Article Text

Abstract
Objective To assess the feasibility of implementing a dedicated feeding support team on a postnatal ward and pilot the potential effectiveness and cost-effectiveness of team (proactive) and woman-initiated (reactive) telephone support after discharge.
Design Randomised controlled trial embedded within a before-and-after study. Participatory approach and mixed-method process evaluation.
Setting A postnatal ward in Scotland.
Sample Women living in disadvantaged areas initiating breast feeding.
Methods Eligible women were recruited to a before-and-after intervention study, a proportion of whom were independently randomised after hospital discharge to intervention: daily proactive and reactive telephone calls for ≤14 days or control: reactive telephone calls ≤ day 14. Intention-to-treat analysis compared the randomised groups on cases with complete outcomes at follow-up.
Main outcome measures Primary outcome: any breast feeding at 6–8 weeks assessed by a telephone call from a researcher blind to group allocation. Secondary outcomes: exclusive breast feeding, satisfaction with care, NHS costs and cost per additional woman breast feeding.
Results There was no difference in feeding outcomes for women initiating breast feeding before the intervention (n=413) and after (n=388). 69 women were randomised to telephone support: 35 intervention (32 complete cases) and 34 control (26 complete cases). 22 intervention women compared with 12 control women were giving their baby some breast milk (RR 1.49, 95% CI 0.92 to 2.40) and 17 intervention women compared with eight control women were exclusively breast feeding (RR 1.73, 95% CI 0.88 to 3.37) at 6–8 weeks after birth. The incremental cost of providing proactive calls was £87 per additional woman breast feeding and £91 per additional woman exclusively breast feeding at 6–8 weeks; costs were sensitive to service organisation.
Conclusions Proactive telephone care delivered by a dedicated feeding team shows promise as a cost-effective intervention for improving breastfeeding outcomes. Integrating the FEeding Support Team (FEST) intervention into routine postnatal care was feasible.
Trial registration number ISRCTN27207603. The study protocol and final report are available on request.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
To pilot the potential effectiveness and cost-effectiveness of continuing proactive and reactive telephone support for breast feeding for up to 14 days after hospital discharge for women living in more disadvantaged areas.
To assess the feasibility of implementing a dedicated feeding team on a postnatal ward.
To design an effective health service intervention for infant feeding by re-organising how routine care is provided to inform a larger programme of research.
Key messages
Proactive telephone care delivered by a dedicated feeding team shows promise for increasing breastfeeding rates 6–8 weeks after birth.
Only having a dedicated feeding team on a postnatal ward did not appear to make any difference to feeding outcomes at 6–8 weeks after birth.
We have demonstrated the feasibility of (1) implementing the FEeding Support Team intervention as part of routine postnatal care and (2) the recruitment and data collection processes for a proposed definitive trial.
Strengths and limitations of this study
Using a participatory approach and embedding a rigorous randomised control trial within a before-and-after cohort study with mixed methods data to evaluate costs are strengths that will enable us to design a definitive trial.
It is likely that the effect sizes are overestimated as the sample size was small and no sample size calculation was performed prior to the study.
Our sample included women requiring longer hospital stays due to birth complications.
The reactive call service was only free to those who had the same mobile phone network provider.
The incremental cost-effectiveness ratios presented represent the most favourable set of assumptions for proactive telephone support and are sensitive to how the service is organised.
Introduction
There is increasing evidence that breast feeding improves maternal and infant health outcomes and that infant formula milk has risks for health. Accordingly, many governments support the World Health Organisation (WHO) recommendation to exclusively breast feed for the first 6 months after birth.1 International evidence syntheses report that additional professional or lay support, particularly if it spans before and after birth, can increase the exclusivity of breast feeding and to a lesser extent duration.2 3 However, the generalisability of effective interventions is uncertain, particularly where breast feeding is less prevalent.4 Multi-faceted interventions seem more effective than those with single components; however, the contribution of each component remains unclear.2 4 It has been proposed that one of the reasons why breastfeeding interventions might fail is because contact after birth is reactive (woman initiated) rather than proactive (care provider initiated).5 6
Randomised proactive telephone interventions to support breast feeding following hospital discharge have received little research attention but may increase breastfeeding duration and exclusivity.6–10 In three trials with mixed results, peer supporters have proactively telephoned women after birth using an unstructured call format.7 8 11 In two further trials, health professionals have used structured call protocols and have reported non-significant improvements in breastfeeding outcomes10 12; however, in one of the trials, intervention infants of disadvantaged, primiparous, predominantly Latina women were less likely to access health services at 1 month.10 For other health-related behaviours, for example, smoking cessation, proactive telephone support was more effective than reactive support, with a dose–response relationship.13 A systematic review of peer supporter calls for a variety of health-related issues (seven studies, 2492 participants) drew no firm conclusions, as study quality was poor, with economic and sustainability issues not addressed.14
In a UK quinquennial postal survey in 2005, 12% of UK women ceased to breast feed in the first 4 days, with 22% stopping by 2 weeks and 37% by 6 weeks, yet nine of 10 of these women would have liked to have breast fed for longer.15 Maternal age, previous breastfeeding experience and maternal disadvantage are strong determinants of breastfeeding outcome.15 UK guidelines recommend proactive targeting of disadvantaged women to improve maternal and infant nutrition outcomes.16 17 Yet health professionals have insufficient time for this; hence, intensive multidisciplinary team interventions have been proposed to address health inequalities.18 19
In this study, we followed guidance on designing complex interventions20 and conducted preliminary longitudinal qualitative research exploring infant feeding experiences of women and their significant others focusing on “what would make a difference?”21 Intervention vignettes were used as a tool in the design,21 and overwhelmingly the immediate postnatal period was seen as the time to prioritise resources compared with during pregnancy or later in infancy. Vignettes describing more help on the postnatal ward, specialised teams to provide expertise, continuity of care and additional telephone support were all viewed favourably by parents. The intervention was informed by systems and ecological behaviour change theory.22 This proposes that changing the context, system, organisation or environment to facilitate the desired behaviour might be more effective than individual cognitive behaviour change interventions, as some decisions are made automatically.23 Building on the service user perspectives, our aims were first to pilot the potential effectiveness and cost-effectiveness of continuing proactive or reactive telephone support at home for up to 14 days after hospital discharge. Second to assess the feasibility of implementing a feeding team on a postnatal ward and the processes necessary to design a definitive trial.
Methods
A participatory approach informed by the principles of action research24 was used to design, implement and evaluate the FEeding Support Team (FEST) intervention and is reported in more detail separately.25 The fixed (unchanged during the study) and flexible intervention components are summarised in box 1. Three of four components to the study are reported in this paper: a before-and-after cohort study, a pilot randomised control trial (RCT) of proactive and reactive telephone support and an economic evaluation. The fourth component is reported separately25 and describes a mixed quantitative and qualitative methods process evaluation to evaluate telephone call activity, intervention feasibility, acceptability and fidelity from the perspectives of women, the feeding team and postnatal hospital and community staff.
Fixed and flexible components of the FEST intervention
Fixed components of the randomised control trial of proactive telephone support
At least one member of the feeding team was continuously available during the intervention period 7 days a week from 13:00 to 20:00 h
On the ward, they recruited and supported trial women with breast feeding and aimed to watch a complete breast feed prior to hospital discharge
At hospital discharge, all trial women were given a leaflet with the names and photographs of the feeding team, hours of availability (13:00–20:00 h) and contact telephone number. All women were informed (written and verbal) that they could phone the feeding team at any time for up to 2 weeks after hospital discharge
Randomisation occurred after hospital discharge to:
Proactive telephone calls (intervention) daily for 1 week following hospital discharge. Calls terminated at the woman's request or if breast feeding ceased. At 1 week following discharge, women could choose to continue receiving daily calls for a further week, change the frequency of calls or have no further calls. Women could telephone the feeding team at any point over the 2 weeks following discharge. Text and answer phone messaging was available. All proactive calls stopped 14 days after hospital discharge
Reactive telephone calls (control). Women could telephone the feeding team at any point over the 2 weeks following discharge. Text and answer phone messaging was available
Qualitative interviews with women before and after the intervention, with both intervention and control women
Ward observations 2 weeks before and 2 weeks after the intervention
Flexible participatory components to implement a dedicated feeding team
A steering group of midwives, managers, public health infant feeding co-ordinator and researchers met every 4 weeks. Reflective action cycles informed by action research methods were used to investigate and decide:
The implementation process involved in establishing a multi-skilled feeding team on the postnatal ward to provide breastfeeding support and deliver proactive/reactive telephone support after hospital discharge
How the FEST team would prioritise delivering the FEST intervention to trial women participants. It was agreed that if they had spare time, they would support non-trial women living in disadvantaged areas, while they were on the postnatal ward
The composition, recruitment and appointment of the dedicated feeding team: two band 4 staff (a nursery nurse and a maternity care assistant) and a band 7 (midwife) team leader. Team rotas, meetings and handover could be flexible
How to assess women's needs and develop a triage system to provide other additional non-telephone support when required, including face-to-face assessment at a suitable place
The content of care and communication style on the ward and on the telephone were not specified other than being woman centred. Continuity of care was negotiable
Setting
The study was conducted in a maternity unit serving a mixed urban and rural population in Scotland. In 2009, there were 4863 live births, with 10.4% elective and 20.1% emergency caesarean deliveries. At hospital discharge, 54% of babies were exclusively breast fed and 6% were receiving breast and formula milk. In the most disadvantaged areas, 39% exclusively breast fed compared with 63% in the most advantaged areas (table S1). The two postnatal wards in the unit were randomised to select the study setting by a witnessed coin toss. Postnatal ward admission procedures did not change during the study and were based on bed availability, with two exceptions: women admitted to the ward when pregnant returned to the same ward following birth and all diabetic mothers were admitted to the study ward for specialist care. All postnatal ward staff (including the FEST team) had a breastfeeding induction and completed a 2-day Unicef accredited training programme.
Before-and-after cohort study
Aim: to compare the proportion of women breast feeding (any and exclusive) at 6–8 weeks after birth for the 12 weeks before and 12 weeks after providing a specialised feeding team on a postnatal ward to support women living in more disadvantaged areas who initiated breast feeding.
All women admitted to the ward who initiated breast feeding between 3 May 2010–25 July 2010 (prior to the feeding team) and 26 July 2010–18 October 2010 (during the feeding team) were eligible to be given written information by the postnatal ward staff on admission. At hospital discharge, written consent was requested by the midwife to (1) complete a short feeding questionnaire documenting socio-demographic, birth and feeding at hospital discharge details and (2) receive a follow-up telephone call by a member of the research team at 6–8 weeks after birth to collect outcome data. The outcome data collected were the same as described below for the RCT of telephone support.
RCT of proactive and reactive telephone support
Aim: to pilot the potential effectiveness and the feasibility of implementing a RCT of proactive and reactive compared with reactive-only telephone support for women living in more disadvantaged areas who were giving their baby some breast milk at the time of hospital discharge.
All women who potentially could be admitted to the postnatal ward after birth were identified from community midwife records and sent written study information when they were 32–36-week pregnant. Women admitted to the ward between 26 July 2010 and 18 October 2010 who lived in the three most disadvantaged postcode area quintiles for the Scottish Index of Multiple Deprivation (SIMD 1–3) in 200926 and who were breast feeding were potentially eligible to participate. Women aged <16 years with serious medical or psychiatric problems or with insufficient spoken English to communicate by telephone were excluded.
The feeding team gained written informed consent and then randomised women immediately after hospital discharge using a website randomisation sequence service set up by an independent statistician. Randomisation was stratified to ensure balance of primiparous and multiparous women across both trial arms. Although not informed of the randomisation outcome, women knew if they had been randomised to the proactive group as they received a phone call from the feeding team within 24 h of hospital discharge. Based on breastfeeding rates at hospital discharge (table S1) and the available feeding team working hours and funds, we anticipated randomising 60 women would be feasible in 12 weeks.
The primary outcome was any breast feeding at 6–8 weeks. The secondary outcomes were: exclusive breast feeding at 6–8 weeks, satisfaction with breast feeding help in hospital and at home, number of days readmitted to hospital (mother or baby) and contact with health professionals following hospital discharge. Outcomes were collected by telephone by a researcher who was blind to randomisation and who had no other contact with study women. No changes to outcome measurement were made during the study. Any breast feeding was defined as any breast milk given to the baby, and exclusive breast feeding was defined as no other liquids (except medicines) within the previous 24 h.27 Women were asked to score their satisfaction with the help they received with breast feeding (1) in hospital and (2) at home. They were asked to use a rating scale of 0 to 10, with 0 being the most dissatisfied and 10 being the most satisfied.
Statistical analysis
Descriptive statistics were used to summarise data from the trial and the before-and-after cohort study (number and percentage for categorical variables and mean (or median) and SD (or IQR) for continuously distributed variables. A generalised linear model with Poisson link function and robust SE was used to estimate the effect of the intervention (presented as RRs and 95% CIs) on the primary outcome: feeding at 6–8 weeks. Satisfaction with care outcomes were analysed using linear regression to estimate the difference between groups (with 95% CIs). Intention-to-treat analysis was performed on cases with complete outcomes at follow-up. All statistical analyses were undertaken using Stata V.11.2 (StataCorp. 2009. Stata Statistical Software: Release 11; StataCorp LP).
Costs and cost-effectiveness
Aim: to pilot the data collection methods for a definitive trial and the cost-effectiveness analysis of providing a specialised feeding team to deliver proactive and reactive telephone support.
Participants in the trial and before-and-after cohort answered questions on their use of healthcare resources including the number of mother and baby readmissions to hospital and contacts with community midwives, health visitors and general practitioners since hospital discharge. While these data were not formally incorporated into the economic evaluation, data completeness gave an indication of the feasibility of data collection for health economic analysis and point estimates (mean and median) with measures of variance (SD and IQRs) providing an indication about whether existing care changed as a result of the trial for either the intervention or control group. Standard sources were used to assign costs to the mean number of health visits in each group, testing the hypothesis that breast feeding may reduce costs to the NHS by reducing the number of contacts required with health professionals.
The cost per woman of providing the intervention was estimated from (1) telephone call activity data described in the process evaluation25 and (2) workload activity diaries collected over 7 days by the FEST team, recording time taken to deliver the intervention as part of usual care as well as time spent on trial research activities. This assumed that the intervention could be provided as part of regular maternity care which may not be practical as the level of time required may prevent staff from completing their regular duties to the required standards.
The mean time spent making telephone calls to and receiving telephone calls from the women was estimated from the telephone call logs.25 Costs were then assigned to this time based on the estimated mix of band 4 and band 7 staff time spent making and receiving calls and differences between the group outcomes.
Cost-effectiveness for proactive telephone support (intervention) compared with reactive telephone support (control) is presented in two ways to reflect the interests of practitioners and policy makers: as incremental cost per (1) additional woman breast feeding and (2) percentage change in breastfeeding rates at 6–8 weeks. The first measure reflects the cost-effectiveness of a 100% change in women's behaviour, whereas the latter measures a 1% change. Both measures are presented in order to report in a manner that is informative to all readers depending on their requirements in practice.
Results
Participants and feeding outcomes for the before-and-after cohort study
There were no significant differences in either the characteristics of mothers and babies or breastfeeding outcomes at hospital discharge or at 6–8 weeks comparing the 12 weeks before and 12 weeks after the intervention (tables 1 and 2) for all consenting women (including trial women), who initiated breast feeding after birth. Watching an entire breast feed was hypothesised to be an effective component of the postnatal ward intervention.21 Before the intervention, 60 of 413 (15%) women reported having an entire breastfeed watched compared with 73 of 388 (19%) after (table 1), and the reasons for this are discussed separately.25
Characteristics of all mothers and babies initiating breast feeding before and after the feeding team intervention started on the postnatal ward
Feeding outcomes before and after the feeding team intervention started on the postnatal ward
Participants in the RCT of proactive and reactive telephone support
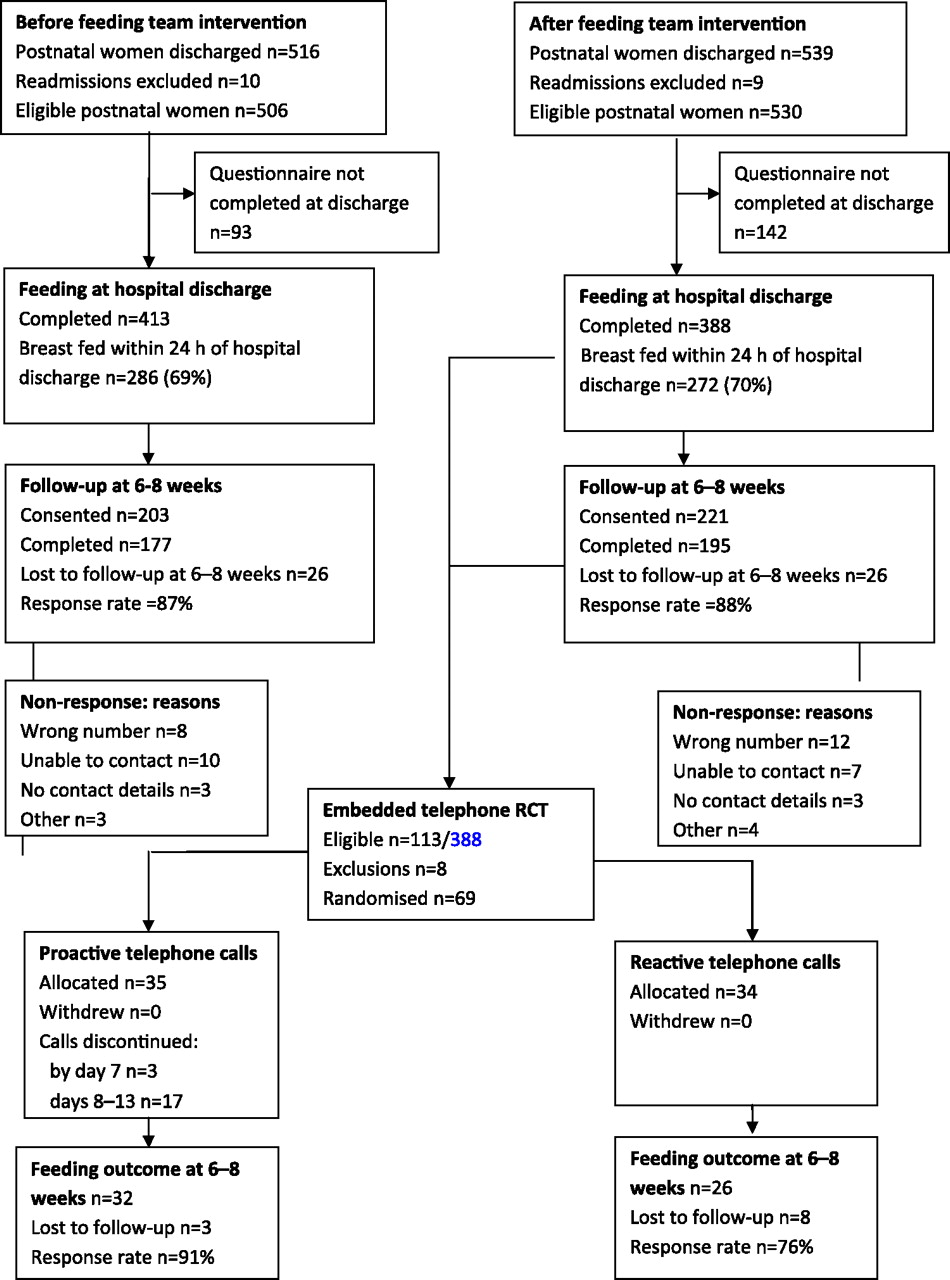
For the telephone support RCT, 69 women were randomised from 113 eligible women living in SIMD 1–3 postcode areas and who were in the cohort study (figure 1). Thirty-five women were randomised to proactive and reactive calls (intervention) and 34 to reactive calls-only group (control). At hospital discharge, 74% of women in both the intervention (n=26) and the control (n=25) groups were exclusively breast feeding (table 3). More multiparous women chose not to be randomised; otherwise, women who were randomised were similar to those who were not (table 3). This might be explained by women who have previously breast fed not anticipating the need for additional support.15

{kind=link}
FEeding Support Team randomised controlled trial flow chart.
Characteristics of mothers and babies participating in the randomised control trial of proactive and reactive compared with reactive-only telephone support for breast feeding
Women in the proactive call group were a year older on average, with more living in the most disadvantaged postcode areas (SIMD 1). Hospital stays were half a day longer on average in the proactive call group; however, data were imbalanced by a small number of women with unusually long hospital stays. Otherwise the randomised groups were similar for parity, method of delivery, gestation and admission to the neonatal special care unit. Comparing women in the study with the 2009 birth statistics available for the hospital, study women had more elective caesarean sections (10% in 2009) and fewer emergency caesarean sections (20% in 2009) with the total number of caesareans remaining similar at 30%. Only 28 (41%) trial women were recorded as having an entire breastfeed observed (table 3) but reporting was incomplete with information missing in 25% of randomised women. Qualitative data about the challenges of observing an entire breast feed on the ward are reported elsewhere.25
Feeding outcomes for the pilot RCT of proactive and reactive telephone calls
Women who received proactive telephone calls from the feeding team were more likely to be giving their baby some breast milk at 6–8 weeks after birth (RR 1.49, 95% CI 0.92 to 2.40) than those who received no feeding team initiated calls, but this difference was not statistically significant (table 4). For women receiving proactive calls, 22 of 32 (69%) women followed up were giving their baby some breast milk at 6–8 weeks compared with 12 of 26 (46%) women followed up in the control group. At 6–8 weeks, 17 of 32 (53%) women receiving proactive calls were giving their baby exclusively breast milk compared with eight of 26 (31%) women in the control group (RR 1.73, 95% CI 0.88 to 3.37). There were missing data for the primary trial outcome at 6–8 weeks, three of 35 (9%) in the proactive call group and eight of 34 (24%) in the control group. Reasons for non-participation in the trial were documented for 14 of 44 women: exclusion due to language difficulty (n=3), leaving the area (n=1), unwell baby in the neonatal unit (n=4) and maternal choice (n=6) with qualitative interview data reported separately.25
Mother and baby outcomes in relation to proactive and reactive compared with reactive-only telephone support for breast feeding
For the secondary outcomes, there were no significant differences in women's reported satisfaction with the breast feeding help they received either in hospital or at home, and overall levels of satisfaction were high (table 4).
Costs and cost-effectiveness
Detailed costs split by telephone25 ward contact and case note/discussion time are presented in table 5. The costs presented refer to a situation where the service is implemented as part of routine postnatal ward care. Other costs that may be incurred, such as the cost of time providing routine care to non-trial participants on the ward, are excluded from the analysis as they are not expected to impact on incremental costs and, hence, will not influence the calculation of incremental cost-effectiveness ratios. Data differentiating activities between the intervention and control groups were available for telephone calls25 and case note transcripts, with the latter on average 2.6 times longer for intervention than control women. We have assumed that time spent on research activities and helping women on the ward was similar between the intervention and control groups. This will likely cause a small bias in favour of the intervention in our quoted cost-effectiveness results.
Costs of the telephone intervention per woman for each randomised group
Table 6 illustrates the main cost-effectiveness results for delivery of the intervention with the cost data relating to the same scenario as considered in table 5 and estimated in the same manner. In practice, the cost per woman of providing proactive telephone calls was £41.25 and £21.13 per woman for reactive calls, as only one woman called the team. For any breast feeding at 6–8 weeks, the incremental cost of providing proactive calls was £87 per additional woman; equivalent to £0.87 per 1% increase. For exclusive breastfeeding at 6–8 weeks: £91 per additional woman; equivalent to £0.91 per 1% increase. These costs are sensitive to the organisation of the service. Alternative intervention costing scenarios, varying staff requirements and period of coverage are presented in tables S2 and S3, using band 4 and band 5 grade nurse support, respectively, over varying hours of coverage per day.
Cost-effectiveness results for women in the randomised control trial of proactive and reactive compared with reactive-only telephone support for breast feeding
In terms of the feasibility of collecting trial data for healthcare resource use, outcome data were collected for: 56/69 (81% of all trial participants), 25/34 (74% of the control group) and 31/35 (89% of the intervention group). Point estimates of mean contact with healthcare professionals indicated that women in the proactive group may have had fewer contacts with health professionals in primary care (table 4); however, these estimates have very large standard deviations and are highly uncertain. The reader should exercise caution in interpreting such data as sample sizes are small and not all women provided complete data and the proportion that provided complete data is not equal across groups.
Discussion
The proportion of women breast and formula milk feeding and exclusive breast feeding was higher in the proactive telephone group at 6–8 weeks, but uncertainty about effectiveness exists as reflected in the width of the CI. This is to be expected in a pilot study of this size; however, the effect size does represent a clinically important difference that is worth pursuing in a large-scale pragmatic trial, particularly as previous UK trials have not significantly improved breastfeeding outcomes.4 The feeding team on the ward did not appear to have any impact on breastfeeding outcomes for all women initiating breast feeding when comparing the 12 weeks before and after the intervention. There were several contributing factors: the team prioritised care to the 69 trial women, observing an entire feed was difficult to implement,25 the median length of stay on the ward was 2 days and with limited daytime team availability there may have been insufficient team time with women to impact on the 30% who decided to stop breast feeding prior to hospital discharge. The rates of breast feeding at 6–8 weeks after birth both before and after the FEST team intervention are consistent with routinely collected data in Scotland.28
The participatory approach, embedding a rigorous RCT within a before-and-after cohort study and using mixed methods to evaluate implementation processes, costs and the feasibility of recruiting and collecting data are strengths that will enable us to design a definitive trial. However, it is likely that the effect sizes are overestimated as the sample size was small and as is common for pilot studies no sample size calculation was performed prior to the study. The underlying rate of breast feeding from the before-and-after cohort data and the risk ratios from the pilot RCT will inform the calculation of the sample size required for a definitive trial. For a definitive trial, alternative methods of collecting feeding outcome data will be considered, as loss to follow-up differed between the intervention and the control arms and is a potential source of bias. One option would be to access routinely collected infant feeding data at 6–8 weeks,28 which only became available in NHS Grampian after the FEST study had started. The logistics of recruiting and collecting data in a busy clinical setting with limited resources did burden postnatal ward staff, and as reported by others, a dedicated research assistant available at all times would probably improve baseline data collection by minimising missing data.29 Our sample included more women requiring longer hospital stays due to complications as women with uncomplicated births went home directly from labour ward; however, women with complications may be those most in need of extra support with feeding. In a larger trial, however, recruitment should be extended to include women discharged home from the labour ward. For more disadvantaged women, the cost of calls is an issue and due to the limited study resources, the reactive call service was only free to those with the same mobile phone network provider. The call activity data and factors contributing to the observed differences between the intervention and control arms are discussed in detail separately.25
The incremental cost-effectiveness ratios represent the most favourable set of assumptions for proactive telephone support. Specifically, costs are based only on those resources directly used to provide proactive telephone support. This is equivalent to making an assumption of perfect divisibility of resources, which may not be realistic. The use of activity data25 to develop a measure of cost-effectiveness for an average woman may be biased as the cost estimates might underestimate those incurred in practice and needs further investigation. Further research is required to test whether potential differences in reduced healthcare contacts are significant and whether proactive telephone support can reduce cost burden to the NHS.
This FEST intervention combined structural changes in service delivery with generic, targeted and clinical process interventions.30 FEST changed the roles and routines of postnatal care through use of the telephone and division of labour. It suggests that a dedicated team of trained lower grade staff, managed by a midwife are capable of delivering effective breastfeeding care. Structural changes protected the time given to women both on the ward and by telephone. In particular, focusing on organisational change rather than on how individual women behave is a strategy which can counteract women's perceptions of feeling ‘pressurised’ or ‘to blame’ when they choose not to breast feed.21
Conclusions
We have found that for women living in more disadvantaged areas, proactive daily telephone calls, delivered by a dedicated feeding team show promise for improving breastfeeding outcomes for a small additional cost. The data collection methods and the implementation of the FEST intervention into routine postnatal ward care were feasible and FEST now requires testing in a definitive multicentre trial. Further research prior to implementation is crucial as dedicated feeding teams would have widespread implications for the working lives of midwives, other staff and resources as well as women, and unanticipated consequences from such a change in service delivery are likely.
Acknowledgments
We would like to thank all the women, NHS Grampian staff, committee members and colleagues who have made this study possible. In particular research team colleagues: Gladys MacPherson (data management), Dale Sherriff (telephone data collection, staff interviewing and data entry), Karen Arnold (qualitative interviews and ward observations) and Diane Collins (data entry); steering group members: Liz Treasure, Lynn Catto, Susi Michie, Jenny McNicol, Tracy Humphrey, Rachel McDonald, Lesley Mowat, Joanne Riach, Eilis Pendlebury, Katrina Dunn, Lesley Kentish and the NHS Grampian Public Health and Planning Directorate, Infant Feeding Workstream Group. The Health Services Research Unit and the Health Economics Research Unit are supported by the Chief Scientist Office (CSO) of the Scottish Government Health Directorates.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
To cite: Hoddinott P, Craig L, Maclennan G, et al. The FEeding Support Team (FEST) randomised, controlled feasibility trial of proactive and reactive telephone support for breastfeeding women living in disadvantaged areas. BMJ Open 2012;2:e000652. doi:10.1136/bmjopen-2011-000652
Contributors PH had the idea for the study, and all the people acknowledged were involved in the design of the study. GM conducted the statistical analysis; DB and LV led the health economic data analysis with PH and LC contributing to the analysis of relevant qualitative data. LC and Karen Arnold conducted interviews with women participants. LC, Dale Sherriff and PH conducted interviews with staff. All authors had full access to anonymised data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. PH wrote the first draft of the paper and all authors made important intellectual contributions to the content and approved the final version.
Funding This study was funded by NHS Grampian through the Scottish Government: nutrition of women of childbearing age, pregnant women and children under 5 years in disadvantaged areas—funding allocation 2008–2011, NHS Health Scotland (http://www.sehd.scot.nhs.uk/mels/CEL2008_36.pdf). NHS Grampian and the University of Aberdeen worked in partnership to implement the study. PH is employed by the University of Aberdeen and as a General Practitioner with NHS Grampian. All evaluation was conducted by University of Aberdeen employees.
Competing interests None.
Patient consent Obtained.
Ethics approval North of Scotland Research ethics committee approved this study on 19 April 2010, ref: 10/S0801/22.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A final report of this research is available on request from PH.