Article Text

Abstract
Background Orbital inflammatory disease (OID) encompasses a wide range of pathology including thyroid-associated orbitopathy (TAO), granulomatosis with polyangiitis (GPA), sarcoidosis and non-specific orbital inflammation (NSOI), accounting for up to 6% of orbital diseases. Understanding the underlying pathophysiology of OID can improve diagnosis and help target therapy.
Aims To test the hypothesis that shared signalling pathways are activated in different forms of OID.
Methods In this secondary analysis, pathway analysis was performed on the previously reported differentially expressed genes from orbital adipose tissue using patients with OID and healthy controls who were characterised by microarray. For the original publications, tissue specimens were collected from oculoplastic surgeons at 10 international centres representing four countries (USA, Canada, Australia and Saudi Arabia). Diagnoses were independently confirmed by two masked ocular pathologists (DJW, HEG). Gene expression profiling analysis was performed at the Oregon Health & Science University. Eighty-three participants were included: 25 with TAO, 6 with orbital GPA, 7 with orbital sarcoidosis, 25 with NSOI and 20 healthy controls.
Results Among the 83 subjects (mean (SD) age, 52.8 (18.3) years; 70% (n=58) female), those with OID demonstrated perturbation of the downstream gene expressions of the IGF-1R (MAPK/RAS/RAF/MEK/ERK and PI3K/Akt/mTOR pathways), peroxisome proliferator-activated receptor-γ (PPARγ), adipocytokine and AMPK signalling pathways compared with healthy controls. Specifically, GPA samples differed from controls in gene expression within the insulin-like growth factor-1 receptor (IGF-1R, PI3K-Akt (p=0.001), RAS (p=0.005)), PPARγ (p=0.002), adipocytokine (p=0.004) or AMPK (p=<0.001) pathways. TAO, sarcoidosis and NSOI samples were also found to have statistically significant differential gene expression in these pathways.
Conclusions Although OID includes a heterogenous group of pathologies, TAO, GPA, sarcoidosis and NSOI share enrichment of common gene signalling pathways, namely IGF-1R, PPARγ, adipocytokine and AMPK. Pathway analyses of gene expression suggest that other forms of orbital inflammation in addition to TAO may benefit from blockade of IGF-1R signalling pathways.
- inflammation
- orbit
- experimental – laboratory
Data availability statement
Data are available upon reasonable request. All the individual participant data that underlie the results reported in this article after deidentification will be shared and available upon request to investigators whose proposed use of the data has been approved by an independent review committee identified for this purpose for individual participant data meta-analysis. Proposal should be directed to rosenbaj@ohsu.edu. To gain access, data requestors will need to sign a data access agreement.
Statistics from Altmetric.com
Introduction
The pathogenesis of orbital inflammatory disease (OID) is uncertain. In the most well-studied OID, thyroid-associated orbitopathy (TAO), the orbital fibroblast appears to be a key effector cell and coexpresses insulin-like growth factor-1 receptor (IGF-1R) and thyroid-stimulating hormone receptor (TSHR).1 2 IGF-1R is a tyrosine kinase receptor and TSHR is a G protein-coupled receptor. Both are upregulated in TAO orbital fibroblasts especially in active disease.3 4 There is evidence that these two cell surface receptors are closely associated and can synergistically regulate overlapping downstream signalling pathways.3 5
Activation of these receptors results in a signalling cascade including the MAPK/Ras/Raf/MEK/ERK and PI3K/Akt/mTOR pathways leading to increased hyaluronic acid synthesis, adipogenesis and production of inflammatory cytokines culminating in clinical TAO.2–7 A fully human monoclonal IGF-1R antagonist antibody, teprotumumab, has recently been approved by the US Food and Drug Administration (FDA) for the treatment of patients with TAO.8 9
In addition to the IGF-1R pathway, de novo adipogenesis is often enhanced in TAO via the peroxisome proliferator-activated receptor-γ (PPARγ) pathway.1–3 PPARγ, a nuclear transcription factor, is a potent stimulator for adipogenesis in TAO through increasing proliferation of orbital fibroblasts and facilitating their differentiation into adipocytes.2 3 PPARγ expression is significantly increased in orbital tissue of patients with active TAO.1 4
Messenger RNA (mRNA) signatures (gene expression profiling) have been previously shown to differentiate TAO from other forms of orbital inflammation.10–14 For example, using molecular profiling, a subset of patients initially thought to have non-specific orbital inflammation (NSOI) was suggested to actually manifest a limited form of granulomatosis with polyangiitis (GPA).11 12 Despite previous studies demonstrating unique gene expression signatures among different OID, the shared gene expression pathways have not yet been characterised. To this end, we aimed to identify enriched gene expression pathways in various forms of OID via microarray analyses and evaluated for shared pathways among TAO, GPA, sarcoidosis and NSOI. This information may assist in the expansion of known therapies and the creation of novel therapeutic targets used to treat orbital inflammation.
Materials and methods
This study was approved by the Institutional Review Board (IRB) at Oregon Health & Science University (IRB00006301) and at each of the other contributing centres. Methods for the microarray analysis of transcripts from orbital adipose tissue biopsies have been described elsewhere.11 13 In brief, formalin-fixed, paraffin-embedded orbital adipose tissue biopsies were obtained from healthy controls (n=20) and patients with TAO (n=25), orbital GPA (n=6), orbital sarcoidosis (n=7) and NSOI (n=25) based on clinical and histopathological information provided by the respective oculoplastic surgeons and ocular pathologists in the Orbital Inflammatory Disease Consortium. Samples were obtained from North America (Oregon, California, Ohio, Wisconsin, North Carolina, New York, Florida and British Columbia), Australia and Saudi Arabia. Histopathological diagnoses were determined independently by two ocular pathologists (DJW and HEG) masked to the clinical diagnosis. In all cases, the consensus diagnosis obtained by DJW and JTR based on the histopathology reports and the clinical data agreed with the contributing centre’s diagnosis. Tissue samples were collected and processed at two different time points, which were used as discovery and validation sets. There was only one sarcoidosis sample in the discovery set, which was excluded from reliability analysis due to the small number of sarcoidosis tissue samples available. Gene expression was quantified using GeneChip Human Genome U133 Plus 2.0 Array (Affymetrix, Santa Clara, California, USA) which can analyse the expression levels of over 38 000 human genes. The subjects within the TAO, GPA, NSOI groups were divided into a discovery and a validation test set to ascertain if the differentially expressed genes found in the former were reproducible in the latter. This is an important step to avoid bias in classifying relationships when the number of candidate predictors (eg, mRNA transcript types) is greater than the number of cases (eg, tissue samples) such as with microarray datasets. Threshold criteria was defined as probe sets containing at least 1.5-fold change (FC) in gene expression compared with healthy controls and a false discovery rate (FDR) adjusted p value <0.05 in both sets.11 13 15 16
Upstream signalling pathways associated with these differentially expressed transcripts were identified to assess whether these genes participated in the biological cascade of OID more than by chance. Both the Reactome programme (http://reactome.org) and the NIH Database for Annotation, Visualisation and Integrated Discovery (DAVID) programme querying the KEGG (Kyoto Encyclopedia of Genes and Genomes) database were used to identify pathways for functional enrichment.17–19 Since FDR, a multiple testing correction, was applied to the previously reported differentially expressed gene lists and the test statistics of pathway enrichment based on the lists were not independent, we report marginal p values in this paper.
Results
Among the 83 subjects, the mean (SD) age was 52.8 (18.3) years, and 58 (70%) subjects were female (table 1). Orbital adipose tissue biopsies were obtained from patients with OID including 25 with TAO, 6 with orbital GPA, 7 with orbital sarcoidosis and 25 with NSOI, each of which were compared with tissues from 20 healthy controls who underwent blepharoplasty or enucleation with non-inflamed orbits. All groups comprised of samples from a majority of female subjects: 76% of TAO, 67% of GPA, 71% of sarcoidosis, 64% of NSOI and 70% of healthy controls were female, and there was no statistically significant difference in female ratios across the groups (χ²=0.893, p=0.944).
Age and sex for each experimental group
Of the 25 subjects with TAO, the median time from ocular symptoms onset to biopsy was 40 months (range 1–432 months, figure 1). One subject was biopsied at 1 month of TAO onset with eight biopsied between 1 and 2 years, none in year 3, five at year 4 and five at >5 years from disease onset. Nineteen (76%) had a history of hyperthyroidism, one (4%) had hypothyroidism, three (12%) were euthyroid and two (8%) did not have thyroid status. One hundred per cent of those who reported a reason for surgery (n=20) stated their reason as ‘symptomatic relief’. The median time from onset of ocular symptoms to biopsy in GPA was 5 months (range 1–10 months) with sarcoidosis at 8 months (range 2–19) and NSOI at 9 months (range 0.3–444 months, figure 1).

Time in months from ocular symptom onset to biopsy in the OID groups. Asterisks indicate outlying data points: 5 samples in TAO: 85, 96, 102, 120, 432 months; four samples in NSOI: 60, 72, 96, 444. All pairwise differences of median time of biopsy were statistically significant by the Mann-Whitney U test except between GPA and sarcoidosis. GPA, granulomatosis with polyangiitis; NSOI, non-specific orbital inflammation; TAO, thyroid-associated orbitopathy.
Differentially expressed genes (>1.5 FC and FDR p<0.05) were previously reported between each of four OID groups relative to healthy controls.11 13 To explore the biological functions of these genes, functional annotation and pathway analyses using the KEGG database in DAVID and the Reactome databases were performed (figure 2, online supplemental figures 1–4, table 2). Orbital fat from controls came from either the anterior orbit or the retrobulbar region. Gene expression in adipose tissue might differ based on tissue location. Accordingly, we tested the hypothesis that our results were affected or skewed by combining results for gene expression from two distinct locations. Healthy controls were segregated into blepharoplasty and enucleation groups and gene expressions were analysed separately. There was overlap in the multidimensional scaling (MDS) plot between the anterior and retrobulbar orbital adipose tissue groups without distinct clusters (online supplemental figure 5). This was confirmed by pairwise comparisons which demonstrated no significantly different genes between these groups using FDR <0.05. In all four OID groups, however, there was a greater number of differentially expressed gene transcripts associated with IGF-1R, PPARγ, adipocytokine and adenosine monophosphate-activated protein kinase (AMPK) signalling pathways when compared with healthy controls (p<0.05 in all pathways, table 2). These were among the top signalling pathways enriched in each individual OID group.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Gene signalling pathway in each experimental group

{kind=link}
{kind=link}
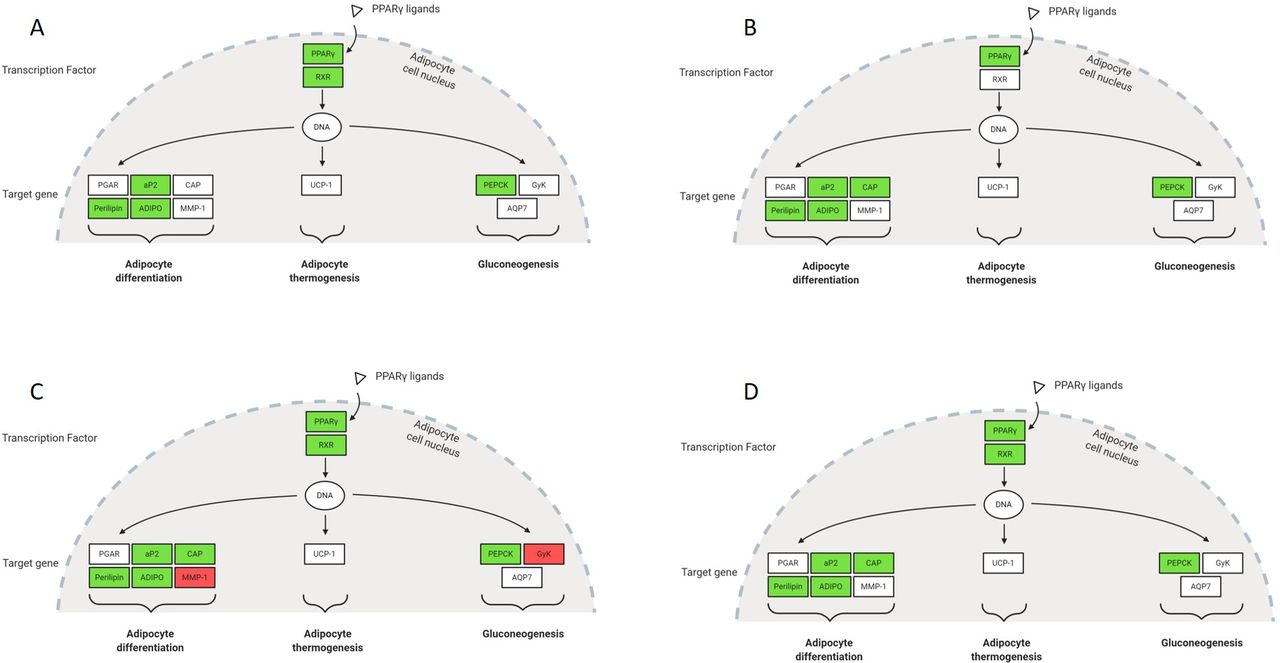
Differential gene expression in the PPARγ receptor signalling pathways. (A) TAO. (B) GPA. (C) Sarcoidosis. (D) NSOI. Upregulation (red) or downregulation (green) illustrates increase or decrease of gene expression in the specific OID compared with controls. The pathway diagrams with differential gene expression were created with BioRender.com. https://david.ncifcrf.gov/kegg.jsp?path=hsa03320$PPAR_signaling_pathway&termId=550028694&source=kegg. OID, orbital inflammatory disease.
The differentially expressed gene transcripts identified within the IGF-1R pathway were associated with cellular functions such as cell survival (ie, FasL), cell growth, apoptosis (ie, Nore1, Mst1), protein synthesis, cytoskeletal remodelling/organisation (ie, ABL), cell motility (ie, PAK) and endocytosis (RAB5, online supplemental figures 1 and 2). In contrast, the differentially expressed transcripts identified within the PPARγ signalling pathway were involved in adipocyte differentiation (ie, Perilipin, ADIPO, aP2) and gluconeogenesis (ie, PEPCK, figure 2). Within the adipocytokine signalling pathway, there was differential expression of cytokine tumour-necrosis factor (TNF) and the adipocytokines leptin and adiponectin known to be associated with growth and reproduction, energy metabolism, and insulin resistance (online supplemental figure 3). Within the AMPK signalling pathway—which intersects the IGF-1R, PPARγ and adipocytokine pathways—differentially expressed proteins were those involved in fatty acid biosynthesis (FAS), mitochondrial biogenesis (FOXO), protein synthesis (eEF2K) and gluconeogenesis (G6Pase, online supplemental figure 4).
Overall, while shared signalling pathways were found to be perturbed in all four forms of OID, their specific gene signatures differed (figure 2, online supplemental figures 1–4).
Discussion
Gene expression patterns have the potential to assist with diagnosis, clarify pathogenesis and tailor choice of therapy. Understanding the molecular pathogenesis of orbital inflammation and regulation of the immune system can lead to the development of tailored biotherapeutics. Our prior studies demonstrate that these biological signatures can be harnessed to differentiate forms of orbital inflammation.10–14 Looking closer at the mRNA expression in orbital biopsies, we now identify potential shared pathways that are involved in various types of OID. All four OID groups demonstrated perturbation of the IGF-1R, PPARγ, adipocytokine and AMPK signalling pathways. Although they mostly exhibited downregulation of these pathways (illustrated in green in figure 2, online supplemental figures 1–4), the interactive nature of a pathway such as reduced gene expression of one gene in an effort to mitigate increased expression of another gene means that downregulation implicates a pathway just as upregulation does.20 21 Thus, it is more appropriate to conclude that there is a functional relationship between these differentially expressed genes. Targeting these pathways in OID may translate into viable therapeutic options.
Earlier this year, teprotumumab, an IGF-1R antagonist, gained FDA approval to treat TAO. This drug has been shown to decrease clinical signs of TAO including proptosis and increase quality of life.8 9 Further studies will determine if drug response can be predicted using gene expression and how treatment would in turn impact gene expression. Assessing biochemical markers may help to optimise the dosage and timing of therapy for OID. This personalised approach to medicine could minimise adverse effects, maximise response rate and may prove to be more cost-effective. Pathway analyses of transcriptomics suggest that forms of orbital inflammation in addition to TAO may be associated with the alteration of signalling pathways downstream of the IGF-1R and may also benefit from blockade of the IGF-1R.
IGF-1R inhibitors were originally investigated over the past four decades for the treatment of cancer.22–29 The only other FDA approved IGF-1R inhibitor is ceritinib (Zykadia, Novartis Pharmaceuticals Corporation), indicated for the treatment of anaplastic lymphoma kinase-positive metastatic non-small cell lung cancer. While teprotumumab demonstrated robust clinical response in therapeutic trials for TAO, the response was neither universal nor uniform. A potential explanation is that compensatory signalling pathways may overcome or bypass the IGF-1R blockade. For instance, crosstalk among the IGF-1R, PPARγ, adipocytokine and AMPK biological signalling pathways may be contributory to disease pathogenesis.30–33 Our findings suggest that there is a network of activated pathways in OID and that multifocal signal modulation therapy may decrease bypass mechanisms of resistance and amplify the effects of a single inhibitor.
Adipose tissue, in contrast to a variety of other tissues, expresses the highest levels of PPARγ, and its activation induces adipogenesis.34 Though not clinically proven, case reports provide examples of exacerbation of proptosis and reactivation of orbital disease in patients with euthyroid TAO taking PPARγ agonists prescribed to manage their type 2 diabetes.35 36 In orbital preadipocytes obtained from patients with TAO, PPARγ agonists have been shown to increase adipogenesis by 2 to 13-fold, whereas PPARγ antagonists reduce adipogenesis by two to sevenfold compared with untreated preadipocytes from patients with TAO.35 The reduction in adipogenesis is not seen in terminally differentiated adipocytes, suggesting that this effect and its potential therapeutic benefit may only exist in the active phase of TAO.37 Our study is also the first to suggest that in addition to TAO, GPA, sarcoidosis and NSOI share enrichment of the PPARγ signalling pathway. Multiple investigational PPARγ antagonists are in the preclinical stages of development. A high-throughput screen of FDA approved drugs discovered that imatinib (Gleevec, Novartis Pharma AG), an anticancer medication, acts as a PPARγ antagonist.38 Further studies in patients with TAO and other OID would be needed to demonstrate the therapeutic efficacy and safety of PPARγ antagonists.
The pathologic activation of PPARγ in GPA, sarcoidosis and NSOI suggests that adipocytes may be involved in their pathogenesis as previously demonstrated in TAO. Additionally, our study identified the activation of the adipocytokine signalling pathway in all OID groups. Orbital fat is predominantly white adipose tissue (WAT) composed of adipocytes, adipose stem cells, fibroblasts, macrophages, leucocytes and endothelial cells.39 Beyond its function in energy storage, WAT is demonstrating functionality as a major endocrine and immunologic organ. Adipocytes can produce adipocytokines such as leptin and resistin which have been linked to the production of inflammatory cytokines: TNF, interleukin-6 (IL-6) and IL-12.40 41 Activation of the adipocytokine pathway also activates AMPK which increases cellular energy production which may facilitate inflammation.42 Tocilizumab, a humanised anti-IL-6 receptor antibody, has been demonstrated to improve inflammation in active TAO.43 The use of anti-TNF agents has also been associated with subjective improvement in active TAO in case reports and small case series.44–46 These biologics, however, are likely targeting redundant genes or pathways and therefore have not been shown to modify the disease course.
It is also important to note that the TAO samples were obtained mainly from patients undergoing decompression more than 3 years after the onset of orbital symptoms and when clinically stable. The teprotumumab clinical trials limited enrolment to within 9 months after the onset of TAO based on the hypothesis that IGF-1R upregulation would be most amenable to therapeutic modification during this interval. However, our data suggest that IGF-1R and PPARγ upregulation persists during the presumed clinically stable, noninflammatory phase. This activation provokes consideration of its clinical significance and warrants further study to determine if the therapeutic window for TAO can be expanded to include late stage orbitopathy with an appropriate inhibitor.47
We acknowledge that artefacts can result from multiple statistical comparisons using a relatively small number of cases. To offset potential artefacts, two separate datasets for each form of OID were utilised to confirm truly differentially expressed genes. This was not possible in one OID form (sarcoidosis) given its rarity in our orbital disease samples. Second, this was a multinational study; although environment can affect gene expression, the commonality of the signalling pathways in the different forms of orbital inflammation studied strengthens the conclusion that they share pathogenetic pathways.
Conclusions
In conclusion, some of the pathways we have investigated are known, IGF-1R, or suspected, PPARγ, to be altered in TAO. However, we have demonstrated that these pathways are also enriched in GPA, sarcoidosis and NSOI. Moreover, additional enriched signalling pathways including adipocytokine and AMPK were identified in all four OID groups. OID is a heterogeneous group of disorders, and a clinical need exists for less-invasive biomarkers that can identify central signalling pathway activation to aid in diagnosis, prognosis, therapeutic selection and response monitoring of OIDs. We hope our findings will generate hypotheses for future trials to understand and modulate the biological mechanisms and clinical sequelae in OID.
Data availability statement
Data are available upon reasonable request. All the individual participant data that underlie the results reported in this article after deidentification will be shared and available upon request to investigators whose proposed use of the data has been approved by an independent review committee identified for this purpose for individual participant data meta-analysis. Proposal should be directed to rosenbaj@ohsu.edu. To gain access, data requestors will need to sign a data access agreement.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the IRB of Oregon Health & Science University, Study 00006301 and at each of the other contributing centres: Emory University IRB, University of California San Diego IRB, Mount Carmel (Ohio) IRB, Columbia University IRB, Medical College of Wisconsin IRB, King Khaled Eye Specialist Hospital Human Ethics Committee/Institutional Review Board, University of Miami IRB, Wake Forest University IRB, University of British Columbia Clinical Research Ethics Board, and Royal Adelaide Hospital Research Ethics Committee.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RV, SRP, CAH and JTR helped in the study concept and design. Analysis and interpretation of data were done by RV, DC, AJC, SRP, CAH, DJW and JTR. Acquisition of data was done by RV, DJW, HEG, CAH, RAD, JN, EAS, SRP, BSK, DK, CNC, JAF, MK, GJH, DPE, HA-H, AMYM, CA, AG and JTR. Drafting of the manuscript was done by RV, DC, AJC and JTR.
Funding This research was supported by funding from National Institutes of Health (NIH) USA Grants EY020249 (JTR) and an NIH/NEI Core Grant P30 EY010572. JTR receives support from the Grandmaison Fund for Autoimmunity Research, the William and Mary Bauman Foundation, the Stan and Madelle Rosenfeld Family Trust and Research to Prevent Blindness (no award number from these sources). The sponsors did not have any role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the manuscript for publication.
Competing interests JTR has in the past consulted for Genentech/Roche and was a coinvestigator on a study funded by Genentech to evaluate the use of rituximab for orbital inflammatory diseases. JTR, RAD, BSK, DOK, and GJH are consultants to Horizon Pharmaceuticals which manufactures teprotumumab. JTR receives research support from Horizon Pharmaceuticals.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- At a glance