Article Text

Statistics from Altmetric.com
Description
Ventricular septal aneurysm is a congenital defect found frequently in association with ventricular septal defects. Its detection has been increasing particularly in the era of non-invasive imaging. The clinical relevance of an incidentally detected aneurysm of the membranous ventricular septum (AMVS) in adults is unclear. Although most patients with AMVS are asymptomatic, various complications including cerebral embolism, cardiac arrhythmias, right ventricular outflow tract obstruction, bacterial endocarditis and rupture causing shunting may occur.1 It has been previously reported that cardiac CT may be one of the best imaging modalities available in identifying these aneurysms.2 Additionally, multi-slice CT has the advantage of three-dimensional morphological display.3
We describe herein for the first time, a patient who had a transcatheter aortic valve replacement with a pre-existing ventricular septal aneurysm. She is a 72-year-old female patient with a history of rheumatic heart disease, status post-previous 25-mm St Jude’s mitral valve replacement in 1988 for rheumatic mitral stenosis, who was referred to the multidisciplinary valve clinic for consideration for a transcatheter aortic valve replacement (TAVR) for severe aortic stenosis (AS). She had been having progressively increasing shortness of breath over the previous 6 months most consistent with New York Heart Association class III.
We were fortunate in having multiple diagnostic modalities available to evaluate this patient prior to her procedure. An echocardiogram showed severe AS with a mean gradient of 38 mm Hg and a peak velocity of 4.13 m/s. Cardiac CT was able to most clearly delineate the anatomy and location of the aneurysm. We could not perform a cardiac MRI on this patient as she had a non-MRI compatible pacemaker.
A TAVR CT done in preparation for her valve clinic visit showed aortic annulus area of 383 mm2 and an aortic annulus mean diameter of 21.8 mm. It also showed an outpouching of the membranous septum at the left ventricular outflow tract measuring 12.1x10 mm consistent with membranous ventricular septal aneurysm (figure 1). A Transesophageal Echocardiogram done to confirm these findings again demonstrated a ventricular septal aneurysm that was approximately 6 mm below the aortic annulus.
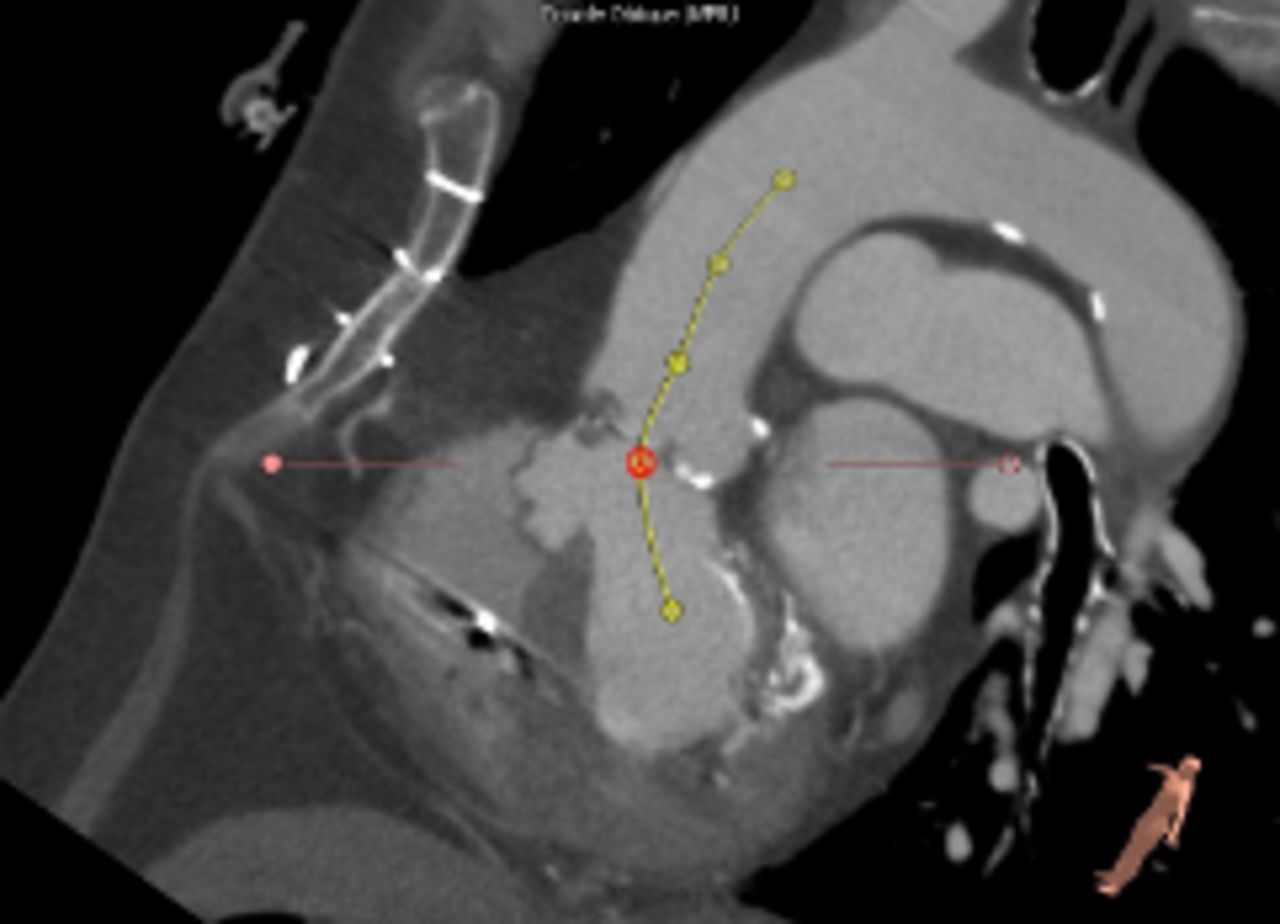
Baseline cardiac CT image in the long-axis view showing the membranous septal aneurysm and its relationship to the aortic annulus.
We had an internal discussion regarding the choice of valve (balloon-expanding vs self-expanding). We ultimately decided on an Edwards Sapien S3 valve as the team felt that this would ensure a controlled placement avoiding the aneurysm as much as possible. Our concern was ensuring the stability of the new valve and avoiding paravalvular leaks.
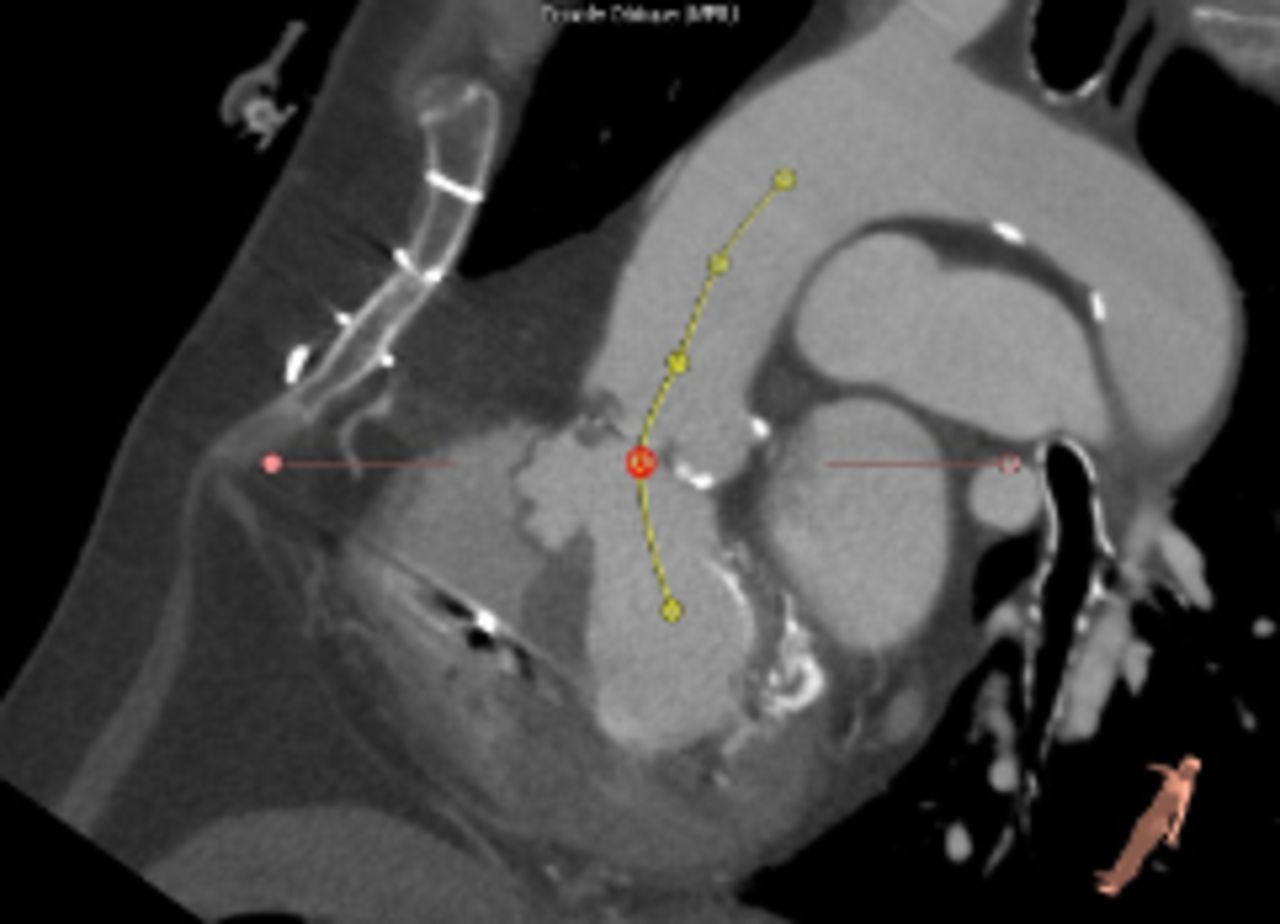
The patient subsequently underwent a successful TAVR using a 23-mm Edwards Sapien S3 valve with trivial paravalvular aortic insufficiency identified on intraoperative TEE. She had an uneventful postoperative course and was discharged home on postoperative day 6 once her International Normalized Ratio was therapeutic. An echocardiogram done 1-month post-TAVR demonstrated a mean gradient of 6 mm Hg and no evidence of paravalvular aortic insufficiency. A cardiac CT done 4 months post-TAVR demonstrated a well-seated valve that had been placed just above the aneurysm (figure 2).

{kind=link}
{kind=link}
Post-transcatheter aortic valve replacement (post-TAVR) cardiac CT image in the long-axis view showing the membranous septal aneurysm and its relationship to the implanted TAVR.
Patient’s perspective
I was extremely excited when I was told about a new procedure that was available to fix my valve. Under any circumstances, I did not want to be cut open again. When I was told about the aneurysm, I thought to myself, whatever will be will be. I did not care much about the aneurysm. I just did not want to go through open heart surgery again. I am happy to say I feel wonderful after the procedure.
Learning points
Ventricular septal aneurysm is a rare congenital defect found frequently in association with ventricular septal defects.
Transcatheter aortic valve replacement is an option for treating aortic stenosis in patients with a pre-existing ventricular septal aneurysm who are not otherwise candidates for surgery.
Footnotes
Contributors ZAH, JM and KA conducted the procedure, reviewed the manuscript and made corrections. AH interviewed the patient, created the manuscript and helped format the images and upload the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.