Accuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: systematic review
BMJ 2007; 335 doi: https://doi.org/10.1136/bmj.39276.636354.AE (Published 04 October 2007) Cite this as: BMJ 2007;335:711
- Daniel Pewsner, senior research fellow in general practice; and general practitioner1,
- Peter Jüni, reader in clinical epidemiology2,
- Matthias Egger, professor3,
- Markus Battaglia, senior research fellow in general practice; and general practitioner1,
- Johan Sundström, associate professor4,
- Lucas M Bachmann, reader in clinical epidemiology and deputy director5
- 1Institute of Social and Preventive Medicine (ISPM), University of Bern, Finkenhubelweg 11, CH-3012 Berne, Switzerland; and Medix General Practice Network, Bern, Switzerland
- 2Institute of Social and Preventive Medicine (ISPM), University of Bern
- 3Institute of Social and Preventive Medicine (ISPM), University of Bern; and Department of Social Medicine, University of Bristol, Bristol
- 4Department of Medical Sciences, Uppsala University Hospital, Uppsala, Sweden
- 5Horten Centre, University of Zurich, Zurich, Switzerland
- Correspondence to: M Egger egger{at}ispm.unibe.ch
- Accepted 11 July 2007
Abstract
Objective To review the accuracy of electrocardiography in screening for left ventricular hypertrophy in patients with hypertension.
Design Systematic review of studies of test accuracy of six electrocardiographic indexes: the Sokolow-Lyon index, Cornell voltage index, Cornell product index, Gubner index, and Romhilt-Estes scores with thresholds for a positive test of ≥4 points or ≥5 points.
Data sources Electronic databases ((Pre-)Medline, Embase), reference lists of relevant studies and previous reviews, and experts.
Study selection Two reviewers scrutinised abstracts and examined potentially eligible studies. Studies comparing the electrocardiographic index with echocardiography in hypertensive patients and reporting sufficient data were included.
Data extraction Data on study populations, echocardiographic criteria, and methodological quality of studies were extracted.
Data synthesis Negative likelihood ratios, which indicate to what extent the posterior odds of left ventricular hypertrophy is reduced by a negative test, were calculated.
Results 21 studies and data on 5608 patients were analysed. The median prevalence of left ventricular hypertrophy was 33% (interquartile range 23-41%) in primary care settings (10 studies) and 65% (37-81%) in secondary care settings (11 studies). The median negative likelihood ratio was similar across electrocardiographic indexes, ranging from 0.85 (range 0.34-1.03) for the Romhilt-Estes score (with threshold ≥4 points) to 0.91 (0.70-1.01) for the Gubner index. Using the Romhilt-Estes score in primary care, a negative electrocardiogram result would reduce the typical pre-test probability from 33% to 31%. In secondary care the typical pre-test probability of 65% would be reduced to 63%.
Conclusion Electrocardiographic criteria should not be used to rule out left ventricular hypertrophy in patients with hypertension.
Introduction
Arterial hypertension is a major cause of coronary heart disease, stroke, and heart failure. Several studies have shown that left ventricular hypertrophy is an important risk factor in patients with hypertension, leading to a fivefold to 10-fold increase in cardiovascular risk,1 2 3 4 5 which is similar to the increase seen in patients with a history of myocardial infarction.6 The presence of left ventricular hypertrophy, in addition to hypertension, thus has important implications for assessing risk and managing patients, including decisions on interventions other than antihypertensive treatment, such as lipid lowering treatment and lifestyle modifications.7 8 Accurate and early diagnosis of left ventricular hypertrophy is therefore an important component of the care of patients with hypertension.
Decisions about treatment should be based on assessments of hypertensive target organ damage and overall cardiovascular risk. The appropriate diagnostic work-up of suspected left ventricular hypertrophy in patients with hypertension is less clear, however. More than 30 different electrocardiographic indexes for the diagnosis of left ventricular hypertrophy, based on the standard 12 lead electrocardiogram, have been described. Many of the proposed indexes have remained anecdotal, but others are commonly used, including the Sokolow-Lyon index,9 the Cornell voltage index,10 the Cornell product index,11 the Gubner index,12 and the Romhilt-Estes scores.13 However, debate about their comparative diagnostic value continues.14 15 16 We did a systematic review to clarify the accuracy of different electrocardiographic indexes, with emphasis on their ability to rule out left ventricular hypertrophy in patients with arterial hypertension.
Methods
Identification of studies
We searched Medline and (Pre-)Medline (PubMed version) from 1966 to present (last update December 2005) and Embase (Ovid version) from 1980 to present (last update December 2005) to identify observational studies that evaluated the accuracy of electrocardiographic indexes for the diagnosis of left ventricular hypertrophy and established the presence or absence of left ventricular hypertrophy with echocardiography. We restricted our search to papers published in English, German, Italian, Spanish, French, and Portuguese. The search strategies are available on request. Checks of the reference lists of relevant studies and contacts with experts in the field complemented the electronic searches.
Study selection
We included studies in asymptomatic patients with primary arterial hypertension in any type of healthcare setting. Studies included patients on antihypertensive treatment, patients with newly diagnosed hypertension being evaluated for treatment, and patients in whom treatment was withdrawn shortly before evaluation. We selected the studies in a two stage process. Two reviewers (DP and MB) independently assessed the abstracts of all retrieved studies. We ordered all papers considered to be potentially relevant by one reviewer and made the final decision by using a checklist to assess whether the criteria for inclusion had been met. We included all studies that assessed the electrocardiographic criteria in hypertensive adults against echocardiography (left ventricular mass indexed for body surface area) for whom sufficient data to allow the construction of the two by two table was available. We excluded studies that compared patients with known left ventricular hypertrophy with healthy controls (diagnostic case-control studies).17 18 We also excluded studies that used a reference standard calibrated according to heart mass/body height and studies that evaluated patients with concomitant left anterior fascicular block and left bundle branch block.
Data extraction
We extracted data in duplicate, including the number and characteristics of patients (mean age, distribution of sex and ethnic groups, mean body mass index, and smoking status), the healthcare setting (primary care versus secondary care), the prevalence of echocardiographically confirmed left ventricular hypertrophy, the electrocardiographic indexes evaluated, and the definition of the echocardiography threshold. We constructed two by two contingency tables for all electrocardiographic criteria reported in included articles. The data extraction form had been piloted for other diagnostic reviews and is described in detail elsewhere.19 We contacted first authors of eligible studies that reported insufficient data and asked them for additional information.
Assessment of study quality
We assessed the methodological quality of papers that met the eligibility criteria. We examined the methods of patient selection and data collection, completeness of descriptions of index and reference tests, completeness of blinding, and the likelihood of verification bias.17 18 20 We ranked studies as high quality if they described the setting (for example, family physicians referring patients to the clinic); collected data prospectively, with enrolment of consecutive patients and follow-up of all patients, including those who did not have echocardiography; and provided details on echocardiography and whether the assessor of the echocardiography was unaware of the electrocardiogram result or vice versa (blinding). We ranked studies as intermediate quality if they met four or five of the six criteria, as low quality if they met only one to three of the six criteria, and as very low quality if they met none of the criteria.
Statistical analysis
We added 0.5 to each cell of all two by two tables that included one or more zero cells. We calculated sensitivities, specificities, and likelihood ratios with their confidence intervals. As the electrocardiogram will mainly be used to rule out the diagnosis of left ventricular hypertrophy, we were particularly interested in the sensitivity and the likelihood ratio of a negative electrocardiogram result. The likelihood ratio of a negative test indicates how likely it is to find a negative result among people with left ventricular hypertrophy compared with those without.21 The negative likelihood ratio is calculated as (1−sensitivity)/specificity. It indicates to what extent the posterior odds of left ventricular hypertrophy would be reduced if the test was negative. If the prior odds is 1 and the negative likelihood ratio is 0.5, the posterior odds will be 1×0.5=0.5. The likelihood ratio of a positive test indicates how likely it is that a positive result will be found among people with left ventricular hypertrophy compared with those without; it is defined as sensitivity/(1−specificity).21 We summarised results by plotting sensitivities and specificities in the receiver operating curve space and by calculating medians, ranges, and interquartile ranges.
Results
Literature search
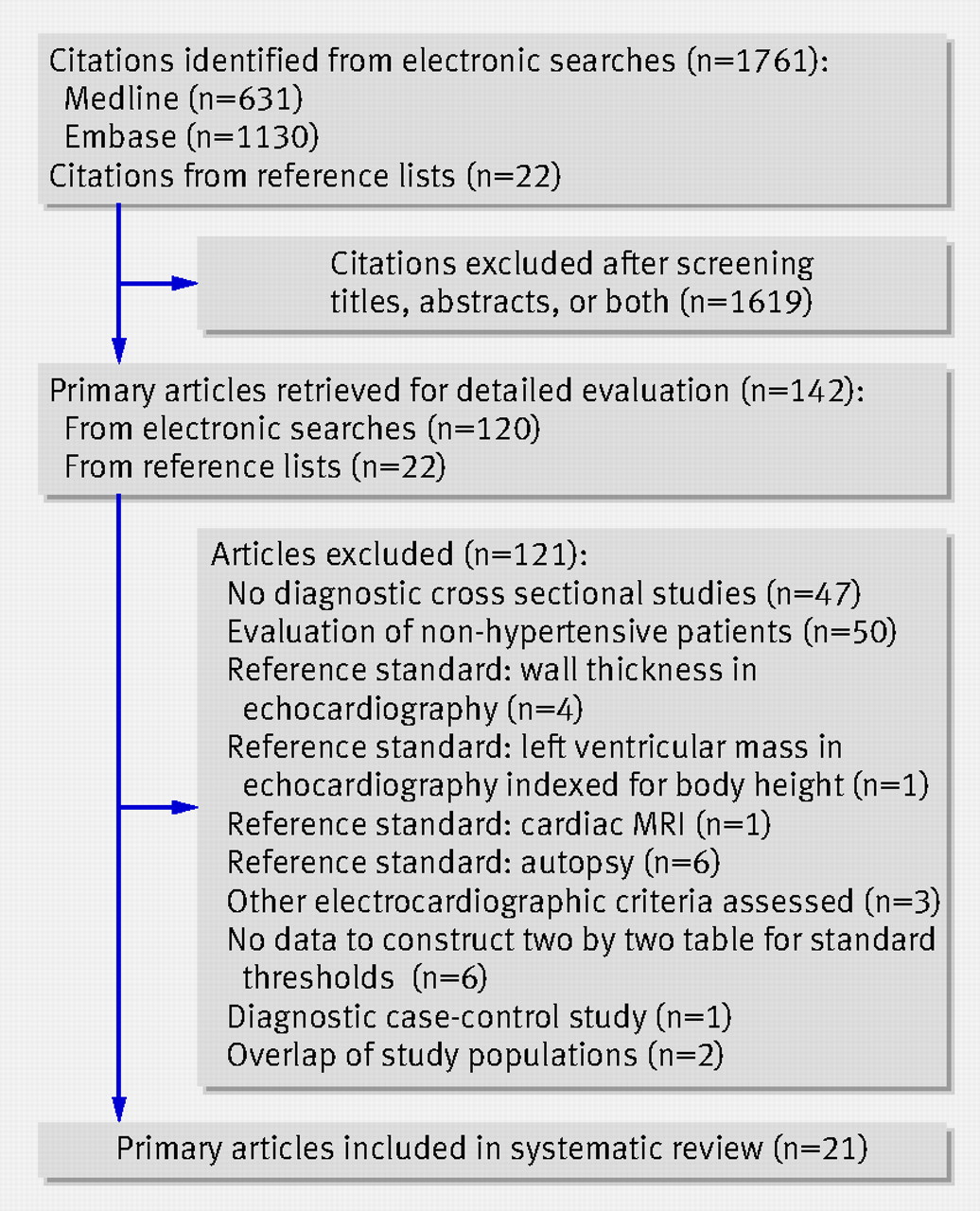
Our search identified 1761 citations. After exclusion of duplicates and examination of the abstracts we considered 142 as potentially eligible, and after scrutinising the full text articles we included 21 studies.w1-w21 Figure 1⇓ summarises the process of assessing and selecting the studies. First authors provided additional information on nine studies.w1w6w10w12w16-w19w21

Fig 1 Flow chart of study selection process. MRI=magnetic resonance imaging
{kind=link}
Study characteristics
The 21 studies included a total of 5608 (range 30-947) patients. Table 1⇓ details the characteristics and methodological quality of the studies. Ten studies were done in primary care and 11 in secondary care. Three studies included only men; all others examined men and women. The median prevalence of left ventricular hypertrophy was 33% (interquartile range 23-41%) in primary care settings and 65% (37-81%) in secondary care. Three studies met all six methodological criteria and were ranked as high quality. Another 11 studies met four or five criteria and were ranked as intermediate quality, whereas seven studies met two or three quality items and were considered of low quality. Table 1⇓ lists the criteria met by different studies.
Characteristics of studies of test accuracy of six commonly used electrocardiographic criteria for diagnosis of left ventricular hypertrophy
Electrocardiographic indexes
The 21 articles reported on 12 different electrocardiographic criteria. We analysed in detail the six most commonly used indexes, including the Sokolow-Lyon voltage index,9 the Cornell voltage and Cornell product indexes,10 11 the Gubner index,12 and the Romhilt-Estes score with two different thresholds.13 The box shows definitions of these indexes.
Definitions of six electrocardiographic indexes commonly used in diagnosis of left ventricular hypertrophy
Sokolow-Lyon index9—sum of SV1+RV5 or V6>3.5 mV
Cornell voltage index22—men: RaVL+SV3>2.8 mV; women: RaVL+SV3>2.0 mV
Cornell product23—men: (SV3+RaVL)×QRS duration ≥2440 ms; women: (SV3+(RaVL+8 mV))×QRS duration>2440 ms
Gubner12—RI+SIII≥25 mV
Romhilt-Estes scores13—excessive amplitude: 3 points (largest R or S wave in limb leads ≥20 mV or S wave in V1 or V2 ≥30 mV or R wave in V5 or V6 ≥30 mV). ST-T segment pattern of LV strain: 3 points (ST-T segment vector shifted in direction opposite to mean QRS vector). Left atrial involvement: 3 points (terminal negativity of P wave in V1≥1 mm with duration ≥0.04 s). Left axis deviation: 2 points (left axis ≥−30° in frontal plain). Prolonged QRS duration: 1 point (≥0.09 s). Intrinsicoid deflection: 1 point (intrinsicoid deflection in V5 or V6≥0.05 s). Two thresholds in use: positive if ≥4 points or ≥5 points
Sensitivity, specificity, and likelihood ratios
Figure 2⇓ shows the accuracy data for the six electrocardiographic indexes plotted in the receiver operating curve space. For all indexes, most studies are located in the bottom left corner of low sensitivity and high specificity. Table 2⇓ shows, for each of the 21 studies, the number of true positives, false positives, false negatives, and true negatives, along with the corresponding sensitivities and specificities. The median sensitivity ranged from 10.5% (range 0-39%) for the Gubner index to 21% (4-52%) for the Sokolow-Lyon index. Median specificity ranged from 89% (53-100%) for the Sokolow-Lyon index to 99% (71-100%) for the Romhilt-Estes (five points) score.

Fig 2 Receiver operating curves of six commonly used electrocardiographic indexes for diagnosis of left ventricular hypertrophy. Each point represents one study
{kind=link}
Results from test accuracy studies of electrocardiographic indexes in diagnosis of left ventricular hypertrophy: raw data from two by two tables, sensitivity, and specificity
Figures 3⇓ and 4⇓ show forest plots of the negative and positive likelihood ratios. The median negative likelihood ratio was similar across electrocardiographic indexes, ranging from 0.85 (range 0.34-1.03) for the Romhilt-Estes score (four points) to 0.91 (0.70-1.01) for the Gubner index. More variation existed in the positive likelihood ratio, which ranged from 1.90 (0.16-25.9) for the Sokolow-Lyon index to 5.90 (0.71-18.2) for the Romhilt-Estes score (four points). Using the median likelihood ratios from the Romhilt-Estes score (four points) in primary care, a negative electrocardiogram result would reduce the typical pre-test probability of 33% to 31%, whereas a positive electrocardiogram would increase it to 74%. In secondary care, the typical pre-test probability of 65% would be reduced to 63% or increased to 92%.

Fig 3 Forest plots of negative likelihood ratio from test accuracy studies of six electrocardiographic indexes in diagnosis of left ventricular hypertrophy. Points represent estimates of likelihood ratio; lines represent 95% confidence intervals
{kind=link}

Fig 4 Forest plots of positive likelihood ratio from test accuracy studies of six electrocardiographic indexes in diagnosis of left ventricular hypertrophy. Points represent estimates of likelihood ratio; lines represent 95% confidence intervals
{kind=link}
Discussion
This systematic review of studies of the accuracy of diagnostic tests found that the accuracy of electrocardiographic indexes in the diagnosis of left ventricular hypertrophy is unsatisfactory. In particular, none of the more recent and more sophisticated indexes is clearly superior to the Sokolow-Lyon index, which was developed in 1949.9 Irrespective of the index used, the electrocardiogram is a poor screening tool to exclude left ventricular hypertrophy in hypertensive patients in primary and secondary care settings. Of note, specificity was reasonably high in most studies, but because sensitivity was low the power to rule in left ventricular hypertrophy was also unsatisfactory, and the electrocardiogram cannot be considered a “SpPIn” (specific, positive, in) test for the diagnosis of left ventricular hypertrophy.21
Strengths and limitations
We did a comprehensive literature search, selected studies according to pre-defined criteria, and appraised the methodological quality of studies. We acknowledge that we may have missed some studies, but their inclusion is unlikely to have changed our conclusions: empirical research suggests that unpublished studies of test accuracy are small and show lower diagnostic accuracy.24 We excluded diagnostic case-control studies, which are known to overestimate accuracy,17 18 as well as studies that did not index ventricular mass for body surface area. We also excluded studies that evaluated patients with concomitant left anterior fascicular block and left bundle branch block, because these patients usually need further examinations and referral irrespective of left ventricular hypertrophy. We summarised the evidence by calculating medians, rather than combining data in meta-analysis. We believe that a formal meta-analysis would have added little in this situation. Similarly, we thought that further exploration of potential sources of heterogeneity was not warranted. The published data did not allow direct comparisons of test accuracy between the different indexes. More importantly, we did not identify any randomised comparisons of diagnostic and treatment strategies and assessed clinical end points.
Implications for clinical practice
Although many hypertensive patients have electrocardiographic testing for other reasons, electrocardiograms should not be done specifically to exclude left ventricular hypertrophy in patients with hypertension. A comprehensive assessment of cardiovascular risk is important to guide decisions on therapeutic interventions in these patients, and referral for echocardiography may be justified in some patients. Referral for specialist examinations and care is often based on high cardiovascular risk scores, but echocardiography may be more informative in hypertensive patients who, on the basis of age, sex, smoking history, and blood lipids, are at low or intermediate risk. In patients known to be at high risk, echocardiographic findings will often not affect clinical management, because interventions to reduce risk, such as example lipid lowering treatment, smoking cessation, and dietary modification, are already in place.
Recommendations from current guidelines differ. The 2003 European Society of Hypertension-European Society of Cardiology guidelines recommend echocardiography in patients in whom target organ damage is not discovered by routine electrocardiography.25 The 2004 guidelines from the British Hypertension Society state that echocardiography is not required routinely but is valuable to confirm or refute the presence of left ventricular hypertrophy when the electrocardiogram shows high left ventricular voltage without T wave abnormalities.26 In the United States, the seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends routine electrocardiography but makes no mention of echocardiography.27
The evidence on the capacity of various antihypertensive agents to decrease left ventricular hypertrophy is limited. Several studies have shown a possible advantage of angiotensin converting enzyme inhibitors and angiotensin II subtype 1 receptor antagonist based treatments in reducing left ventricular hypertrophy and preventing clinical events.28 However, as most patients need several antihypertensive agents for optimal blood pressure control, the relative merits of each agent may be of lesser importance. In addition to antihypertensive drugs, preventing cardiovascular disease through modifications of other risk factors such as smoking cessation, lifestyle change, or lipid lowering treatment is the most promising approach.29 30 Indeed, moderate reductions in several risk factors might be more effective than major reductions in one.31
Future research
Further research is needed to identify cost effective diagnostic strategies in primary care settings, including randomised controlled trials that compare different diagnostic and treatment strategies and assess clinical end points. Such research could inform the development of algorithms to identify patients who should be referred for echocardiography. In the absence of accurate and inexpensive screening tests for left ventricular hypertrophy, research into new diagnostic technologies is also warranted. Of note, electrocardiographic left ventricular hypertrophy and echocardiographic left ventricular hypertrophy have been shown to predict mortality independently of each other and may therefore assess different aspects of the underlying pathology.5 Alternatively, they may measure the same condition with some imprecision.32 For example, in echocardiography, distinguishing physiological from pathological left ventricular hypertrophy can sometimes be difficult.5 Further studies are needed to better define the pathophysiological mechanisms and outcomes in patients with echocardiographically confirmed left ventricular hypertrophy but negative electrocardiograms. Similarly, more data are needed on patients with positive electrocardiographic tests but negative echocardiography.
Conclusions
The power of some of the more commonly used electrocardiographic criteria to rule out the diagnosis of left ventricular hypertrophy in patients with hypertension is poor. Further research is needed to assess the cost effectiveness of different diagnostic and treatment strategies and to develop alternative diagnostic technologies for assessment of left ventricular hypertrophy in primary care.
What is already known on this topic
Left ventricular hypertrophy leads to a fivefold to 10-fold increase in cardiovascular risk in hypertensive patients
Several indexes calculated from standard 12 lead electrocardiograms are used in the diagnostic work-up of patients with hypertension
What this paper adds
The accuracy of the more commonly used electrocardiographic criteria for ruling out left ventricular hypertrophy is unsatisfactory in both primary and secondary care.
Echocardiography is needed for a comprehensive assessment of cardiovascular risk in hypertensive patients
Footnotes
We thank Marc Gertsch, Richard S Crow, Benedict Martina, Fritz Grossenbacher, and Heiner C Bucher for valuable input and for commenting on an earlier draft.
Contributors: DP, ME, PJ, and MB initiated the study and wrote the protocol. DP and MB did the searches, screened the literature, and extracted the data. LMB did the analysis, supervised the work, and wrote a first draft, which was subsequently revised by ME. All authors participated in interpreting the data and critically revising the manuscript for important intellectual content. ME is the guarantor.
Funding: Krankenfürsorgestiftung der Gesellschaft für das Gute und Gemeinnützige (GGG), Basel, Switzerland, Swiss National Science Foundation (grant 3233B0-103182 and 3200B0-103183).
Competing interests: None declared.
Ethical approval: Not needed.
Provenance and peer review: Non-commissioned; externally peer reviewed.