Article Text

Abstract
Thymoma-associated multiorgan autoimmunity is a relatively new term to describe the rare paraneoplastic syndrome that complicates thymoma, which can involve the thyroid, liver and intestine in addition to the skin. The pathology often indicates a graft-versus-host-like pattern commonly observed in recipients of an allogeneic haematopoietic cell transplant. We report a case of type B2 and B3 thymoma with invasion to the lung and pleura in a patient who presented with oral lichen planus and graft-versus-host-like erythroderma. The cutaneous lesions improved after complete resection of the thymoma in combination with systemic glucocorticoids, which was subsequently complicated by cytomegalovirus pneumonitis.
- cardiothoracic surgery
- dermatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Thymomas are the most common tumours arising from the anterior mediastinum. The association of thymoma with myasthenia gravis has long been recognised, and other paraneoplastic disorders are considerably rare.1 Herein, we report a case of thymoma with oral lichen planus and graft-versus-host-like erythroderma. The cutaneous lesions improved after complete resection of the thymoma with systemic glucocorticoids. Literatures on thymoma-related lichen planus and graft-versus-host-like erythroderma are also reviewed.
Case presentation
A 61-year-old man was admitted to the hospital because of masses in the mediastinum and right pleura with a massive pleural effusion in the right lung. Four years before this admission, he had received a diagnosis of oral lichen planus and autoimmune thyroiditis. Recurrent oral mucosal and lip erosions were refractory to oral prednisolone at a daily dose of 20 mg for 4 years and 100 mg of azathioprine for 3 months. One year later, erythematous, scaling and nonpruritic plaques over the lower limbs developed, which gradually extended to the trunk and upper limbs 4 months before this admission, without response to topical steroids. One month before this presentation, dysphagia, dry cough, dyspnea on exertion and hoarseness developed. The patient reported a weight loss of 8 kg and decreased appetite in the past 6 months. A chest radiograph revealed a mediastinal tumour with a pleural effusion (figure 1A), and a diagnosis of mediastinal tumour with pleural metastases was made. He was referred to the surgery department of our hospital.

(A) Chest radiography reveals a mediastinal tumour and multiple pleura-based masses with a pleural effusion of the right lung. (B) CT reveals a mediastinal tumour with invasion to the anterior chest wall and pleura-based masses with a pleural effusion.
Investigations
Physical examination revealed that the blood pressure was 126/71 mm Hg, the temperature 36.9°C, the pulse rate 84 beats/min and the respiration rate 18 breaths/min. Oxygen saturation was 95% while the patient was breathing ambient air. Confluent erosions were observed on the tongue surface. Erythematous patches on the face and numerous ill-defined and scaling plaques of various sizes were noted over the trunk and extremities involving more than 90% of the body surface area (figure 2). Bilateral leg erythema, swelling, discharge and tenderness on palpation were reported for 1 week.

Skin lesions of the trunk 7 days after the operation.
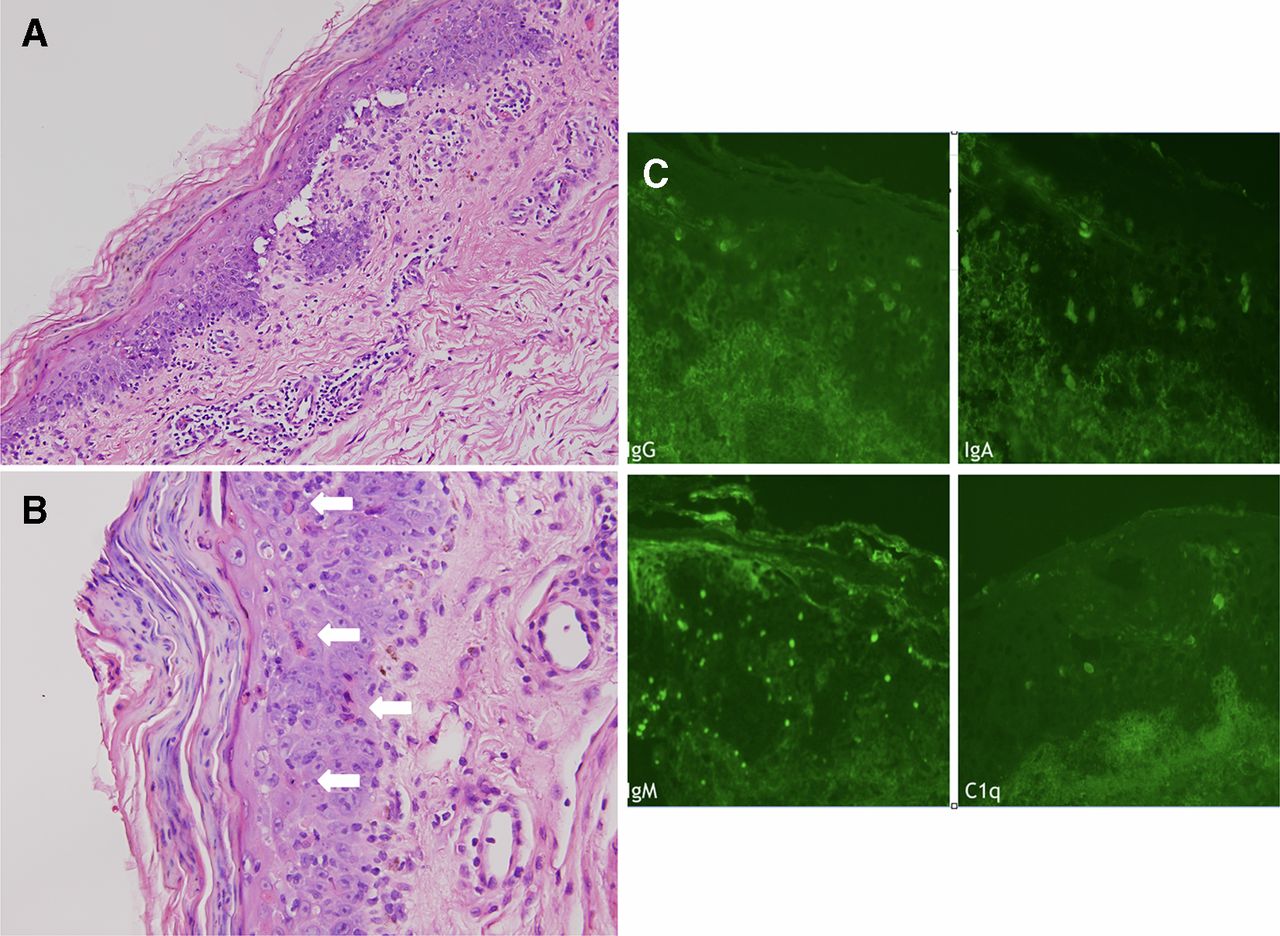
The laboratory test, including complete blood cell count and biochemistry, showed a mildly elevated white blood cell count (11×109/L) and aspartate aminotransferase level (54 U/L). The acetylcholine receptor autoantibody level (5.34 nmol/L) and anticardiolipin IgM (13.4 MPL) were elevated, the antibodies against extractable nuclear antigens were positive and the titer of antinuclear antibody was 1:40 with homogeneous pattern. Other tests for autoantibodies, including antithyroglobulin antibodies, antithyroperoxidase antibodies, anti-double stranded DNA antibody, anti-SSA, anti-SSB, IgG anticardiolipin, anti-phospholipid IgG and IgM, basement membrane zone antibody, intercellular substance antibody, lupus anticoagulant test C3 and C4 quantification and thyroid hormones were negative or within normal ranges. Cultures of the discharge from the skin lesion over the leg revealed growth of methicillin-susceptible Staphylococcus aureus and methicillin-resistant S. epidermidis. The first skin biopsy from the abdomen showed lichenoid interface dermatitis. The second skin biopsy from the left arm showed interface dermatitis, and direct immunofluorescence staining revealed no evidence of pemphigus or pemphigoid (figure 3). CT of the chest revealed a tumour in the anterior mediastinum with the greatest dimension measuring 14.0×10.2×8.2 cm (figure 1B), multiple pleura-based tumours and a massive pleural effusion with septation of the right lung. A diagnosis of thymoma was confirmed through sonography-guided biopsy of the mediastinal mass.
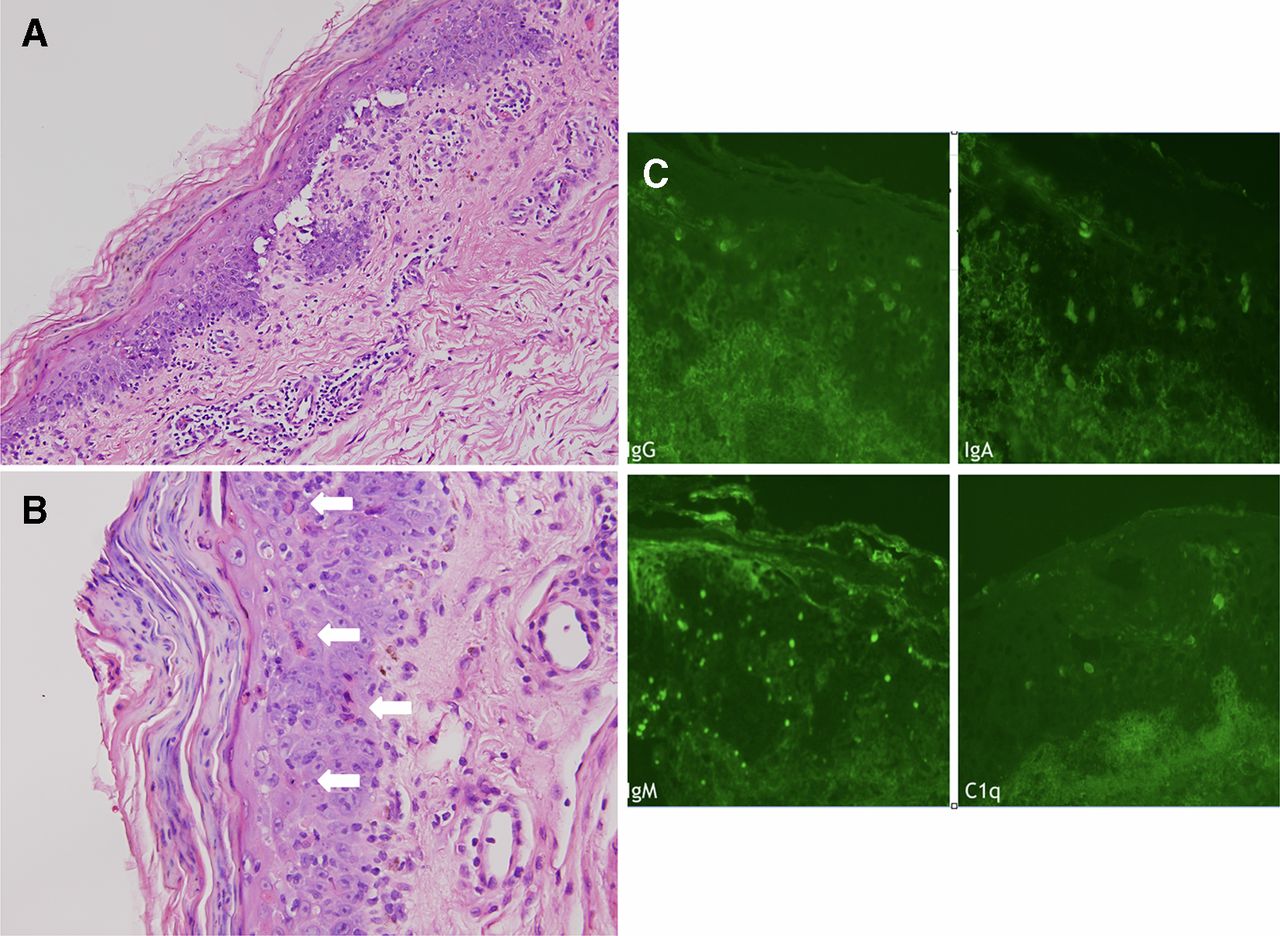
(A) H&E, 200×: interface dermatitis with dyskeratotic cells and confluent parakeratosis; dermis shows a perivascular infiltrate of lymphocytes with scattered eosinophils. (B) H&E, 400×: frequent dyskeratosis (arrows) and confluent parakeratosis. (C) Direct immunofluorescence staining: several cytoid bodies (under IgG, IgA, IgM and C1q staining) in the lower epidermis, dermal–epidermal junction and upper dermis. There was no intercellular or linear basement membrane pattern deposition.
Differential diagnosis
The interface changes of the skin may be presented in various diseases such as lupus erythematosus, lichen planus, drug reaction and graft versus host disease (GVHD). There was no identifiable culprit drug, and the clinical manifestation did not meet the 2012 systemic lupus international collaborating clinics criterita. Direct immunofluorescence staining showed no evidence of pemphigus or pemphigoid. Based on the patient’s clinical history, physical findings and histopathology, the lesions of the skin were mostly consistent with graft-versus-host-like erythroderma, a manifestation of thymoma-associated multiorgan autoimmunity (TAMA), which was complicated with cellulitis of the legs.
Treatment
The patient underwent sternotomy and right thoracotomy for thymectomy, partial pleurectomy and excision of the tumour involving the diaphragm and right lung. A diagnosis of thymoma, Masaoka stage IVA and WHO type B2 and B3, with invasion to the right lung and metastasis to the right pleural cavity was made (figure 4). Cellulitis of the legs resolved with the administration of vancomycin. Erythrodermic changes of the skin improved but the oral erosion persisted postoperatively and after the administration of intravenous methylprednisolone at a daily dose of 80 mg, which was tapered to 10 mg/day of oral prednisolone as maintenance therapy (figure 5).
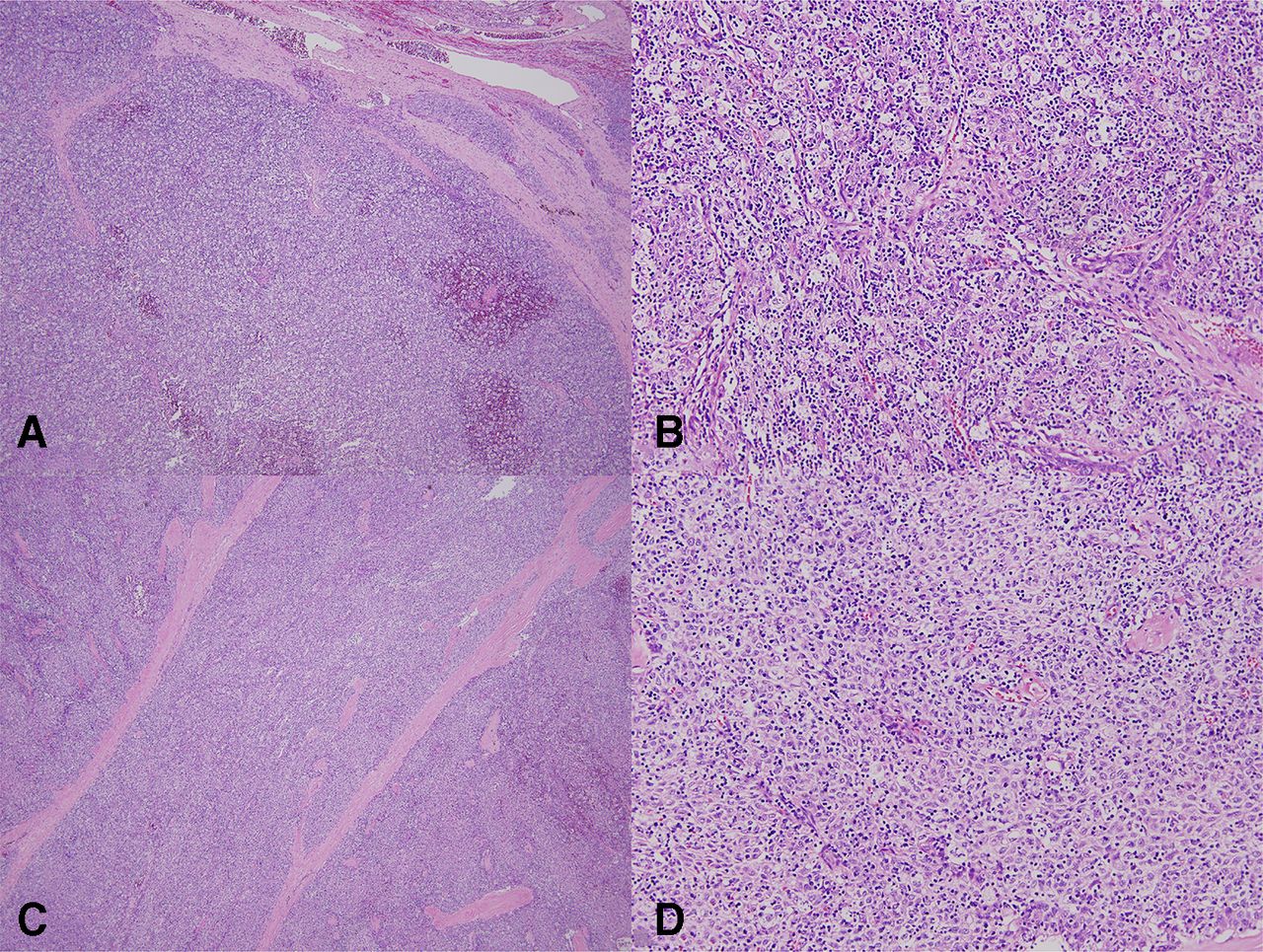
(A) H&E, 40x type B2 thymoma with a bluish appearance at low magnification and lung invasion. (B) H&E, 200x, type B2 thymoma with small lymphocytes mixed with some aggregates of epithelial cells. (C) 40x, type B3 thymoma with a pink appearance at low magnification (D) type B3 thymoma with a predominance of polygonal epithelial cells.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Skin lesions of the trunk 24 days after operation.
Outcome and follow-up
One month after the operation, cytomegalovirus (CMV) pneumonitis with respiratory failure developed, which responded to ganciclovir therapy.
Discussion
Thymomas are the most common tumours arising from the anterior mediastinum. The presentation of thymoma could be asymptomatic, related to the mass effects from tumour compression of the mediastinal structure, or as paraneoplastic syndromes. Approximately 30%–44% of the patients with thymoma present with myasthenia gravis. Other autoimmune disorders are considerably less frequent, such as hypogammaglobulinemia, pure red cell aplasia and systemic lupus erythematosus.1 The thymus is essential for the development of T-cells. In the abnormal microenvironment of thymoma, the positive and negative selection of T-cells is compromised, resulting in a broad spectrum of autoimmune-mediated diseases.2 In 2007, Wadhera et al proposed a new term, TAMA, to describe the unique graft-versus-host-like manifestations in patients with thymoma.3 TAMA was defined as diseases of the skin, liver and intestines that resemble GVHD histopathologically in the context of thymoma rather than in allogeneic haematopoietic cell transplantation.
In this patient, mucocutaneous lesions, including oral lichen planus and GVHD-like erythroderma, were the sole manifestation of TAMA. Although the patient’s acetylcholine receptor autoantibody level was elevated, he did not present with the typical symptoms of myasthenia gravis, such as ptosis, dysphagia and proximal muscle weakness. The patient’s GVHD-like erythroderma promptly improved after thymectomy and the administration of intravenous methylprednisolone, which, however, was complicated by CMV pneumonitis and respiratory failure 1 month after operation and immunosuppression. Current treatment options for GVHD-like skin lesions related to TAMA include thymectomy, systemic glucocorticoids, intravenous immunoglobulin, cyclosporine and narrow-band ultraviolet B phototherapy, with varying results.3–5 Two case reports have described the resolution of skin lesions with complete resection of thymoma without the use of systemic glucocorticoids.6 7 Motoishi et al reported a case of a 69-year-old woman with a GVHD-like disease with skin manifestations that were successfully treated with thymectomy and topical steroids, which suggests that complete resection of the thymoma could improve such skin lesions.6 However, systemic glucocorticoids for TAMA and other autoimmune diseases may increase the risk of severe infections.7 Given the rarity of this disease, studies that compare the efficacy of different treatments for GVHD-like erythroderma of TAMA are lacking.
Our patient presented with oral lichen planus 4 years before the diagnosis of thymoma. The oral lesion could be a manifestation of paraneoplastic syndrome, even though it presented much earlier than the diagnosis of the neoplasm. In 2001, Nguyen et al suggested a new term, ‘paraneoplastic autoimmune multiorgan syndrome (PAMS)’, to describe the heterogeneous autoimmune syndrome associated with neoplasm. The patient with PAMS may present with a spectrum of different clinical and immunopathological mucocutaneous variants (ie, pemphigus-like, pemphigoid-like, erythema multiform-like, graft-vs-host disease-like and lichen planus-like).8 TAMA, with the characteristic of thymoma and various autoimmune disorders, is in accordance with the definition of PAMS. The oral lesion did not improve with systemic glucocorticoids or after thymoma excision. Currently, no consensus has been reached on the treatment of oral erosive lichen planus associated with thymoma. Regression of lichen planus by thymectomy, oral prednisolone, oral etretinate or immunoglobulin infusion has been described.9 According to a literature review of 30 case reports of lichen planus associated with thymoma, most patients presented with oral erosive lichen planus, and oral lesions usually did not regress after thymectomy.10 Given the available data, the association of intractable oral lichen planus and thymomas warrants further investigations.
In conclusion, complete resection of the thymoma could lead to resolution of GVHD-like erythroderma related to TAMA, but the oral lichen planus tends to be more resistant. More studies are required to identify the optimal treatment of GVHD-like erythroderma related to TAMA, and in particular, to examine the role of systemic glucocorticoids that may cause immunosuppression and confer a high risk of severe infections.
Learning points
Thymoma-associated multiorgan autoimmunity (TAMA) is a rare paraneoplastic syndrome that complicates thymoma, which can involve the thyroid, liver, intestine and skin.
Complete resection of the thymoma could lead to resolution of graft versus host disease-like erythroderma related to TAMA.
Intractable oral lichen planus may warrant further investigation for thymoma.
Footnotes
Contributors Conception and design of the work: C-TH, J-SC. Data collection: C-TH, J-SC. Data analysis and interpretation: C-TH, J-SC. Drafting the article: C-TH. Critical revision of the article: T-FT, M-SH. Final approval of the article: C-TH, J-SC, T-FT, M-SH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None to declare
Ethics approval This case report was waived for ethics approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.