executive functioning and psychomotor functioning.4–12 Deficits are greater in children with a history of higher disease severity, suggesting residual effects of HIV-associated cerebral injury.11 13 However, deficits are apparent even when the disease is well-managed4 10 11 14 and are associated with disease progression, functional limitations and future cognitive decline.11 15 Moreover, initiation of cART may halt the progression of neurocognitive dysfunction but does not reverse existing dysfunction.16–19 There is also evidence that HIV-exposed uninfected children (HEU) suffer from more neurodevelopmental delays than HIV-unexposed uninfected children (HUU).11 20–22
Taken together, it is clear that early, accurate detection of neurocognitive deficits is crucial for effective clinical, educational and rehabilitative care. Accurate assessments are particularly critical in areas with a high HIV prevalence, in resource-limited settings where exposures to HIV impact large numbers of children and in settings in which neurobehavioural disorders commonly go undetected.23 However, few locally validated cognitive assessments exist in resource-limited settings, which presents significant challenges for assessing cognition in adults and children with HIV.
Screening measures have been created to provide brief assessments for HIV-associated neurocognitive disorders, although most do not possess adequate diagnostic precision.24 Thus, it is recommended that a full neuropsychological battery assessing multiple domains of cognitive functioning be used to detect HIV-associated neurocognitive dysfunction.25 These batteries provide critical information about the pattern and severity of neurocognitive deficits and aid in disease management and understanding functional limitations. However, most neuropsychological batteries are proprietary, expensive and resource intensive. Most involve 3–5 hours of testing, with highly specialised training required in administration, interpretation and scoring. Furthermore, such batteries are predominantly administered by paper and pencil, raising the risk of errors in administration and scoring and creating challenges for data entry, management and rapid turnaround of results. Thus, these testing batteries are not feasible in many settings, including those with limited resources.
Modern computerised neurocognitive testing allows shorter testing times while offering sophisticated features unavailable to traditional neuropsychological tests, such as automatic, precise recording of response times and accuracy. The Brain Behavior Lab at the University of Pennsylvania has developed the Penn Computerized Neurocognitive Battery (PennCNB),26–28 a publicly available collection of ‘neurobehavioral probes’ designed to assess psychological constructs (eg, working memory) by way of their underlying brain networks. PennCNB tests have been subjected to an iterative validation process to evaluate their psychometric properties26 27 and normed in multiple populations.28–31 Importantly, PennCNB tests have been validated with functional neuroimaging as eliciting the recruitment of specific brain systems,32–35 making them useful as potential biomarkers of brain dysfunction.28 The cognitive domains assessed by conventional neuropsychological tests36 are readily replicated by the PennCNB, reinforcing its potential validity in individuals living with HIV. The PennCNB has been applied in several contexts, including large-scale genomic studies,28–30 longitudinal research,37 38 intervention studies39 and even in space flight.40 41 Importantly, the measures are well-tolerated by children and have been used for several specialised paediatric populations, including children with 22q11.2 deletion syndrome42–45 and chronic kidney disease,46 as well as the landmark Philadelphia Neurodevelopmental Cohort study, a sample of 9500 youth aged 8–21 years.47 Critically, the PennCNB has been culturally adapted in western and non-western cultures and translated into 12 languages, including a Nguni African language (isiXhosa).37 48–52
The current research protocol focuses on Botswana, a resource-limited setting with scarce neurocognitive or neurodevelopmental assessment tools and expertise. As the first country in Africa to provide free antiretroviral therapy in the public sector to all citizens living with HIV, Botswana has a large ageing population of children and adolescents with perinatally acquired HIV.53 In the proposed project, we aim to establish the validity, reliability and feasibility of administering the PennCNB in Botswana to assess neurocognitive functioning in children living with HIV.
In addition, we aim to develop a screening measure to identify which children would benefit from assessment with the PennCNB by adapting the Pediatric Symptom Checklist (PSC),54 a 3–5 min parent-report questionnaire validated for detection of psychosocial risk in children in several cultural contexts, including in Botswana by members of our team.55–57 We aim to enhance its sensitivity for identifying children with neurocognitive difficulties through adaptations, including adding questions about domains important for children with HIV-related cognitive dysfunction, such as academic functioning and self-direction.
Methods
Participants
Three groups of participants will be selected (figure 1). We will enrol 200 children with HIV (HIV+), 200 HEU and 240 HUU, all between 7 and <18 years old. We focus on school-aged children because some CNB subtests are less suitable for preschool-aged children, and most prior work has been conducted in school-aged children, enabling a more extensive knowledge base for comparison. HIV+ youth will be randomly selected from eligible youth in care at the Botswana-Baylor Children’s Clinical Centre of Excellence (COE) in Gaborone. Youth with HIV will be predominantly perinatally infected, and likely mode of infection for each participant will be recorded. We will enrol children randomly selected from local public schools in Gaborone, Botswana until 240 HUU children are enrolled. Randomisation will be stratified by age bands (ie, 7/8, 9/10, 11/12, 13/14, 15–17) for robust normative comparisons. Based on local seroprevalence data, it is estimated that ~5% of school-going youth will be HIV+ and ~20% will be HEU. HIV status and HIV exposure status will be unknown at the time that school-based participants are consented, though this information will be elicited. Students recruited from schools and HIV+ children enrolled in the clinic will be randomly selected from among all students/patients in an age stratum to achieve a minimum of 30 in each stratum. HEU children who are not part of the randomly selected school sample will be selected by recruiting family members of clinical patients to enrol 200 HEU children.

Study flowchart. Figure does not include the additional participants being enrolled as cases for the gold standard assessment. HEU, HIV exposed uninfected; HIV+, children with HIV; HUU, HIV unexposed uninfected.
Parents of enrolled children will privately complete surveys that will include HIV and HIV exposure status. Enrolment data will be uploaded daily to the data coordinating centre. A record will be kept (age, sex, reason for exclusion) of all individuals who were selected for enrolment but not enrolled.
Neurocognitive assessment
The core paediatric version of the PennCNB comprises 14 tests assessing five neurobehavioral domains.31 For the proposed study, we selected 13 tests from this battery and from our prior HIV work, as shown in figures 2 and 3 and described later. Tests were selected for inclusion based on the following criteria: (1) ability to assess the cognitive domains impacted in paediatric HIV and in utero HIV or antiretroviral therapy exposure4–10 58 59; (2) suitability for large-scale administration; (3) suitability for resource-limited settings; (4) suitability for translation and adaptation across cultures (eg, low language demands, limited unfamiliar stimuli); and (5) demonstrated sensitivity to individual differences and mild impairments. To enhance reliability and sensitivity, we use more than one test within each domain. All tests except the Penn Conditional Exclusion Test (PCET) include practice periods to ensure task engagement and comprehension.
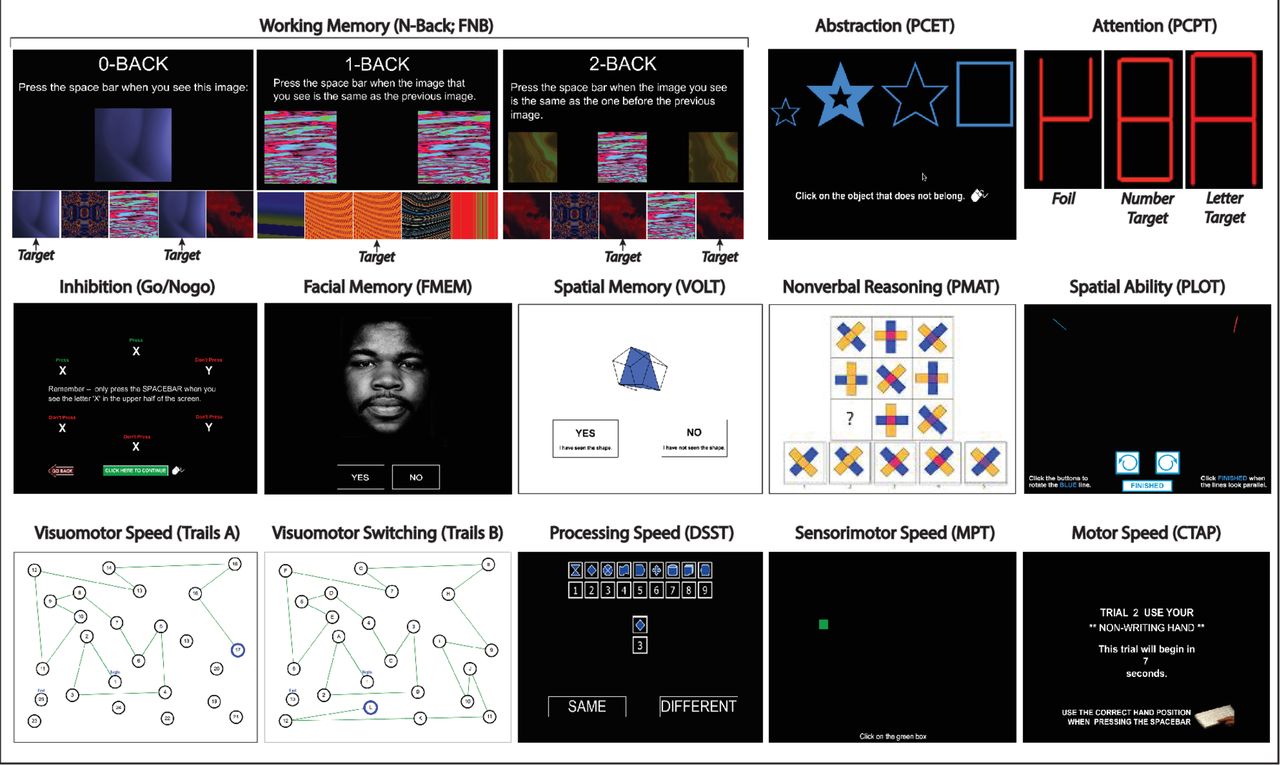
Tests selected from the Penn Computerized Neurocognitive Battery (PennCNB), English version. Stimuli used with permission from Dr Ruben Gur, lead author of the PennCNB. Image used for the FMEM is used as a stimulus and is not from a participant. Actors in these photos consented for their subsequent use without limitation. CTAP, Penn Finger Tapping Test; DSST, Penn Digit Symbol Substitution Test; FMEM, Penn Facial Memory Test; FNB, Fractal N-Back; MPT, Motor Praxis Test; PCET, Penn Conditional Exclusion Test; PCPT, Penn Continuous Performance Test; PLOT, Penn Line Orientation Test; PMAT, Penn Matrix Analysis Test; VOLT, Visual Object Learning Test.

{kind=link}
{kind=link}
{kind=link}
Tests selected from the Penn Computerized Neurocognitive Battery (PennCNB), Setswana Version. Stimuli used with permission from Dr Ruben Gur, lead author of the PennCNB. Image used for the FMEM is used as a stimulus and is not from a participant. Actors in these photos consented for their subsequent use without limitation. CTAP, Penn Finger Tapping Test; DSST, Penn Digit Symbol Substitution Test; FMEM, Penn Facial Memory Test; FNB, Fractal N-Back; MPT, Motor Praxis Test; PCET, Penn Conditional Exclusion Test; PCPT, Penn Continuous Performance Test; PLOT, Penn Line Orientation Test; PMAT, Penn Matrix Analysis Test; VOLT, Visual Object Learning Test.
Attention and processing speed
Penn Continuous Performance Test (PCPT)60; Digit Symbol Substitution Test (DSST)61; and Penn Trailmaking Test, Part A (TMTA). The PCPT presents 7-segment displays (1/s) and requires participants to respond when the segments form a number (first 1.5 min) or letter (next 1.5 min). The number of true positive responses reflects accuracy, and the median response time for true positives reflects attention speed. The DSST presents a reference set of digit-symbol pairs and a target digit-symbol pair. Participants are instructed to quickly indicate if the target pair matches one of the digit-symbol pairs in the reference set. The TMTA is a computerised analogue of the classic Trailmaking test that measures visual attention and processing speed, requiring participants to connect a sequence of numbers in sequential order.62
Episodic memory
Penn Face Memory Test (FMEM)63 and Visual Object Learning Test (VOLT).64 The FMEM presents 20 faces to remember, while the recall portion shows these target faces mixed with 20 distractors equated for age, gender and race. The version of the FMEM proposed in this study uses a multiracial assortment of faces. The VOLT shows participants a series of 10 three-dimensional Euclidean shapes. They are then shown a mixture of shapes they have seen and 10 novel shapes, and are asked to decide whether they have seen each shape before.
Executive functioning
PCET65 66; Fractal N-Back Test (FNB)67 68; Penn Trailmaking Test, Part B (TMTB); and Penn Go/Nogo (GNG).38 The PCET is a measure of abstraction and concept formation by hypothesis-testing, in which participants are presented with four objects and asked to select the one that does not belong, based on a sorting principle (eg, size). After a set number of successive correct responses, the sorting principle is changed (as in the Wisconsin Card Sorting Test). The FNB measures working memory by presenting a series of figures (fractals) and requiring the participant to identify visual repetitions occurring ‘n’ trials preceding the current stimulus. The TMTB is similar to the TMTA, but requires participants to alternate between letters and numbers (ie, 1→A→2→B), engaging set-switching abilities.9 69 The GNG is a measure of impulse control that requires participants to respond to a series of targets (an ‘X’ in the upper half of the screen) and inhibit responding to low-frequency non-targets (‘X’ in the lower half of the screen or a ‘Y’ anywhere). The test induces participants to develop a response tendency and then interrupts that tendency with intermittent non-targets to which participants have to inhibit responding.
Complex cognition
Penn Line Orientation Test (PLOT)70 and Penn Matrix Analysis Test (PMAT).71 The PLOT presents two angled lines. Participants click a button to rotate one line until they believe it has the same angle as the other. The PMAT is a measure of non-verbal reasoning that uses the same principles as Raven’s progressive matrices,72 consisting of matrices requiring reasoning by geometric analogy and contrast principles.
Sensorimotor speed
Finger Tapping Test (CTAP)73 and Motor Praxis Test (MPT). The CTAP measures how quickly the participant can press the spacebar using the index finger. The MPT requires moving the mouse and clicking on a green square that disappears after the click. The square gets increasingly small and appears in unpredictable locations.
Cultural adaptation and translation
For the Setswana version of the CNB and clinical interview materials, we followed WHO translation guidelines. The process of cultural and language adaptations involved a formal procedure that we have previously applied.74 75 This involved translation by a professional, followed by: (1) iterations of back-translating, resolving discrepancies and re-translating (when necessary); (2) piloting of tests and items; (3) discussions about challenging concepts; and (4) further modifications of the instruments to select the most linguistically and conceptually appropriate Setswana terminology. Concurrently, English terminology was adapted to be locally appropriate.
Patient and public involvement
At the initiation of the study, the principal investigators (EDL and JCS) met with clinicians and staff at the Baylor-Botswana COE in Gaborone and with other local stakeholders. This stakeholder group consisted of representatives from the Botswana Ministry of Basic Education and Ministry of Health and Wellness, physicians, teachers from area schools, school counsellors, social workers, nurses, psychologists, representatives from UNESCO, three young adults who were patients in the clinic cohort, and a parent of a clinic child with cognitive challenges. This multidisciplinary group of stakeholders was convened for 2 days to provide feedback on concepts and stimuli, offer thoughtful back-translation of the research instruments, assist with and discuss conceptual and linguistic discrepancies occurring during translation/back-translation, and promote the substantive involvement of the communities.
The stakeholder group offered important feedback to guide adaptations. First, they suggested that some older adolescent participants might prefer to receive the assessments in English, since English is used for higher level instruction in schools. Notably, this feedback was supported by our pilot testing (see later), in which two older participants asked to receive assessments in English. Thus, we created equivalent versions of assessments in English and Setswana. Second, they suggested a greater racial diversity of faces for the FMEM, which we adapted to address this feedback. Third, they suggested (and we developed) a formal practice period for gaining familiarity with the computers since many participants might not have used computers previously. Fourth, they suggested that certain words such as those for computer components (eg, screen, mouse) should be explained by study staff since there are limited appropriate Setswana words; standardised methods for these explanations were developed. Finally, the group suggested simpler ways of conveying several ideas that were initially translated into Setswana in a more formal or literal fashion.
The stakeholder group also chose the study name, ‘Ntemoga’. Ntemoga is a multifaceted Setswana word with meanings that are commonly translated as ‘cognition’, but also: ‘know me inside and out’, ‘acknowledge that I matter’, ‘notice me’, ‘take me seriously’ and ‘know my needs’.
Pilot sample
After completing adaptation and training, JCS and AMP supervised piloting of the tools to finalise procedures and get feedback from participants and assessors. Local assessors administered the battery to 10 children and adolescents with HIV from the clinic, including five boys and five girls distributed in ages between 7 and 17. This pilot sample assisted with additional minor modifications to instructions and study procedures.
Procedures for validation study
Parents of participants will provide demographic and health information and school reports. History of hospitalisations, nervous system disorders, surgeries requiring anaesthesia and current medication use will be collected. For HIV+ participants, we will record WHO clinical staging, WHO T-staging, nadir CD4+ T-lymphocyte count (CD4), and most recent CD4 and viral load. Participants will receive compensation for participating, with amounts determined by the national Health Research Development Council (equivalent to about US$4/participant per study visit).
Participants will be administered the PennCNB on laptops (MacBooks) by proctors with extensive remote and on-site training by PennCNB staff. Each facility provides a secluded and quiet room with adequate space. Facilities and procedures were verified during site visits by JCS, EDL, AMP, and monitored on an ongoing basis by local study staff. Proctors were trained to note protocol issues in designated fields and provide information necessary for determining the validity of results for each test separately and for the battery as a whole. All data from the validation sample will be used for validation procedures discussed later under the Analyses section.
‘Gold standard’ assessments
To assess the criterion validity of the PennCNB, in a subset of enrolled participants, we will evaluate its ability to identify children who are classified as cognitively impaired or unimpaired based on the best available local assessments. Participants for this subset will be drawn from two sources. HIV+ participants aged 10–17 years in the randomly selected clinic cohort will be evaluated by a clinical psychologist for possible inclusion. To supplement the randomly selected clinic patients, patients with HIV previously identified as having neurocognitive impairments will also be selected for re-evaluation to ensure adequate numbers of ‘impaired’ participants. We will select patients until 45 ‘cases’ and 23 ‘controls’ are identified.
Due to limited validated cognitive assessment tools in Botswana, ‘gold standard’ assessments use a team-based approach to comprehensively evaluate cognitive abilities and daily functioning of this subset. A local clinical psychologist will conduct an evaluation, consisting of: (1) an intake assessment, with in-depth qualitative interviews with the child and parent and review of school records; (2) Montreal cognitive assessment,76 a 30-question tool designed to assess cognitive ability in eight domains (orientation, short-term memory, executive function, language, abstraction, attention, animal naming and visuoconstructional); and (3) Draw-a-Person Test, measuring cognitive maturity and mental age. Through comprehensive review of the data, the clinical psychologist will preliminarily classify a participant as a case (ie, with clinically significant cognitive impairment) or a control (ie, without clinically significant cognitive impairment). The preliminary classifications will be discussed by a group of four clinicians with local and international expertise in paediatrics, neuropsychology and HIV, who will review data to determine whether each participant should be classified as a case, with cognitive impairments impacting daily functioning. If there is a lack of consensus, the participant will be deemed ‘unclassifiable’ and not included among cases and controls for analysis. To ensure that the randomly selected sample remains representative of the underlying clinical population, cases not drawn from the 200 randomly selected clinic patients will not be included in other analyses described later.
Screening assessment development—the ‘Ntemoga Screener’
Since the PennCNB takes over an hour to administer and requires trained proctors, we also aim to develop a simpler screening tool to prioritise children who are most likely to benefit from PennCNB screening. First, the PSC will be administered to each participant’s parent to assess participant psychosocial difficulties.54 Notably, the PSC displays high internal consistency, moderate to high test–retest reliability77 78 and moderate to strong correlations with ratings from psychiatric interviews.54 79 80 The PSC also shows promise for identifying children in need of further evaluation for neurocognitive dysfunction.81 Thus, we aim to enhance its sensitivity for that purpose through adaptations, including removal of items that are less discriminative for prediction of cognitive dysfunction and addition of questions querying relevant areas such as academic functioning and self-direction. This new ‘Ntemoga Screener’ will combine items from the PSC with additional items selected for their likely sensitivity to cognitive dysfunction and need for further evaluation. Use of this tool is similar to ‘pipeline optimisation’ in machine learning,82 in which, for example, a subsample of patients might be ‘ruled out’ from the very beginning as not having an illness. This is useful in statistical analysis but also has important practical implications, such as obviating the need for further medical assessment.
Analyses
Data cleaning
Response patterns for individual tests will be examined for subject-related problems (eg, extended periods of inattention, participant misunderstanding). Thresholds for whether to flag a test for validity problems vary by test. Flagged individual tests will be removed from analyses, so it is possible for some participants to only have data for some tests. Missing data will be handled using pairwise and (then) listwise deletion in all analyses so that effects of missing data handling can be compared.
Reliability
Reliability will be assessed with measures of internal consistency (Cronbach’s α and McDonald’s ωH 83) and test–retest reliability. To assess test–retest reliability, 50 participants will repeat testing in approximately 12 weeks. We will calculate intraclass correlation coefficients with one-way random-effects models.84 We have examined reliability in both USA and international cohorts26 37 and have found it acceptable to date. If reliability of any test is inferior to that seen in other cohorts, likely reasons for reduced reliability will be examined, and test–retest procedures will be repeated with the next 50 enrolled participants.
Validity
Because there is no ‘gold standard’ cognitive assessment in Botswana to which we can compare the PennCNB, we will use several procedures to provide evidence of validity in this setting. To examine concurrent validity, we will compare mean scores and effects of sex and age in Botswana HUU youth to US normative samples to determine whether expected effects are present. Although scores may be lower in youth from Botswana compared with US youth, especially on speeded measures,85 overall effects of age and sex should show similar patterns, which are well characterised in previous work.49 To examine predictive validity, we will compare CNB scores to the gold standard assessment classifications and evaluate its discriminability between children with and without clinically significant impairment. To assess the ability of the CNB to identify cases and controls, we will calculate classification accuracy statistics (eg, sensitivity, specificity, positive predictive value) and area under the receiver operating characteristic curves. To maximise generalisability of findings, all prediction results will be cross-validated by leave-one-out and bootstrapped split-half approaches.
We will conduct factor analyses to determine whether the structural validity of the battery is consistent with theory and past work. We will compare the PennCNB factor structure across groups to test for measurement invariance, as we have done previously.31 38 We will examine group differences in cognitive performance on the PennCNB, comparing overall and individual test performance using both age-corrected scores and rates of impairment within each domain, using a well-validated deficit score approach.86 Neuropsychological norms will be generated for each 2-year age bin. Comparisons among HIV+, HEU and HUU groups will be conducted using both multiple regression (for continuous scores) and logistic regression (for impairment outcomes), with comparison of adjusted and unadjusted models to assess the influence of covariates (eg, sociodemographic factors). We will also use multivariate normative comparisons87–89 to account for the covariances among tests when assessing deviation of scores on any given test, avoiding a multiple-testing problem. It is expected that, compared with HUU, children with HIV will demonstrate significantly worse overall CNB performance, with the greatest impairment in domains most consistently shown to be impaired in paediatric HIV, including executive functioning (eg, working memory) and attention and processing speed, indicating convergent validity. We also expect that children with HIV will demonstrate smaller deficits on subtests measuring domains with less consistent evidence for deficits (eg, spatial processing).
After the parents of 300 study participants have completed the PSC, classification accuracy statistics will assess the ability of the PSC as a whole and individual PSC questions to identify children with cognitive impairment on the PennCNB. Questions that lack association with PennCNB classifications will be considered for removal. In-depth semistructured interviews of parents of children who had abnormal CNB testing will help to identify new candidate questions for the ‘Ntemoga Screener’ tool. In addition, an outcome-neutral method of scale construction—that is, use of computerised adaptive test simulation70—will be used to compare items selected using the two methods.
Parents of the final ~200 participants to enrol will complete the Ntemoga Screener, and associations between scores on the Ntemoga Screener and the PennCNB will be calculated. We hypothesise that the Ntemoga Screener will more readily identify children at risk for neurocognitive difficulties.
Ethics and dissemination
Ethical approval was granted by the Health Research and Development Division of the Botswana Ministry of Health and Wellness, Botswana-Baylor Children’s Clinical COE, and University of Pennsylvania Institutional Review Board. Children will provide assent, and parents/guardians will provide informed consent prior to participation. Informed consent/assent materials will be presented in Setswana or English, according to participant/parental preference. Potential participants will be excluded if they have severe developmental delays that prevent them from following simple instructions or are unable to assent, or if consent cannot be obtained from an authorised parent/guardian.
This project seeks to address the lack of validated tools to measure neurocognitive deficits among children affected by HIV in resource-limited settings, a significant public health issue. Findings from this research will be disseminated in peer-reviewed journals and scientific meetings, and we will communicate results and implications to critical stakeholders in Botswana, including regular updates to our stakeholder group.
In the future, tools developed from this study could provide practical screening and streamlined, comprehensive assessments that could be widely implemented in resource-limited settings to identify children with neurocognitive deficits, who could then be targeted for specific rehabilitation programmes. Thus, the proposed study could lay the groundwork for increased access to paediatric cognitive assessments in resource-limited settings. On-going mixed-methods research led by AEVP is obtaining implementation guidance by eliciting stakeholder perspectives in the medical and educational sectors in Botswana to identify factors likely to influence the success of implementing the PennCNB. These data will inform implementation strategies for the effective use of the PennCNB to support child health and wellness in Botswana.
Acknowledgments
The authors wish to thank our Stakeholder Group in Botswana who provided invaluable guidance and support for this project.
References
Footnotes
Contributors Study concept and design: JCS, EDL, AEVP, TMM, RCG, MM. Drafting of the manuscript: JCS, EDL, AEVP, TMM. Critical revision of the manuscript for important intellectual content: JCS, EDL, AEVP, AMP, LN, TMM, RCG, OP, OT, MM, KR, JC. Obtained funding: JCS, EDL. Technical, software and material support: AMP, LN, OP, OT, MM, KR, JCS. Study supervision: JCS, EDL.
Funding This work was supported by the NIH (R01 HD095278). TMM is supported by the Lifespan Brain Institute (LiBI) of the University of Pennsylvania and the Children’s Hospital of Philadelphia. Indirect support was received from two NIH-funded centers at Penn, the Penn Center for AIDS Research (CFAR; P30 AI045008) and the Penn Mental Health AIDS Research Center (PMHARC; P30 MH097488). The funding sources had no role in the design of the study; collection, analysis and interpretation of data; or in writing the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.