Article Text

Abstract
Objectives The aim of this study was to evaluate by meta-analysis the current level of evidence in order to establish the impact of a platelet transfusion on survival in patients on pre-injury antiplatelet agents who sustain an intracranial haemorrhage (either spontaneous or traumatic).
Design This was a meta-analysis; the MEDLINE Database was searched using the PubMed interface and the Ovid interface. CINAHL and EMBASE Databases were also searched. The search was performed to identify randomised controlled trials (RCT)'s case-controlled studies or nested case-controlled studies. Comparing the outcome (death or survival) of patients with intracranial haemorrhage (ICH) and pre-injury antiplatelet agents who received a platelet transfusion against a similar cohort of patients who did not receive a platelet transfusion.
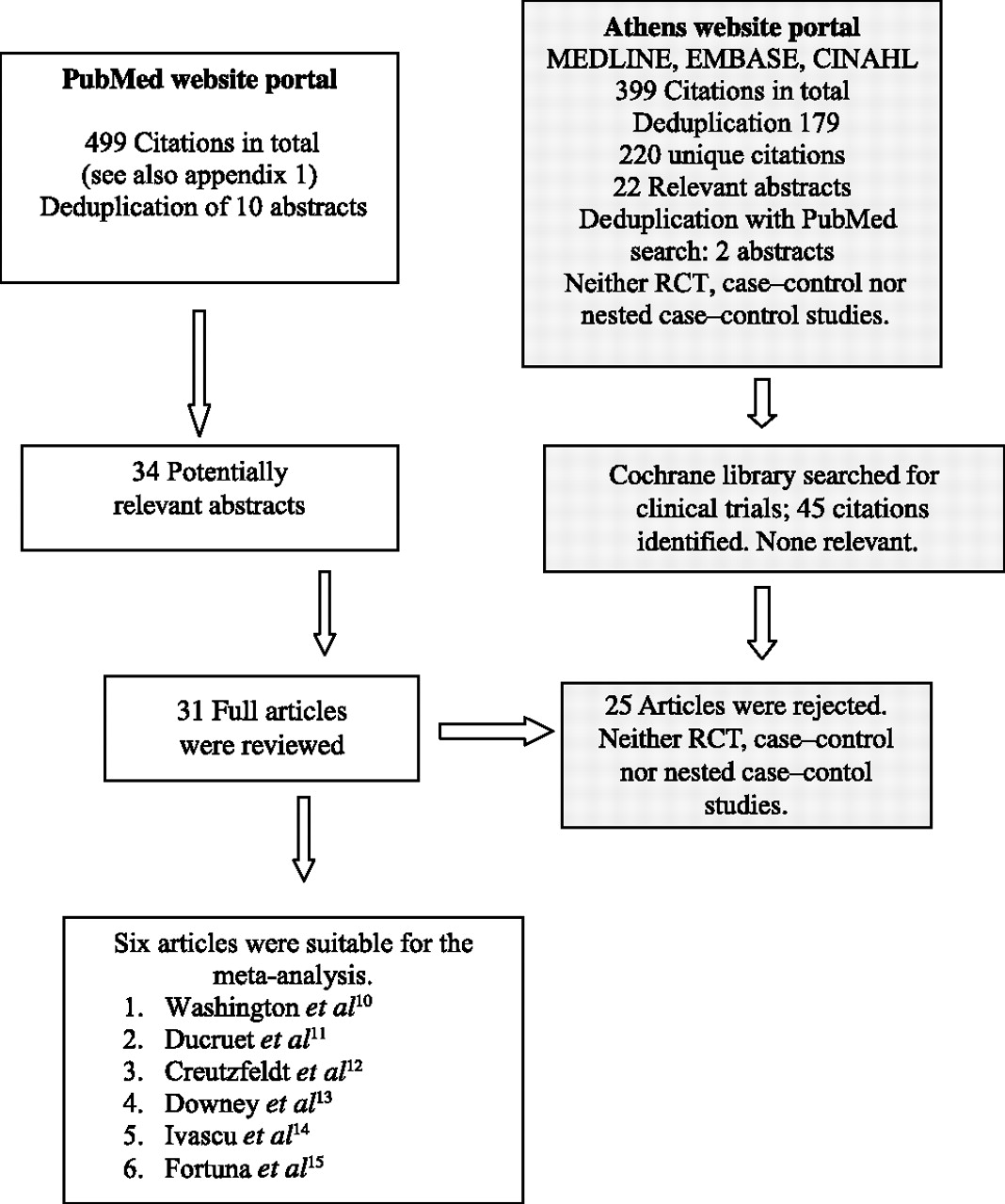
Results 499 citations were obtained from the PubMed search. 31 full articles were reviewed from 34 abstracts. 6 studies were found suitable for the meta-analysis. No randomised controlled studies were identified. 2 of the six studies were in patients with spontaneous ICH. The remaining four studies were in patients with traumatic intracranial haemorrhage. Significant heterogeneity was present between the studies, I2=58.276. The random effects model was therefore the preferred model, this produced a pooled OR for survival of 0.773 (95% CI 0.414 to 1.442).
Conclusions The results of this meta-analysis has shown, based upon six small studies, that there was no clear benefit in terms of survival in the administration of a platelet transfusion to patients with antiplatelet-associated ICH. Further work is required in order to establish any potential benefit in the administration of a platelet transfusion in patients with spontaneous or traumatic intracranial haemorrhage who were on pre-injury antiplatelet agents.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
The aim of this meta-analysis was to determine the impact on survival of a platelet transfusion in patients on pre-injury antiplatelet agents with:
Traumatic intracranial haemorrhage following blunt head trauma.
Spontaneous ICH.
Key messages
Six studies were found to be suitable for the meta-analysis (two studies for spontaneous ICH and the remaining four were traumatic intracranial haemorrhage).
The pooled OR showed no benefit in survival following a platelet transfusion (OR=0.773, 95% CI 0.414 to 1.442).
Strengths and limitations of this study
The studies were small, unpowered and not randomised.
Mortality is a relatively crude marker of effect in the cohort of patients with either spontaneous or traumatic haemorrhage.
Significant bias may have been introduced in view of the fact that in all but one study, the platelet transfusions were given at the discretion of the attending physician.
Introduction
Antiplatelet agents, in particular aspirin and clopidogrel, are an essential component of treatment and prophylaxis for both cardiovascular disease and cerebrovasular; however, they are both associated with a small risk of intracranial haemorrhage (ICH). He et al1 performed a meta-analysis of 16 clinical trials and showed that aspirin treatment was associated with an absolute risk increase of haemorrhagic stroke of 12 events per 10 000 persons (95% CI 5 to 20, p<0.001). With regard to traumatic intracranial haemorrhage (TICH), early studies in this field (Mack et al2, Spektor et al3, Jones et al4) failed to demonstrate antiplatelet agents as a risk factor for ICH in patients with blunt head trauma. Fabbri et al5 undertook a cohort study looking at predictors for ICH on a database of 14 288 head injury patients. These authors found using multivariate logistic regression that the combination of age over 65 years and the use of antiplatelet agents statistically increased the risk of ICH in their model. Pre-injury use of antiplatelet agents alone was found to have an OR of 1.2 (95% CI 0.9 to 1.7, p=0.202). Thus, it may well be that the combination of increased age plus use of antiplatelet agents rather than antiplatelet agents in isolation increases the risk of TICH as suggested by Fabbri et al.5
McMillan and Rogers6 proposed a protocol for the administration of a platelet transfusion in patients with TICH who were on pre-injury antiplatelet agents. The authors, however admit, in their own review that the evidence for this approach is lacking. A systematic review by Beshay et al7 provided an overview of the pharmacology of antiplatelet agents in the setting of intracranial haemorrhage. Cambell et al8 also provided a protocol for correcting platelet dysfunction in antiplatelet-associated ICH. These authors also recognised that the current evidence for this approach is limited. The administration of platelet transfusions is practiced in some trauma centres for traumatic antiplatelet-associated ICH. The aim of this study was to evaluate by meta-analysis the current level of evidence in order to establish the impact of a platelet transfusion on survival in patients on pre-injury antiplatelet agents who sustain an intracranial haemorrhage (either spontaneous or traumatic).
Methods
The MEDLINE Database was searched using the PubMed interface. The following search terms were used: (1) Head injury AND antiplatelet agents. (2) Intracranial haemorrhage AND platelet transfusion. Case–control and nested case–control studies comparing the cohort who were given platelet transfusions against the cohort who had not were included in the meta-analysis. The search strategy was run several times during the development of the paper in order to ensure that all the relevant papers were captured up to the date of submission. The final PubMed search was performed on 30 November 2011. The Athens website was also used to search the UK MEDLINE Database, EMBASE and CINAHL Databases. The search was performed on 30 November. A full review of the search strategy is provided in online appendix 1. No limits were placed on the search using either the PubMed portal or the Athens portal with regard to year range, age range or language. Third, a search for randomised controlled trials was performed using the Cochrane Database. A full review of the search strategy is provided in online appendix 1.
Selection criteria were broadly based upon MOOSE,9 methodology. Inclusion criteria were (1) randomised controlled trials comparing patients with aspirin-related ICH (spontaneous or traumatic) who were treated with a platelet transfusion compared with those with aspirin-related ICH who were not treated with a platelet transfusion. (2) Case–control studies comparing mortality rates of adult head injury patients on antiplatelet agents (with ICH) who received a platelet transfusion versus mortality rates of adult head injury patients on antiplatelet agents (with ICH) who did not receive a platelet transfusion. No lower limit was placed on the size of the study groups in either the case–control or nested case–control studies. (3) Cohort studies with a nested case–control group comparing mortality rates of adult head injury patients on antiplatelet agents (with ICH) who received a platelet transfusion versus mortality rates of adult head injury patients on antiplatelet agents (with ICH) who did not receive a platelet transfusion. (4) Case–control studies or nested case–control studies comparing mortality rates of adult patients on antiplatelet agents with spontaneous ICH who received a platelet transfusion versus mortality rates of adult patients on antiplatelet agents with spontaneous ICH who did not receive a platelet transfusion. No lower limit was placed on the size of the study groups in either the case–control or nested case–control studies. Appraisal of the abstract titles for relevance was made by JSB and AG. All full papers were reviewed by JSB and AG.
Articles were eligible for inclusion from any language provided that they were published in peer-reviewed journals. Exclusion criteria: (1) case–control or cohort studies where patient transfusion was used to correct a generalised coagulopathy. (2) Case–control or nested case–control studies in patients with ICH from thrombocytopaenia. All the abstracts and full papers reviewed were in English language and therefore problems with translation were not encountered. Conference proceedings were not included in the search strategy nor was a search for unpublished data performed. Contact was not made with authors of any of the studies, and the data were extracted directly either from the abstract or the full text.
Statistical analysis was performed using Comprehensive Meta-analysis V.2 (http://meta-analysis.com; Biostat Inc.). Forest plots were produced for the studies with respect to mortality. Heterogeneity between studies was performed using the I2 test.
Results
Six studies were identified which were found to be suitable for the meta-analysis. Two studies were case-controlled studies in patients with spontaneous ICH and the remaining four studies were in patients with TICH. No completed randomised controlled trials were identified. The inclusion and exclusion PRISMA flow diagram is shown in figure 1. A more detailed summary of the results of the search strategy is shown in online appendix 1.

The PRISMA flow diagram.
Characteristics of included studies
Washington and colleagues10 from Missouri retrospectively reviewed 1101 patients presenting to their level one trauma centre over a 2-year period with minor traumatic brain injury (TBI) (Glasgow Coma Scale (GCS) ≥13). Of these, 321 had TICH and 113 (35.2%) were on pre-injury antiplatelet agents. The two groups were similar at baseline in terms of age and presenting GCS. Primary outcome measures were neurological decline, Glasgow Outcome Scale, surgical intervention and mortality. Platelet transfusion was given according to physician discretion, introducing a risk of bias. The transfused group had a higher Marshall score, reflecting a larger haematoma volume (20.6±26.5 vs 8.2±13.7; p=0.02), at presentation. There were significantly more patients in the transfused group taking clopidogrel compared with the non-transfused group (52% vs 20%, p=0.0005). They found no statistically significant difference in outcome between the groups; they did find a trend towards significance for medical decline (defined a priori as an increase in the delivered level of monitoring or intervention because of cardiac, pulmonary or renal decline). Mortality rates were not significant between the two groups (2/44 (5%) vs 0/64 (0%)). They did, however, find that of all the TBI patients included, any patient receiving a transfusion (n=65, 20%) had a significantly higher mortality (6% vs 0%, p<0.0001) and OR of medical decline (5.8, 95% CI 1.2 to 28.2).
The study by Ducruet et al11 was a retrospective cohort study of 66 patients admitted to a neurological ICU with a primary ICH while on antiplatelet agents. One hundred five of the 121 patients were on aspirin alone and 11 of the 121 patients were taking aspirin and clopidogrel. Of the remaining five patients, two were on dipyridamole and the final three not specified. Of these, 35 (53.8%) received a platelet transfusion. The primary outcome measure was to detect a 25% difference in haematoma expansion from the CT on admission between the platelet-transfused group and the non-transfused group. Other outcome parameters were the modified Rankin Score on discharge, mortality rate and the rate of systemic complications. The indications for giving a platelet transfusion were not available to the investigators, although the assumption was that a platelet transfusion was given at the discretion of the attending physician. This may introduce an element of bias into the study and is to the detriment of the paper. The groups were well matched with regard to age (p=0.597) and mean GCS (p=0.992). The mortality rate in the treatment group was half than that in the non-treatment group; however, due to the small numbers (2/35 (5.7%) vs 4/31 (12.9%)), the result did not reach statistical significance. They also noted no statistical significance in either initial or final haematoma volume (initial volume (ml) 30.9±28.3 vs 27.7±25.4, p=0.63; final volume 33.9±32.6 vs 33.1±30.8, p=0.92), length of stay or discharge modified Rankin score (4.1±1.3 vs 4.5±0.9). The study did suggest a trend towards increased mortality (23.1% vs 6.1%, p=0.10) and haematoma expansion (35.7% vs 11.8%, p=0.034) in patients taking clopidogrel rather than those taking aspirin alone.
The Creutzfeldt study12 was a single-centre retrospective study of 368 consecutive patients with spontaneous ICH over 2 years admitted to a primary stroke centre. Of these, 121 (31.3%) were taking antiplatelet agents (aspirin 105, clopidogrel 3, aspirin + clopidogrel 11, aspirin + dipyridamole 2). The primary outcome measure was hospital death. Secondary outcome measure was favourable outcome. This study was again well matched for age (70 vs 71, p=0.65); however, median GCS (13 (9–15) vs 11 (6.5–14), p=0.1) was lower at presentation, suggesting that some of the group not receiving a platelet transfusion were deemed unsalvageable and palliation was the preferred treatment pathway, as reflected by the increased Do Not Attempt Resuscitation order frequency (34% vs 44%). The indications for using a platelet transfusion were also not available to the investigating authors, and again, it must be assumed that this was given at the discretion of the attending physician with the caveats described above. The mortality rate in the control group (38%) was quite high in comparison to the other studies. In the intervention group all 14 patients died, withdrawl of tretament was performed presumably due to futility of continuing active management. Due to the small size of the study, the difference in the mortality rate between the study group and the control group did reach statistical significance (p=0.17).
The study by Downey et al13 was a retrospective review over 4 years in two level 1 trauma centres. They identified 328 patients over 50 with TBI on pre-injury antiplatelet therapy of whom 166 (50.6%) received platelet transfusion. Primary outcome measure was mortality. Secondary outcome measure was length of hospital stay. The two groups were well matched with respect to the presenting GCS (p=0.96) but not with respect to age. Patients who received a platelet transfusion were older than the control group (p=0.001). This may reflect the increased prevalence of cardiovascular and cerebrovascular disease in a more elderly population. Thirty-one patients received a platelet transfusion at the discretion of the attending surgeon at one centre. At the second study centre, 135 patients received a platelet transfusion as part of a routine procedure if the Platelet Function Analyzer (PFA)-100 screening test showed evidence of platelet dysfunction. There was little difference in mortality between the treatment group and the control group (17.5% vs 16.7%). Additional confounders include the higher rates of both warfarin use (89% vs 80%, p=0.038) and clopidogrel use (45% vs 14%, p<0.001). Unfortunately, the data as described do not allow separation of these two groups. The warfarin group had an increased mortality (27.5% vs 15.2%, p=0.032) and the clopidogrel group did not (15.5% vs 17.7%, p=0.62), which contradicts the findings of the later study by Creutzfeldt et al.12
The Ivascu study14 was a retrospective review of a trauma registry over a 5-year period of patients with ICH who were taking pre-injury antiplatelet agents. In total, 109 patients were identified: 61 patients were on aspirin, 17 patients were on clopidogrel and 31 patients were on both. Of these 109 patients, 40 (36.7%) were given a platelet transfusion, again at the discretion of the attending physician. The primary outcome measure was mortality. The cohort of patients in this study were reasonably well matched with regard to age (p=0.593) and presenting GCS (p=0.332). The Injury Severity Score was slightly higher in the transfusion group than in the control group (23.4±9.8 vs 20.3±6.7, p=0.183). This may be the explanation for the sizeable difference in the mortality between the two groups with the higher mortality being in the transfusion group (27.5% vs 13.0%, p=0.064), as may also explain the increased proportion in the transfusion group operated upon compared with the non-transfused group (9/40 (22.5%) vs 8/69 (11.5%)), p=0.137).
The Fortuna study15 was a retrospective review of patients with TBI aged over 50 years in a single, tertiary, level 1 trauma centre. They identified 521 patients fitting these criteria but acknowledge that they did exclude patients in whom the medical records were incomplete. Of the 521 patients, 166 were taking pre-injury antiplatelet and anticoagulant therapy. One hundred and twenty-six patients were taking antiplatelet agents (17 clopidogrel, 91 aspirin and 18 were taking both). Twenty-nine patients were taking warfarin and 11 patients ‘other’ unspecified medication. Sixty-six (39.8%) of these 166 patients received a platelet transfusion during their stay. Patients receiving a platelet transfusion were older (73±2 vs 69±1, p=0.02), had a lower initial GCS (11±1 vs 13±0.2, p=0.004), a higher initial Injury Severity Score (ISS) (28±1 vs 24±1, p=0.001) and a longer length of stay (12±2 vs 7±0.4 days, p=0.007); all these may have contributed to the higher mortality (20/66, 30.3%) compared with those in the group which did not receive a platelet transfusion (16/100, 16%). As with many of the preceding papers, the platelets were given at the discretion of the attending physician.
A comparison of the studies by age, mean GCS and mortality rates are provided in tables 1–3, respectively.
Comparison of studies by mean age
Comparison of studies by mean Glasgow Coma Scale (GCS)
Mortality rates for the six studies
Meta-analysis data
Forest plots were produced for the mortality rates in the intervention (transfusion) and control groups (figure 2). Separate Forest plots were produced for traumatic and spontaneous ICH. These are included as figures 3 and 4. Significant heterogeneity was present between the six studies, I2=58.276; therefore, the random effects model was the preferred model and this produced a pooled OR for survival of 0.773 (95% CI 0.414 to 1.442). The fixed effects model was also evaluated and this was found to produce a similar results (common OR for survival: 0.798, 95% CI 0.559 to 1.139). The fixed effect model for the spontaneous-only group produced a pooled OR of 1.825 (95% CI 0.892 to 3.744). The fixed effect model for the trauma-only group produced a pooled OR of 0.609 (95% CI 0.404 to 0.917).

The forest plot for the six studies. Random effect model.
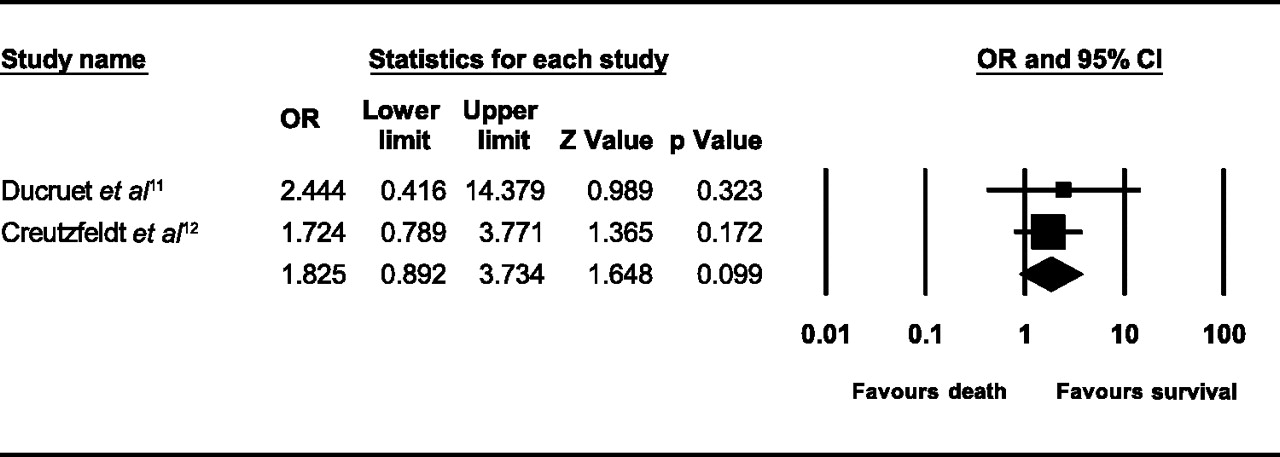
Forest plot for the two spontaneous intracranial haemorrhage studies. Fixed effects model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for the four traumatic intracranial haemorrhage studies. Fixed effects model.
Discussion
Six studies were identified for the meta-analysis, two studies evaluating patients with spontaneous ICH and four with TICH. Combining the data from all studies, there was no evidence of benefit, with a trend towards decreased survival in patients selected for a platelet transfusion. All six studies were relatively small in size, this combined with the difference in pathophysiology of traumatic ICH and spontaneous ICH makes any clear conclusions prohibitive.
When the data for TICH are extracted separately, platelet transfusions appear to have a negative effect on survival 0.609 (95% CI 0.404 to 0.917). The paper by Downey et al13 had the greatest weight in the meta-analysis data because of its greater numbers. The paper by Downey et al13 was judged by both authors to be the weakest due to differing protocols followed on either site (treatment at physician discretion vs treatment according to platelet function). If this paper is removed, the risk of survival from platelet transfusion decreases further (OR 0.387, 95% CI 0.216 to 0.694); how much weight can be given to this due to the reduction of patient numbers by 46% is unclear. The fact that platelet transfusions were given at the discretion of the attending surgeon does add significant bias into the meta-analysis. Although the studies were reasonably controlled with respect to presenting GCS, other factors such as increased haematoma volume or associated co-morbidity may have contributed to the worse outcome in the platelet transfusion group rather than the platelet transfusion itself. There may be a caveat for transfusing patients on antiplatelet agents who have sustained a traumatic ICH, although further work is required in this area.
Conversely, patients with spontaneous ICH showed a trend towards benefit from platelet transfusion (OR 1.825, 95% CI 0.892 to 3.734). This was despite the small study numbers and allocation of patients at physician discretion, possibly introducing a positive bias in terms of both severity and therefore presumed survivability. With the assumption that patients considered more likely to survive were more likely to be given a platelet transfusion and vice versa. A subgroup analysis, Ducruet et al,11 also showed that in the subgroup of patients on clopidogrel, there was an increased mortality and an increase in haematoma expansion.
With regard to spontaneous ICH, three important papers relevant to this subject need to be discussed. Sansing et al16 undertook a retrospective cohort study on 282 patients with spontaneous ICH, 70 patients were on antiplatelet medication. The authors found no difference between the antiplatelet medication group and the no antiplatelet group with regard to volume of ICH on CT, haematoma growth or outcome score. Naidech et al17 performed a cohort study on 68 patients with spontaneous ICH who were either on antiplatelet agents or had laboratory evidence of reduced platelet function. A platelet transfusion was administered in 16 patients at the discretion of the attending physician. The authors found that there was no difference in the modified Rankin Scale at 14 days, 28 days and 3 months between the transfused group and the non-transfused group. Naidech et al18 published their findings from a prospective cohort study on 45 patients with spontaneous ICH and reduced platelet activity. The cohort was divided into high risk for haemorrhage growth grade and non-high-risk patients for haemorrhage growth. High-risk patients received a CT and platelet transfusion within 12 h of symptom onset. Non-high-risk patients received a CT and platelet transfusion after 12 h. The authors found that for the high-risk group platelet transfusion within 12 h resulted in smaller haemorrhage size and better outcome (modified Rankin Score) compared with the cohort of patients who received a platelet transfusion after 12 h. Further work is required in some of these areas, in particular to clarify the effect of pre-injury antiplatelet agents on haematoma size and progression.
With regard to the traumatic ICH cohort, a relevant paper was published by Bachelani et al.19 Theses authors performed a nested case–control study comparing aspirin-associated TICH against a control group of non-aspirin-associated ICH. The Aspirin Response Test (ART; VerifyNow) was performed on all patients. Patients with an ART <550 received a platelet transfusion. Eleven patients in the non-aspirin control group (n=48) had an ART evidence of platelet inhibition and consequently received a platelet transfusion. Two patients in the aspirin group (n=36) had no ART evidence of platelet inhibition and therefore did not receive a platelet transfusion. The data were therefore not suitable for this meta-analysis. Bachelani et al,19 however, found no difference in mortality between the aspirin group and the non-aspirin group.
Conclusions
The small size of the six studies none of which were powered to demonstrate a difference in survival clearly means that no firm conclusions can be drawn from this meta-analysis. Except for the study by Downey et al,13 platelet transfusion in the remaining studies were given at the discretion of the attending surgeon. The current low level of evidence has prompted a multiple centre randomised control trial based in the Netherlands, The PATCH study,20 in order to address the potential efficacy of platelet transfusion in patients with antiplatelet-associated ICH. The end points of the study are safety of platelet transfusion and haematoma progression. Further work is clearly required on this subject so that the efficacy of platelet transfusion in spontaneous or traumatic ICH can be fully evaluated.
Acknowledgments
The authors would like to thank Katherine Wylie Senior Informaticist, Department of Emergency Medicine, Manchester Royal Infirmary, for her assistance with the Cochrane Search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
- Data Supplement - Manuscript file of format pdf
Footnotes
To cite: Batchelor JS, Grayson A. A meta-analysis to determine the effect on survival of platelet transfusions in patients with either spontaneous or traumatic antiplatelet medication-associated intracranial haemorrhage. BMJ Open 2012;2:e000588. doi:10.1136/bmjopen-2011-000588
Contributors JSB reviewed all the abstracts, reviewed all the full papers, performed the statistical analysis and wrote the paper. AG also reviewed all the abstract titles for relevance. AG also reviewed the papers selected for the meta-analysis and undertook a substantial part in the preparation of the revised manuscript.
Funding This research received no specific grant from any agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available.