Article Text

Abstract
Objectives We aimed to systematically review the published literature regarding adults with clinical suspicion of pneumonia that compares the accuracy of lung ultrasonography (LUS) performed by non-imaging specialists to other reference standards in diagnosing and evaluating the severity of community-acquired pneumonia. Moreover, we aimed to describe LUS training and the speciality of the physician performing LUS, time spent on the LUS procedure and potential harms to patients.
Materials and methods We searched MEDLINE, Embase, CINAHL, Web of Science and Cochrane Central Register of Controlled Trials up until May 2019. We included studies that used LUS to diagnose pneumonia, but also confirmed pneumonia by other means. Publications were excluded if LUS was performed by a sonographer or radiologist (imaging specialists) or performed on other indications than suspicion of pneumonia. Two review authors screened and selected articles, extracted data and assessed quality using Quality Assessment of Diagnostic Accuracy Studies 2.
Results We included 17 studies. The sensitivity of LUS to diagnose pneumonia ranged from 0.68 to 1.00; however, in 14 studies, sensitivity was ≥0.91. Specificities varied from 0.57 to 1.00. We found no obvious differences between studies with low and high diagnostic accuracy. The non-imaging specialists were emergency physicians, internal medicine physicians, intensivists or ‘speciality not described’. Five studies described LUS training, which varied from a 1-hour course to fully credentialed ultrasound education. In general, the methodological quality of studies was good, though, some studies had a high risk of bias.
Conclusion We found significant heterogeneity across studies. In the majority of studies, LUS in the hands of the non-imaging specialists demonstrated high sensitivities and specificities in diagnosing pneumonia. However, due to problems with methodology and heterogeneity there is a need for larger studies with uniform and clearly established criteria for diagnosis and blinding.
PROSPERO registration number Prospectively registered in PROSPERO (CRD42017057804).
- ultrasonography
- respiratory infections
- general medicine (see internal medicine)
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review to focus specifically on lung ultrasonography to diagnose community-acquired pneumonia in adults in the hands of non-imaging specialists physicians working clinically.
We rigorously followed the Cochrane recommendations for conducting systematic literature reviews and searched five major databases using a broadly defined search string.
We distinguished between imaging specialists defined as sonographers or radiologists and non-imaging specialist defined as physician working clinically, even though some physicians working clinically may have an experience with ultrasonography similar to that of an imaging specialist.
Introduction
Community-acquired pneumonia (CAP) is a frequent and serious health concern, leading to increased morbidity and mortality if not detected and treated properly.1 2 CAP accounts for 2.5% of all patient contacts in Danish general practice3 and globally causes countless hospital admissions, laboratory tests and imaging procedures.4
Today, the typical imaging procedures for diagnosing pneumonia are CT scan of the chest and chest X-ray (CXR), with CT considered the gold standard.5 However, far from all patients have these imaging procedures performed due to high radiation dose, high costs and low availability.6
An alternative mode of imaging is lung ultrasonography (LUS). The advantages of LUS are absence of radiation, high availability and low cost.7 Moreover, LUS can be performed as a bedside point-of-care test to supplement the physician’s clinical examination. Numerous reviews and meta-analyses indicate that LUS has excellent accuracy for the diagnosis of pneumonia in adults.8–13 None of the existing literature, however, differentiates between LUS operators despite the fact that ultrasound generally is considered a highly user-dependent imaging modality.14 To our knowledge, no previous review has focussed solely on the accuracy of LUS in the hands of physicians working clinically.
The aim of this study was to systematically review the published literature regarding adults with clinical suspicion of pneumonia that compares the accuracy of LUS performed by physicians working clinically (non-imaging specialists) to other reference standards in diagnosing and evaluating the severity of CAP. Moreover, to describe LUS training and the speciality of the physician performing LUS, time spent on the LUS procedure and potential harms to patients.
Methods
Data sources and search strategy
This review was prospectively registered in PROSPERO. We followed the Cochrane guideline15 for conducting a systematic literature review, and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline for reporting the results. The literature search was conducted by a medical librarian and JJS in February 2017 and updated in May 2019. We searched the following databases: MEDLINE and Embase via Ovid, CINAHL via Ebsco, Web of Science and Cochrane Central Register of Controlled Trials.
The search terms ‘ultrasonography’ and ‘pneumonia’ were used in combination and with thesaurus terms (online supplementary e-appendix 1). Reference lists of included articles and identified reviews were evaluated manually for further eligible studies. Patients or the public were not involved in our research. All data relevant to the study are included in the article or uploaded as online supplementary information.
Supplemental material
Eligibility and selection of studies
Studies were eligible if a full-text paper with original data was available, the paper described the use of LUS for diagnosing CAP in adults (≥18 years) and the diagnosis of CAP was confirmed by other means, for example, other imaging. Hence, we included all diagnostic accuracy studies that used any reference standard other than LUS. Studies were excluded if not published in English, Danish, Norwegian, or Swedish, if LUS was performed on other indications than suspicion of pneumonia, if LUS was performed by an imaging specialist or if the pneumonia was considered to be ventilator-associated or nosocomial. We defined an imaging specialist as a sonographer or radiologist, and a non-imaging specialist as a physician working clinically.
Two review authors (JJS and PSH or MPH) independently screened the titles and abstracts of all studies identified. Any disagreements were resolved by consensus or by consulting other review authors (CAA and MBJ).
Two review authors (JJS and PSH or MPH) independently extracted data using an adapted version of the Cochrane data exaction template (online supplementary e-appendix 2). We contacted study authors when information about the physician performing the LUS was incomplete or missing, or if important data could not be derived directly from the published study.
Methodological assessment
Methodological quality of the selected studies was evaluated according to the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2).16 Two reviewers (JJS and PSH or MPH) independently performed the assessment of methodological quality. Any disagreements were resolved by consensus or by consulting a third review author (CAA).
Patient and public involvement
No patient involved.
Results
The database search identified 7285 individual, non-duplicate articles, and one potential article was identified through the reference lists (figure 1). Twelve studies had little or no information about the physician performing LUS17–28 and we contacted the corresponding authors of these studies. Based on additional information provided by the study authors, two studies were included18 27 and two studies were excluded.21 25 No elaboration was available for the remaining eight studies. They were thoroughly assessed and four were included, as they clearly described the scanning physicians as a non-imaging specialist physician working clinically.17 19 20 22 The remaining four studies were excluded.23 24 26 28

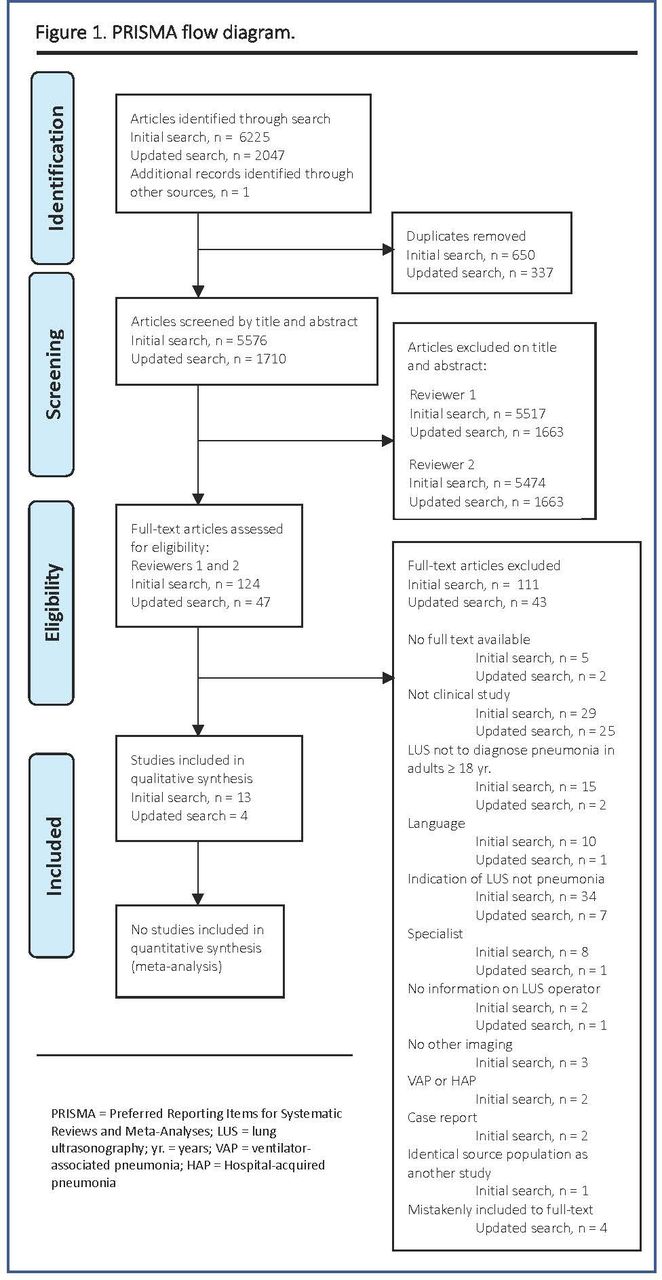{kind=link}
PRISMA flow diagram. HAP, hospital-acquired pneumonia; LUS, lung ultrasonography; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; VAP, ventilator-associated pneumonia; yr, years.
One study included both patients with CAP and nosocomial pneumonia.29 However, data on the CAP subgroup was obtained by correspondence with the study authors.
In total, 17 studies describing LUS in the hands of the non-imaging specialist to diagnose CAP in adults were included17–20 22 27 29–39 (figure 1).
Study characteristics
The studies were published between 1996 and 2019; 16 were prospective diagnostic accuracy cohort studies, and one was a retrospective study27 (online supplementary e-table 1).
The majority of studies included patients admitted to hospital, although one multi-centre study enrolled both hospitalised patients and outpatients20 (table 1). The studies included between 11 and 356 adult patients with a mean age from 34.0 to 84.8 years, of whom between 47% and 93% were men. Two studies included only patients aged ≥65 years.27 36
Diagnostic accuracy of LUS
The signs and symptoms of pneumonia described in the American Thoracic Society guidelines (cough, pleuritic pain, sputum production, fever and dyspnoea) were used as inclusion criteria in nine studies19 20 22 29 31 33–36 and six studies based inclusion on comparable, but not identical, criteria.17 27 30 37–39 The remaining two studies only included patients with respiratory complaints like cough, dyspnoea, chest pain or haemoptysis leading to a chest CT being ordered.18 32
Definition of pneumonia based on LUS varied across studies. Still, presence of subpleural or alveolar consolidation or a tissue-like lesion was part of the definition in all studies except one, in which no definition was described.35 The physicians performing and interpreting LUS were generally blinded to the reference standard; however, in four studies, this matter was unclear.17 22 27 35 The definitions of pneumonia, blinding, scanning procedure and characteristics of LUS are listed in online supplementary e-table 2. The reference standard varied from CT, qualitative assessment of the final diagnosis based on clinical, laboratory and microbiological data, including CXR or chest CT results, and CXR combined with CT when LUS and CXR were discordant (table 1).
Overall, the methodological quality of the included studies, according to QUADAS-2, was good (online supplementary e-table 3). Some studies, however, had a high risk of bias regarding flow and timing due to heterogeneity in the reference standard between patients, and high risk of bias in patient selection due to the exclusion of patients with pulmonal or cardiac comorbidities. The study populations, severity of condition (intensive care unit vs non-intensive care unit), and the reference standard were heterogeneous across studies. As a result, the specific requirements for including results in a meta-analysis (eg, comparable populations, LUS performer and reference standard), were neither met by the included studies nor by a subgroup of included studies.
Diagnostic accuracy of LUS
Diagnostic accuracy is presented in table 1. The sensitivity of LUS to diagnose CAP ranged from 0.68 (95% CI, 0.52 to 0.81) to 1.00 (95% CI, 0.95 to 1.00); in 14 of the 17 studies, it was ≥0.91. The specificity could be calculated in 13 of the studies. It varied from 0.57 (95% CI, 0.34 to 0.78) to 1.00 (95% CI, 0.92 to 1.00), but in seven studies, it was ≥0.94. We found no systematic differences between studies with low and high diagnostic accuracy in terms of study setting, participant training or experience, or choice of reference standard. Inter-observer agreement was reported in two studies with κ-values of 0.83 and 0.90.32 36
The studies by Liu et al and Amatya et al were the two studies of highest methodological quality (online supplementary e-Table 3). Both studies compared LUS to CT (table 1) and LUS was performed by emergency physicians whose prior experience and training was described (table 2). However, they differed with regards to procedure and characteristics of LUS in terms of areas examined and definition of pneumonia on LUS (online supplementary e-Table 2). They found sensitivities of, respectively, 0.95 (95% CI, 0.89 to 0.98) and 0.91 (95% CI, 0.78 to 0.98) and specificities of 0.99 (95% CI, 0.92 to 1.00) and 0.61 (95% CI, 0.36 to 0.83).
Speciality of non-specialists, experience and training in LUS
None of the studies compared sonographic findings to clinical outcomes. Three studies assessed the severity of pneumonia in patients with either CURB-6518 22 or Pneumonia Outcome Research Team score,34 but these were not compared with LUS findings.
Bourcier et al30 stratified their results according to onset of symptoms of pneumonia (<24 hours versus >24 hours). They found that LUS (sensitivity of 0.97) was significantly more effective than CXR (sensitivity of 0.30) in diagnosing pneumonia when time from clinical onset was <24 hours.
Speciality and training of non-imaging specialists
Information about speciality, experience and training of physicians performing LUS is presented in table 2. LUS was performed by emergency physicians, internal medicine physicians and by intensivists, while four studies did not declare the specific speciality of the non-imaging specialists.17 19 20 22 Nine studies reported that physicians had previous experience with LUS or ultrasonography in general.17 18 20 27 31–34 38 Prior experience of performing LUS varied from 1 week in the emergency department to more than 10 years of clinical experience.
Five studies described a LUS training programme for the participating physicians.30 31 36–38 Two studies provided a reference for an established educational programme,31 36 whereas the remaining studies described training specifically designed for their study.30 37 38 All training programmes included both theoretical and practical sessions. A large variation in the extent of the training programmes was noted, ranging from a few hours at a course facility37 to completion of a European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB)14 level one qualification.36 Four studies reported the time spent performing LUS, which was overall <10 min.
Potential harms to patients
Twelve studies reported false positive results from LUS, and 14 studies described false negative results (table 3). Corradi et al reported a high number of false negative results as they found 14 (22%) false negative hemithorax LUS examinations.18 However, five of these were reported in patients with bilateral pneumonia, in whom LUS examination only detected pneumonia in one hemithorax. Moreover, Corradi et al described that LUS-positive pneumonia were larger in diameter (81±55 mm) and close to the pleural line (1±3 mm).18 Likewise, more studies described false negative results that were mainly seen in patients with small consolidations where pneumonia did not reach the pleura.20 22 30 32
Potential harms to patients
Parlamento et al reported two incidental findings of subpleural consolidations in patients without pneumonia.34 In both cases, LUS findings were verified by chest CT scan and confirmed to be, respectively, an atelectasis caused by a large pleural effusion and a case of pulmonary embolism.
Discussion
To our knowledge, this is the first systematic review to focus specifically on LUS to diagnose CAP in adults in the hands of non-imaging specialists physicians working clinically. These non-imaging specialists were emergency physicians, internal medicine physicians, intensivists or unclassified physicians and obtained LUS sensitivities and specificities that were typically above 0.90. We found no overall difference in diagnostic accuracy when compared with study setting or the physicians’ speciality, experience or training. Importantly, the variation in sensivitity and specificity was found across reference standards. No study compared sonographic findings to the severity of pneumonia. Only a few studies described LUS training of the non-imaging specialists, and these training programmes varied from short lectures to fully accredited ultrasound education.
We highlighted the results of Liu et al and Amatya et al due to the quality of the studies, but the studies were not completely comparable in other parameters. Both studies found high and comparable sensitivities of 0.95 (95% CI, 0.89 to 0.98) and 0.91 (95% CI, 0.78 to 0.98), respectively. However, in Amatya et al, LUS specificity was 0.61 (95% CI, 0.36 to 0.83) and significantly lower than the specificity in Liu et al of 0.99 (95% CI, 0.92 to 1.00). According to Amatya et al, this was due to a higher prevalence of pulmonal co-morbidities which resulted in false positive LUS results. Low specificity may lead to over-diagnosis of pneumonia and inappropriate use of antibiotics.
The diagnostic accuracy of LUS for diagnosing pneumonia described in this review is consistent with results from previous reviews that made no distinction between imaging specialists and physicians working clinically.8–13 Recently, Orso et al obtained a pooled sensitivity of 0.92 and a specificity of 0.93 in a review based on studies performed in emergency departments.40 Of course, the majority of LUS operators were emergency physicians, corresponding to the non-specialists in the present review. Consequently, Orso et al and this study have included many of the same studies. However, Orso et al also included studies with imaging specialists and patients with ‘acute respiratory failure’. Our review included LUS performed by non-imaging specialists from different specialties and in different settings. One study was even partly conducted in outpatient settings with non-hospitalised patients.20 Importantly, the results of this particular study did not differ from the remaining studies. Hence, LUS might also be applied on non-hospitalised patients with suspected CAP, which supports the vision that LUS could be a useful tool for any clinician in the future.41
Non-imaging specialists working in primary care are first in line to see patients with CAP and general practitioners have already begun using point-of-care ultrasound.42 43 The results by Bourcier et al suggest that LUS is a better diagnostic tool for achieving an early diagnosis (≤24 hours from clinical onset) compared with CXR. The ability of LUS to accurately diagnose pneumonia early in the course of the disease may improve outcomes for patients attending primary care.43 Furthermore, improved diagnostic performance in patients with suspected CAP may reduce the need for antibiotics. On the other hand, the size of pulmonary lesions might be smaller in the early stages of disease and the results indicate that the usability of LUS to diagnose CAP is compromised by its inability to visualise pulmonary lesions that are not in contact with the pleura. However, according to Lichtenstein et al who looked for lung consolidation in intensive care patients, this occurred in only 1.5% cases of lung consolidation44 . Due to a lower prevalence and less severe disease in a general practice population, further evaluation of LUS for the diagnosis of CAP in general practice is required.
LUS is a user-dependent examination and several guidelines14 45 46 stress that diagnostic performance requires sufficient training to gain the necessary competencies. A meta-analysis by Tsou et al found a significant difference in diagnostic accuracy between LUS performed by ‘advanced’ versus ‘novice’ sonographers in the diagnosis of pneumonia in children.47 However, they defined ‘novice sonographers’ as physicians with little or no prior LUS experience or training (≤7 days); most of the non-imaging specialists in the present review would be classified as ‘advanced sonographers’ according to this definition. Though, the learning curve appears steep from paediatric data and in a randomised controlled trial by Jones et al,48 they found that substitution of CXR with LUS when evaluating children suspected of having pneumonia was feasible and safe, also in the hands of novice sonographers (≤25 examinations). Today, there are no guidelines or recommendations specifying the amount of training or level of competence needed to perform LUS.49 50 As this review has shown, however, these competencies can be reached by the non-imaging specialist physician even after a short, tailored training programme. To ensure that physicians maintain and develop skills over time and learn to incorporate LUS findings into clinical decision-making, longitudinal training elements must be incorporated into the training programmes.50
This study describes the different specialties of the non-imaging specialists and demonstrates great heterogeneity in their prior experience and training in LUS. However, sensitivities and specificities are comparable, thereby implying that LUS can be performed by physicians in various specialties, and by less experienced physicians, with comparable results to those of physicians with considerable experience in LUS.
Limitations
The aim of this study was to describe the diagnostic accuracy of LUS for diagnosing CAP when performed by physicians with considerably less ultrasound experience than imaging specialists. In four of the included studies, the speciality of the physician was not reported.17 19 20 22 These studies were included as we assessed from the clinical setting that the physicians were not radiologists or sonographers. The results from these four studies did not differ from the remaining studies. Furthermore, while some of the physicians had extensive experience with LUS,17 18 34 and their ultrasonography competencies may be compared with those of an imaging specialist, we did not find, in general, that sensitivity and specificity increased with experience. Comparison of studies was difficult due to sparse information on the non-imaging specialists’ training, their experience with LUS and the heterogeneity in the reference standards used. Due to the significant heterogeneity across studies, it was not appropriate to pool data and perform a meta-analyses.
Conclusion
We found significant heterogeneity across studies. In the majority of studies, LUS in the hands of the non-imaging specialists demonstrated high sensitivities and specificities in diagnosing pneumonia. However, due to problems with methodology and heterogeneity, there is a need for larger studies with uniform and clearly established criteria for diagnosis and blinding.
References
Footnotes
Contributors JJS is the guarantor of the study. JJS, PSH, MPH, MBBJ, OG and CAA contributed to the concept, design and drafting of the study. JJS, PSH and MPH conducted the systematic search strategy and the review. All authors revised critically and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.