Article Text

Abstract
Objective To determine the effect of occupational therapy provided at home on activities of daily living, behavioural and psychological symptoms of dementia (BPSD) and quality of life (QOL) for people with dementia, and the effect on family carer burden, depression and QOL.
Design Systematic review and meta-analysis.
Methods Eight databases were searched to February 2018. Randomised controlled trials of occupational therapy delivered at home for people with dementia and their family carers that measured ADL, and/or BPSD were included. Two independent reviewers determined eligibility, risk of bias and extracted data.
Results Fifteen trials were included (n=2063). Occupational therapy comprised multiple components (median=8 sessions). Compared with usual care or attention control occupational therapy resulted in improvements in the following outcomes for people with dementia: overall ADL after intervention (standardised means difference (SMD) 0.61, 95% CI 0.16 to 1.05); instrumental ADL alone (SMD 0.22, 95% CI 0.07 to 0.37; moderate quality); number of behavioural and psychological symptoms (SMD −0.32, 95% CI −0.57 to −0.08; moderate quality); and QOL (SMD 0.76, 95% CI 0.28 to 1.24) after the intervention and at follow-up (SMD 1.07, 95% CI 0.58 to 1.55). Carers reported less hours assisting the person with dementia (SMD −0.33, 95% CI −0.58 to −0.07); had less distress with behaviours (SMD −0.23, 95% CI −0.42 to −0.05; moderate quality) and improved QOL (SMD 0.99, 95% CI 0.66 to 1.33; moderate quality). Two studies compared occupational therapy with a comparison intervention and found no statistically significant results. GRADE ratings indicated evidence was very low to moderate quality.
Conclusions Findings suggest that occupational therapy provided at home may improve a range of important outcomes for people with dementia and their family carers. Health professionals could consider referring them for occupational therapy.
PROSPERO registration number CRD42011001166.
- dementia
- geriatric medicine
- occupational therapy
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Comprehensive searches were used that were not restricted to English language or by publication date.
All studies had a high risk of bias with respect to lack of blinding of participants and therapists, and most had no assessor blinding, but this is known to be difficult to achieve in rehabilitation research.
The overall quality of the evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) criteria: study design, risk of bias, inconsistency, indirectness and imprecision, with the overall quality of evidence in this review ranging from very low to moderate.
Introduction
Providing support for people with dementia who live at home is an important, yet challenging issue of concern to people with dementia and their families, healthcare providers and policymakers.1 It is estimated that in 2015, 46.8 million people were living with dementia worldwide with an international cost of ~US$818 billion for that year.2 People with dementia have significant difficulties with cognitive function, language and activities of daily living (ADL), and may have behavioural and psychological symptoms of dementia (BPSD) such as apathy, depression, agitation and anxiety.3–5 These changes in communication, function and in behaviours (which are often a response to, or communication of unmet needs) can be stressful and difficult for family carers to cope with.6
The majority of people with dementia live at home and are dependent on receiving care from family carers.7–9 Family members who take on the role of primary carer subsequently have reported increased rates of carer strain, physical and mental health problems, and experience difficulties in maintaining employment, leisure activities and family interactions which impacts their quality of life (QOL).8 With increasing numbers of people being diagnosed with dementia, the demand for research into approaches to enable people to stay at home as long as possible and avoid institutionalisation with ensuing increases in healthcare costs is strong.1 2 However, for people with dementia to stay at home, family carers need support to optimise the person’s independence in ADLs and to be able to understand and respond to changes in the person’s behaviours and psychosocial needs, among the myriad of other day to day issues they need to attend to.
Research testing the effects of non-pharmacological interventions for people with dementia is expanding.1 Non-pharmacological interventions may play a role in delaying functional decline, reducing the severity of BPSD and in supporting family carers.5 10 Systematic reviews of non-pharmacological interventions11 12 and the Clinical Practice Guidelines for Dementia in Australia13 have noted the potential of occupational therapy for people with dementia living in the community.14 15 Occupational therapists aim to improve the fit between occupation (eg, activities and roles), the person’s capabilities, and the physical and social environment in which they live in order to optimise participation in valued activities, roles and relationships.16 For people with dementia, this process may involve helping them to identify activities they find meaningful, simplifying and implementing these activities in such a way that optimises their engagement in them, and removing stressors and distractions from the environment.14 15 17 It also involves collaborating with family carers to help them more readily recognise and adjust aspects of the activity and environment that enables this engagement and participation.15 17 Previous systematic reviews have considered the effect of any interventions delivered by a range of health professionals for maintaining occupations broadly to improve or maintain the person’s health and QOL18 19; the effect of occupational therapy interventions specifically on BPSD in a range of different environments20; and the effect of any non-pharmacological intervention (including occupational therapy) on functional decline in people with dementia.21 These reviews either did not use meta-analysis,18 21 included studies with participants from both the community or hospital/aged care settings,18–20 or did not consider outcomes for family carers.20 21
A systematic review is needed that focuses specifically on the effects of occupational therapy provided at home for people with dementia and their family carers, to inform health professionals who provide support and referral for people with dementia in the community. This is important because identifying approaches to support people with dementia who live at home is a high priority of both consumers and the healthcare system.1 The aim of this systematic review were to evaluate the effect of occupational therapy provided at home on the performance of ADL, BPSD and global QOL for people with dementia. It also aimed to determine the effect of this therapy on carer burden, depression and QOL.
Methods
Details of the protocol for this systematic review were registered on PROSPERO and can be accessed at www.crd.york.ac.uk/prospero 22 (online supplementary File 1). It describes prespecified review questions, search strategies, eligibility criteria, data extraction, data analysis and strategies for assessing risk of bias. We used the Preferred Reporting of Items for Systematic Reviews and Meta-Analyses (PRISMA)23 as a guideline for reporting this review.
Supplemental material
Patient and public involvement
There was no patient or public involvement in this review, although some authors have been family carers of people with dementia.
Eligibility criteria
We included only randomised controlled trials assessing the effect of occupational therapy for people with dementia and their family carers if therapy was delivered at the participant’s home and aimed to optimise ADL of the person with dementia, and/or to manage BPSD. Interventions delivered in community facilities were excluded. We defined occupational therapy services as being predominantly (over 75%), delivered by a qualified occupational therapist, or under the supervision of a qualified occupational therapist. Occupational therapy could be compared with usual care, attention control, waitlist control, active control or another intervention. Studies were eligible if they addressed at least one of: ADL and/or BPSD. We considered BPSD in terms of the type, number or frequency of behaviours and measurement of anxiety and/or depression. Secondary outcomes included QOL for the person with dementia and their family carer, carer burden and depression. After scoping the available research, we also decided to report on family carer distress or upset. Trials had to be published in full text, peer-reviewed journals, or full reports of dissertations and could be published in any language. Conference abstracts were excluded.
Literature search and study selection
The search strategy used by the Cochrane Dementia and Cognitive Improvement Group24 to identify trials and systematic reviews for dementia was adapted and combined with relevant search terms relevant to occupational therapy for each database. We searched Medline, Embase, the Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Education Resources Information Centre, OTseeker, PEDro and clinical trial registries without restrictions to year or language, up to February 2018. An example of a search strategy for Medline can be seen as an in online supplementary file 2 figure 1. Searches of reference lists and hand searches of eight key journals were also done. A research assistant initially screened titles and abstracts to eliminate studies that were clearly ineligible. Two reviewer authors (SB and JW or KL) then independently screened the remaining studies using full-text to confirm eligibility. Disagreements were resolved by consensus or if unsuccessful, a third reviewer (LL) was consulted.
Supplemental material
Data extraction
A data extraction form was developed and used by a reviewer (SB) to extract relevant data from the included studies. This was then verified by a second reviewer (KL, LL or JW). Disagreements about the extracted data were resolved by discussion between the two authors involved in this process.
When multiple reports from the same study were found (eg, covering different measures or time-points), data were extracted from associated reports as relevant. When data were available from different time points following intervention within a single study, we referred to the first time point as ‘after intervention’ and referred to data at the second time point as ‘at follow-up’. Details of the characteristics of included studies can be seen in online supplementary file 3 table 1: Characteristics of studies.
Supplemental material
Assessment of risk of bias and quality of the evidence
Two review authors independently assessed the risk of bias in each study using the Cochrane Collaboration's risk of bias tool.25 We used the Grading of Recommendation, Assessment, Development and Evaluation (GRADE)26 approach to assess the quality of the evidence overall for risk of bias, inconsistency of results, indirectness, imprecision and other factors such as reporting bias (if sufficient trials were included in the meta-analysis). We used GRADpro software27 to tabulate this information and decisions made about the quality of the evidence. In GRADE,26 the authors start with the quality of evidence rated as ‘high’, and grade down in the presence of the factors listed above. However, authors can also grade up the confidence in the evidence some circumstances, such as when there is a large effect size.28 The GRADE26 ratings of high, moderate, low or very low, indicates how confident we can be in the effect estimates.
Data synthesis
We conducted meta-analysis if data were available within individual studies, and were in an appropriate format for this purpose. The rationale for excluding data from meta-analyses are explained in the results. We calculated effect sizes for continuous data using standardised mean differences (SMD) to enable pooling and comparison of the different outcome measures across individual studies. To facilitate interpretation of SMD we compared the SMD using Cohen’s29 rule of thumb where 0.2 represents a small effect, 0.5 a moderate effect and 0.8 a large effect. To assess statistical heterogeneity, we used the I2 statistic. An I2 value of <50% was considered indicated of relative homogeneity. Meta-analyses were still conducted in the presence of high statistical heterogeneity, but the quality of the evidence was downgraded. The random-effects model was used in all analyses due to heterogeneity between studies. No sensitivity or subgroup analyses were specified in the protocol. Funnel plots were not used to test for publication bias because there were insufficient studies included in each comparison. Data analyses were undertaken using RevMan V.5.2.30
Results
Search results
Fifteen studies14 15 17 31–42 were eligible for inclusion from a total of 9737 articles identified from database searches and other sources (see online supplementary file 4: PRISMA flow diagram). A number of these studies reported the results of different outcomes for the same study in separate reports. Therefore, this review reports on the results of the 15 studies presented across 19 articles.11 15 17 31–46 All but one study were peer-reviewed articles published in English. The remaining study was published as a dissertation and was written in German. Three of the final studies selected required consensus and involvement of a third author to determine eligibility. Most studies that we excluded when examining the full-text, were excluded because the intervention was not provided in the person’s home, or the intervention was not clearly ‘occupational therapy’ (which we defined as being predominantly (over 75%), delivered by a qualified occupational therapist or under the supervision of a qualified occupational therapist). A few studies were excluded because they were not randomised controlled trials.
Supplemental material
Study characteristics
Participants
Of the 15 randomised controlled trials included in this review, 10 trials took place in the USA15 17 31–34 39 41 and other countries included Germany,35 36 The Netherlands,14 Hong Kong,37 Wales,38 Australia40 and Brazil.42 A total of 2063 persons with dementia/family carer (majority dyads) were randomised and participated in the included studies. The majority of participants with dementia were aged over 75 years, had a medical diagnosis of mostly moderate stage dementia with Mini-Mental State Examination scores47 between 11.3 and 22.73, and needed assistance with instrumental ADL (eg, cooking, shopping, managing finances) and to a lesser extent, basic ADL (eg, toileting, bathing, dressing). Most studies did not specify the type of dementia, although one focused on frontotemporal dementia.40 There was roughly equal male/female participants with dementia when looking across all studies. The intervention was delivered to the person with dementia and the family carer as a dyad in all but one study38 that had some participants without family carers. Family carers were, on average, 65 years of age, lived at home with the person with dementia or at a minimum provided assistance or supervision to the person with dementia for several hours per week. Between 20% and 90% of carers were spouses. For further information, please refer to online supplementary file 3 table 1: Characteristics of studies.
Characteristics of interventions
All included studies utilised occupational therapy services, provided or supervised, by a qualified occupational therapist at least 75% of the time, with two trials32 33 also including some time with nurses. Most interventions were aimed at optimising the person with dementia’s involvement in ADL and/or management of BPSD. Just over half of the studies used interventions based on theory.
From the summary of the characteristics of the interventions below in table 1 it can be seen that occupational therapy comprised multiple components (as is typical of occupational therapy) and was provided across a median of eight sessions. Studies within this review used a range of different outcome measures as can be seen in online supplementary file 3 table 1: Characteristics of studies.
Summary of intervention characteristics
Risk of bias within studies and quality of evidence
Most studies explained their randomisation procedure and concealed the allocation sequence. Blinding of participants and therapists was not possible due to the nature of the studies and therefore these studies may be subject to performance bias. Although a number of trials reported using assessor blinding, most of these also used measures that were self-report and were thus still susceptible to bias. A summary of the risk of bias across different criteria can be seen in online supplementary file 5 figure 1: Risk of bias assessment. In addition, the majority had small sample sizes with the largest trial33 having 272 participant-dyads and four studies having <100 participant-dyads. The evidence was of assessed as between moderate and very low quality depending on the outcome, according to GRADE26 due to the risk of bias, inconsistent results between studies, and some imprecision (see online supplementary file 6 table 1: GRADE profile- people with dementia and online supplementary file 7 table 1: GRADE profile-carers for details).
Supplemental material
Supplemental material
Supplemental material
Synthesis of results
Effects of interventions are presented separately below for people with dementia and their family carers. All effects sizes were based on between-group differences measured after completion of the interventions, with seven studies33 35 37–39 43 44 providing data from one or more follow-up points beyond the completion of the intervention. Only data from 3-month or 6-month follow-up time points were included in the meta-analyses. No change scores were included. Thirteen studies14 15 17 31–34 36–38 40–42 compared occupational therapy with usual care or attention control and are presented first. Two studies are then presented that compared occupational therapy with another intervention.35 39
Occupational therapy versus usual care or attention control
Activities of daily living
Nine randomised controlled trials examined an occupational therapy intervention provided at home, designed to improve, maintain or slow the deterioration of ADL of people with dementia. Meta-analysis of five studies found occupational therapy was more effective than usual care14 36 40 41 or attention control32 for improving overall ADL (basic and instrumental ADL combined) after completion of the intervention (SMD 0.61, 95% CI 0.16 to 1.05; low quality evidence) (see figure 1). Considerable heterogeneity was present (I2 = 85%; p< 0.0001) which on retrospective exploration, appeared to be influenced by one study14 that reported a large effect size. We explored the consequence of omitting this trial from the analysis; removal of the trial lowered statistical heterogeneity (I2=24%) and the overall effect remained positive (SMD 0.36, CI 0.15 to 0.57) though the size of the effect was smaller. Two of these studies also measured overall ADL at a further time point.14 36 One study14 reported between-group reduction in the deterioration in overall ADL 3 months from the commencement of occupational therapy (mean difference −13.6; 95% CI 15.8 to –11.3) on the interview of deterioration of daily activities outcome which has a score range of 0–44. The other study36 that measured overall ADL using the Alzheimer's Disease Cooperative Study-Activities of Daily Living (ADCS-ADL), reported a mean between-group difference of 7.3 (95% CI 4.08 to 10.52) 3 months following commencement of occupational therapy. The effect of occupational therapy on BADL and on instrumental activities of daily living (IADL) are considered separately below.
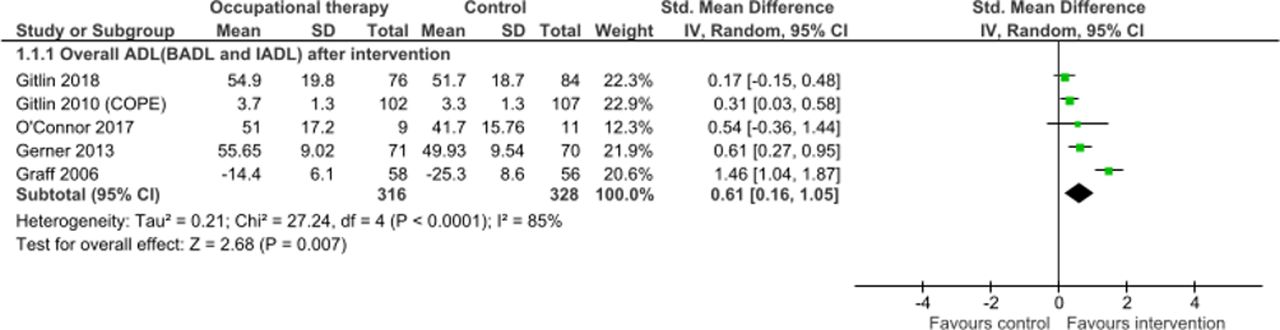
Overall activities of daily living (BADL and IADL combined). ADL,activities of daily living; BADL, behavioural and psychological symptoms ofdementia; IADL, instrumental activities of daily living.
Five studies17 31 32 40 41 measured basic activities of daily living (BADL) on its own (with some providing separate data for BADL as well as overall ADL).31 40 41 Meta-analysis found no between-group difference for BADL (SMD 0.13 95% CI −0.02 to 0.27; low quality evidence) and heterogeneity was not present. An additional study34 that provided two visits versus usual care measured BADL reported a statistically significant effect in favour of the occupational therapy intervention group but data were not available to determine effect size. Meta-analysis of five studies17 31 32 40 41 resulted in a significant, small effect size29 for occupational therapy compared with usual care for IADL (SMD 0.22, 95% CI 0.07 to 0.37; I2 = 6%) and this evidence was of moderate quality (see online supplementary file 8: Instrumental activities of daily living).
Supplemental material
BPSD—occurrence of behaviours, depression and anxiety
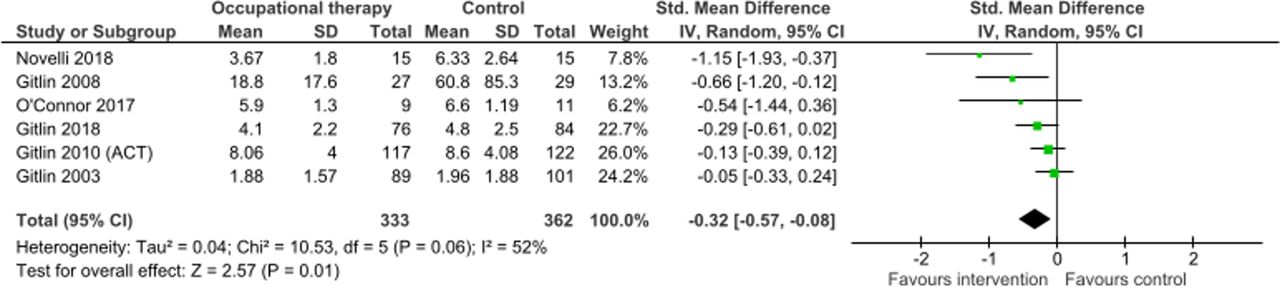
Effects of interventions are presented separately below for different aspects of BPSD. Ten studies compared the effect of occupational therapy provided at home with usual care or attention control on behavioural and psychological symptoms. Six of the 10 studies measured occurrence of behaviours or psychological symptoms in terms of the number of behavioural or psychological symptoms, with authors obtaining data for one study33 by contacting the study authors. Pooled analysis of data of these six studies15 31 33 40–42 (figure 2), demonstrated a small to moderate statistically significant between-group difference (SMD −0.32, 95% CI −0.57 to −0.08; moderate quality evidence) in the number of behavioural and psychological symptoms in favour of those receiving occupational therapy. Heterogeneity was high (I2=58%) likely reflecting the included studies application of different intervention programme with slightly different client groups. The psychological symptoms of depression and anxiety were also considered separately. Combined data from three studies15 38 44 comparing the effect of occupational therapy provided at home with usual care on depression experienced by people with dementia, yielded no significant differences between groups after the intervention (SMD −0.26, 95% CI −0.57 to 0.06; very low quality evidence). An additional study37 that did not have data in a format that could be used in the meta-analysis, found no between-group difference for depression. Two studies38 44 measured depression at a follow-up time-point. One study38 found no statistically significant effects, while the other44 reported a reduction of depression (mean difference −3.0; 95% CI −5.07 to −0.93) 3 months following commencement of occupational therapy. Anxiety in people with dementia was measured using a separate scale in only one study which found no statistically significant between-group difference.38

Number of behaviours and psychological symptoms.
QOL for people with dementia
Seven studies15 32 37 38 40 42 44 measured QOL of people with dementia, after occupational therapy intervention. Pooled analysis of six of these studies15 32 38 40 42 44 providing occupational therapy at home revealed significantly better QOL than those in the control groups (SMD 0.76, 95% CI 0.28 to 1.24) (see figure 3). A high level of heterogeneity was present (I2 = 80%) (and remained after exploring possible reasons for heterogeneity), which in addition to risk of bias, prompted downgrading of the rating of the quality of this evidence to low. At follow-up, combined data from two studies38 44 showed a large, significant result (SMD 1.07, 95% CI 0.58 to 1.55; I2=30%) (figure 3). No statistically significant between-group differences in QOL was identified in the study by Lam et al 37 either immediately following the intervention or at follow-up, but results were not in the format to be able to be included in the meta-analysis.

Person with dementia—quality of life.
Carer depression
Six studies15 33 35 38 41 44 contributed data about family carer depression. Combined, five of these trials15 33 38 41 44 yielded no statistically significant difference between occupational therapy and control groups for depression immediately following the interventions (SMD −0.33, 95% CI −0.71 to 0.04; very low quality evidence). Heterogeneity was high (I2 = 76%) which when explored, appeared to be influenced by one study44 that reported a large effect size. Combined data from three studies at either 3-month44 or 6-month follow-up33 38 found no between-group difference for depression (SMD −0.50, 95% CI −1.24 to 0.23; I2 = 87%; p= 0.16). This evidence was of low quality.
Carer burden
Four studies15 33 41 42 contributed data to the meta-analysis considering family carer burden with no statistically significant between-group difference found immediately after the intervention (SMD −0.06, 95% CI −0.31 to 0.18; I2 35%; low quality evidence). Two further studies34 37 used the Zarit Burden Interview48 but did not have data that could be used in the meta-analysis. One of these studies37 found no statistically significant difference between groups, whereas the other34 reported that family carers receiving occupational therapy had significantly lower levels of burden at post-test than carers receiving usual care. As a further measure of carer burden, three studies15 40 41 measured the hours family carers spent ‘on duty’ with no statistically significant difference between groups (SMD −0.20, 95% CI −0.46 to 0.06; I2=56%; low evidence). These three studies also measured the hours ‘doing things’ for (or providing attention to) the person with dementia which showed a statistically significant difference (SMD −0.33, 95% CI −0.58 to −0.07; I2=41%). This evidence was of low quality.
Carer distress or upset with behaviours
Data from six studies15 17 31 33 41 42 that measured the amount of upset or distress family carers felt with respect to the behaviours or psychological symptoms of the person with dementia, were combined and demonstrated a small, statistically significant result in favour of those receiving occupational therapy and this evidence was of moderate quality (SMD −0.23, 95% CI −0.42 to −0.05; I2=41%)(figure 4).

Carer distress or upset with behaviours
Carer QOL
Only three studies measured overall QOL of the family carers of people with dementia.37 42 44 Pooled data from two of these studies42 44 produced a large, significantly significant between-group difference after the intervention (SMD 0.99, 95% CI 0.66 to 1.33; I2=2%) and this evidence was of moderate quality (see figure 5). In comparison, no statistically significant between-group differences in family carer QOL was identified in the study by Lam et al 37 either immediately following the case management intervention provided by occupational therapists or at follow-up, but data were not in a format that could be included in the meta-analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Carer quality of life.
Adverse events
Two studies14 32 indicated there were no adverse events or harms related to the occupational therapy intervention. No harms were reported in the remaining studies.
Occupational therapy versus comparison intervention
Two studies compared occupational therapy provided at home for people with dementia and their family carers to either a smaller dose of occupational therapy35 or to a different intervention39 and were therefore not included in the meta-analyses described above. Their results are described here. One study35 compared 10 visits by an occupational therapist (using the same intervention described by Graff et al 14) with one-session provided by the same occupational therapy interventionists. For the comparisons group, the occupational therapist explained a 10-page leaflet and talked with participants about individual problems related to the needs of the person with dementia and their family carer. They were also given advice about staying active, maintaining social contacts and contacts with dementia services. No statistically significant between-group differences were found for persons with dementia or family carers for any outcome after completion of the intervention or at later follow-up. There were no adverse events or harms related to the occupational therapy intervention.35 The second study39 compared up to 24 sessions of occupational therapy over a 2-year period, with collaborative care. Collaborative care included individualised non-pharmacological management of behaviours and medication if needed. At the 24-month endpoint there were no between-group differences in ADL, physical function, depression, anxiety or mortality.
Discussion
This systematic review provides evidence that people with largely moderate stage dementia who commonly received between 8 and 12 hours of multicomponent occupational therapy at home (median of 8 sessions) had improvements in a number of key outcomes. They were better able to carry out overall ADL, IADL and importantly carers reported fewer behaviours and psychological symptoms, and better QOL compared with those receiving usual care or attention control. However, no clarity yet exists about the effect of occupational therapy on the specific psychological symptoms of depression or anxiety in people with dementia. Similarly, it is unclear if occupational therapy improves family carer depression. No improvement in carer burden was found using measures such as the Zarit Burden Interview,48 however, family carers reported less hours assisting the person with dementia. They also had less distress from behaviours and a large improvement in QOL. Cost-effectiveness was not a focus of this review but two studies had an additional paper reporting the interventions were cost-effectiveness.45 46 Evidence ranged from very low to moderate quality indicating that future research could impact the estimates of effect.
Strengths and weaknesses of this systematic review
This review was conducted with a high level of rigour and considered a broad range of outcomes of interest to consumers and healthcare providers. However, as with many non-pharmacological interventions, blinding participants and therapists in the individual studies could not be achieved. This introduces the potential for expectation bias that may lead to an overestimation of results.49 In most cases, due to the nature of the outcome measures, people with dementia and their family carer were providing the data thereby complicating the efforts to use blinded assessors. Karlawish et al 50 warn that there is the potential for bias to be introduced when family carers are providing proxy data for people with dementia. In future, trials could consider use of objective measures where possible (eg, performance-based measures of ADL), although this is not possible for measures such as depression and QOL. We decided to conduct meta-analyses even when heterogeneity was high, but to reflect this in the GRADE judgements about the quality of the evidence.26 For the majority of outcomes, the quality of evidence was graded down due to the risk of bias most of the included studies, and in some cases, moderate to high levels of heterogeneity. For example, there was a high level of statistical heterogeneity for the outcomes of overall ADL (postintervention and at follow-up) and for QOL of the person with dementia (postintervention). Although this review did not limit the searches by date or language, the possibility of publication bias still exists. An assessment of publication bias was not carried out, in part due to the small number of studies, and this should be taken into consideration when interpreting the results. In addition, we identified a number of eligible trials that could not be included in the meta-analyses due the data not being in a suitable format34 37 or due to use of different comparison groups.35 39 Results from the meta-analyses in this review should be interpreted with this in mind. Finally, this review focused specifically on occupational therapy provided in the home and did not include studies carried out in community-based facilities. This would be an important addition for future research.
Strengths and weaknesses in relation to other studies
To the best of our knowledge, this systematic review is the first to focus on the effects of occupational therapy deliverd in the home on ADL, BPSD and QOL for people with dementia, and to consider the effect on family carer’s QOL, burden and depression. Our review findings are consistent with results of a systematic review reported by McLaren et al 21 that focused on a range of different interventions (including but not focused on occupational therapy) designed to delay functional decline in people with dementia living in the community. It concluded that interventions covered in their review, can delay functional decline and may improve QOL for people with dementia. In addition to including more recent studies our analyses included a broader range of outcomes relevant to the primary care population. Similarly, our results extend the results reported in a systematic review by Kim et al 20 that included studies based across both the community and hospital settings, examining the effects of occupational therapy on behavioural symptoms or depression. By focusing just on occupational therapy provided in the home and examining a broader range of outcomes, this review may be more informative for primary care providers and for health professionals within the hospital system referring on to community-based care. The results of our review also correspond with the recent recommendations of the Clinical Practice Guidelines for Dementia in Australia,13 although our review has also indicated that occupational therapy reduced the number of behaviours or psychological symptoms that occurred for people with dementia (but not depression or anxiety). This review is also in line with the recommendations of the Social Economic Report of the Social Economic Council of the Ministry of the Netherlands51 that recommend that people with dementia living at home should be offered occupational therapy.
Implications for clinicians and policymakers
Referral to occupational therapy for people with moderate stage dementia and their family carers should be considered to support and optimise the person’s ability to carry out everyday activities and to improve their QOL while living at home. Occupational therapy in the studies in this review, like many approaches in occupational therapy, comprised multiple components. Therapists worked with both the person with dementia and their family carer to identify their goals, tailor and adapt activities for the person with dementia, and modify the environment in order to sustain their engagement and participation.14 31 Occupational therapists also provided support to the family carer as an individual however benefits on carer burden is still to be clarified. While efforts might be made to identify which ‘component’ of occupational therapy provides benefit, occupational therapy’s strength is in its integrated approach to analysing occupation (activity), the physical and social environment and its resources, and abilities of the individual, to guide intervention.16 Seven of the studies14 17 31 33 35 36 42 reported the training time occupational therapists needed to provide the interventions ranging from 16 to 80 hours with the median being 25 hours. Translating this research into practice will need to consider the knowledge and skill of occupational therapists involved; feasibility and preparedness of organisations to implement the use of multiple occupational therapy home visits; availability of sufficient funding or models of care that would enable multiple home visits; and awareness by other health professionals to refer to occupational therapy, where it is available.52–54 Effort to scale up use of occupational therapy provided in the home is complex and would require a well-skilled workforce, and responsive referral and funding models. This has implications for the training currently provided by occupational therapy schools and dementia-specific training organisations and the education of stakeholders about the full scope of occupational therapy practice for this client group.
Directions for future research
The maximum length of follow-up of randomised controlled trials considered in this systematic review with data available was 24 months postbaseline,39 although no statistically significant results were found. Most trials measured outcomes immediately after completion of the interventions and did not have further follow-up. Randomised controlled trials with longer follow-up, maintenance phases, accompanied by cost effectiveness studies, will allow the long-term effects of these interventions to be determined. The potential for floor or ceiling effects should also be considered in future research. It is possible that significant results for IADL but not for BADL were due to participants in the relevant studies being more independent in BADL than IADL at baseline, with less scope for improvement. Similarly in the study by Voigt-Radloff et al, 35 participants had a low need for assistance in overall ADL at outset compared with other studies14 32 leading the authors to query the presence of a floor effect. Questions remain regarding what stage of the illness trajectory people may benefit most from occupational therapy and the dosage of this intervention has not yet received sufficient attention. A number of studies in this review showed a reduction in the number of behavioural or psychological symptoms, but it was not reported which type of behavioural or psychological symptoms these most commonly were. The majority of studies that measured behaviours and psychological symptoms reported the overall number, severity or frequency of behavioural or psychological symptoms (or some combination of these), and some measured anxiety and depression separately. Trialist’s who have collected information that would allow analysis about the type of behavioural or psychological symptoms influenced by these interventions should consider publishing this additional information, even if in a journal’s supplementary files. All but one trial38 delivered the intervention to people with dementia and their family carer as a dyad and the benefit for people with dementia living alone could be investigated further. Two trials35 36 transferred the successful Dutch home-based occupational therapy programme14 into a multicentre practice context. One of these trials36 finding statistically significant benefit for ADL (but not as large an effect size) and the other35 found no statistically significant results. Replication studies will add to our understanding of these outcomes. It must also be noted that the majority of the studies in this review were undertaken in developed countries where access to occupational therapy with capacity for delivering evidence-based interventions is significantly greater than can be found in developing countries. However encouragingly, one trial42 which replicated the ‘Tailored Activity Program’ intervention in Brazil reported positive results. Testing these interventions in other contexts and cultures should therefore be an important priority for the research agenda. Finally, successful translation of complex interventions such as occupational therapy into practice needs research that is informed by knowledge translation frameworks, consults multiple stakeholder groups including people with dementia and their family carers from the beginning, and addresses questions of both effectiveness and translation.52
Conclusions
In summary, there is evidence that occupational therapy provided in the home may help optimise performance of ADL of people with dementia, reduce behaviours and psychological symptoms (but not depression and anxiety) and contribute to improving their QOL. It can also have beneficial effects on family carer’s distress with behaviours, number of hours assisting the person with dementia, and improve family carer’s QOL. However, translation of this knowledge to practice will require further research to determine the most cost-effective model of therapy, and how the challenges to its delivery might be overcome.
References
Footnotes
Contributors Conceptualisation: SB, SV-R, MG and LL. Methodology: SB, SV-R, MG and LL. Investigation: SB, JW, KL, LL (study selection), SB, KL, JW, LL (data extraction and risk of bias assessments). Formal analysis: SB (analyses), SB, LC and KL (final analyses decisions). Verification: SB, KL, SV-R, JW, LC, LL and LG. Writing: SB, JW and KL. Review and editing: SB, KL, SV-R, JW, LC, LL and LG. Project administration: SB.
Funding The first author’s contribution was partially supported by The University of Queensland, Australia. Grant number: 2007000387.
Competing interests Four authors (MG, SV-R, LC and LG) are authors of trials included in this systematic review. They were therefore not included in study selection, assessment of risk of bias or analysis. LG reports funding grants from National Institute on Aging, other from Johns Hopkins, during the conduct of the study.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.