Article Text

Abstract
Introduction To assess the effect of exenatide and pioglitazone or basal-bolus insulin on diabetic peripheral neuropathy (DPN) in patients with poorly controlled type 2 diabetes (T2D).
Research design and methods This is a substudy of the Qatar Study, an open-label, randomized controlled trial. 38 subjects with poorly controlled T2D were studied at baseline and 1-year follow-up and 18 control subjects were assessed at baseline only. A combination of exenatide (2 mg/week) and pioglitazone (30 mg/day) or glargine with aspart insulin were randomly assigned to patients to achieve an HbA1c <53 mmol/mol (<7%). DPN was assessed with corneal confocal microscopy (CCM), DN4, vibration perception and sudomotor function.
Results Subjects with T2D had reduced corneal nerves, but other DPN measures were comparable with the control group. In the combination treatment arm (n=21), HbA1c decreased by 35.2 mmol/mol (3.8 %) (p<0.0001), body weight increased by 5.6 kg (p<0.0001), corneal nerve branch density increased (p<0.05), vibration perception worsened (p<0.05), and DN4 and sudomotor function showed no change. In the insulin treatment arm, HbA1c decreased by 28.7 mmol/mol (2.7 %) (p<0.0001), body weight increased by 4.6 kg (p<0.01), corneal nerve branch density and fiber length increased (p≤0.01), vibration perception improved (p<0.01), and DN4 and sudomotor function showed no change. There was no association between the change in CCM measures with change in HbA1c, weight or lipids.
Conclusions Treatment with exenatide and pioglitazone or basal-bolus insulin results in corneal nerve regeneration, but no change in neuropathic symptoms or sudomotor function over 1 year.
- diabetic neuropathies
- pioglitazone
- Glucagon-Like Peptide 1
- insulin glargine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Improved glycemic control delays the progression of diabetic neuropathy in patients with type 1 diabetes but has a limited impact in type 2 diabetes.
Glucagon-like peptide 1 receptor agonists, thiazolidinediones and insulin have a neuroprotective effect independent of their glucose-lowering effect.
What are the new findings?
Treatment with exenatide and pioglitazone or basal bolus insulin was associated with corneal nerve regeneration, but no change in sudomotor function or neuropathic pain.
How might these results change the focus of research or clinical practice?
This study provides support for the role of corneal confocal microscopy as an endpoint in clinical trials of therapies for diabetic neuropathy.
Introduction
Diabetic peripheral neuropathy (DPN) affects 50% of patients with diabetes leading to neuropathic pain, erectile dysfunction and foot ulcers, and imposes a significant health and economic burden to both the patient and healthcare providers.1 While intensive glycemic control can prevent the onset or delay progression of DPN in type 1 diabetes (T1D),2 there are conflicting data in type 2 diabetes (T2D).3–9 Both glucagon-like peptide 1 (GLP-1) receptor agonists10 11 and thiazolidinediones (TZDs)5 12–14 produce a durable reduction in HbA1c.15 GLP-1 receptor agonists stimulate insulin secretion in response to hyperglycemia, delay gastric emptying leading to weight loss and inhibit hepatic glucose secretion, while TZDs are potent insulin sensitizers and improve β-cell function. In preclinical studies, exendin-4, a GLP-1 receptor agonist, prevented sensory10 and motor nerve conduction slowing11 and a reduction in intraepidermal nerve fiber density (IENFD) in T1D mice. However, twice-daily exenatide showed no effect on DPN in patients with T2D.16 TZDs prevent nerve conduction slowing,12 maintain myelinated fiber density and reduce macrophage infiltration in the sciatic nerve.13 TZDs have been shown to reduce the incidence of DPN in patients with T2D.5
There are currently no FDA-approved therapies for DPN, despite multiple clinical trials. It has been suggested that the endpoints in these trials may not be sufficiently sensitive to detect a change in DPN.17 Several studies have provided support for the prevailing hypothesis that early subclinical small fiber injury precedes large fiber damage in DPN.18 19 In this study, corneal confocal microscopy (CCM) was used to assess early small nerve fiber repair. Several longitudinal studies have shown that a lower corneal nerve fiber length (CNFL) at baseline predicts those patients who develop DPN.20–22 CCM has also been used to identify early small fiber repair in several small clinical trials.23 24 Indeed, CCM identified early corneal nerve regeneration 6 months after pancreas and kidney transplantation which was followed by an improvement in neuropathic symptoms and nerve conduction after 24 months.25 26
The Qatar Study15 is an open-label, randomized controlled trial, which showed a rapid and effective reduction in HbA1c after treatment with a combination of exenatide and pioglitazone or basal-bolus insulin in patients with poorly controlled T2D. This is a substudy of the Qatar Study designed to assess the effect of the two treatment arms on DPN with CCM as a primary outcome measure and DN4, vibration perception threshold (VPT) and sudomotor function as secondary outcome measures. This study also evaluated the effect of the treatments on diabetic retinopathy.
Materials and methods
This is a prospective substudy of the Qatar Study,15 an open-label, randomized controlled trial (ClinicalTrials.gov identifier NCT02887625) designed to examine the efficacy of exenatide plus pioglitazone versus basal-bolus insulin in patients with poorly controlled T2D on metformin plus sulfonylurea. This substudy was not registered in a publicly available clinical trial database as it was part of the larger Qatar Study. Subjects with T2D were enrolled from the National Diabetes Center in Hamad General Hospital and studied at baseline and 1-year follow-up, and control subjects without diabetes were enrolled from Rumailah Hospital and studied between October 2016 and November 2018.
Study cohort
Subjects were eligible to participate if they were between 18 and 75 years old, had poorly controlled (HbA1c >58 mmol/mol (7.5%)) T2D treated with a maximal dose of metformin (>1500 mg/day) plus sulfonylurea (>4 mg glimepiride or >60 mg gliclazide), had normal kidney and liver function and ECG, and stable body weight (±1 kg within the preceding year). Healthy controls had a HbA1c <6%.
Exclusion criteria were any cause of neuropathy other than diabetes (chemotherapy, HIV infection and hepatitis C), factors that may affect the corneal nerves (severe dry eyes, severe corneal dystrophies, ocular trauma or surgery in the preceding 6 months), a hematocrit <34%, medications known to affect glucose metabolism other than sulfonylureas and metformin, evidence of diabetic proliferative retinopathy, albumin excretion >300 mg/day and major organ system disease, as determined by physical examination, medical history and screening blood tests.
Interventions
In the Qatar Study, eligible subjects were randomized to receive exenatide plus pioglitazone or glargine and aspart to achieve and maintain an HbA1c <53 mmol/mol (<7%). There was no limit on the upper value of HbA1c for enrollment. Subjects randomized to combination treatment were started on weekly subcutaneous extended release exenatide (2 mg/week Bydureon) and pioglitazone (30 mg/day). Subjects receiving insulin were started on glargine before breakfast. The Treat-to-Target Trial (4T) algorithm was used to calculate the starting glargine dose, and the dose was adjusted weekly to achieve a fasting plasma glucose (FPG) of <6.11 mmol/L. After the FPG goal was achieved, if the HbA1c was >53 mmol/mol (>7.0%), 4–6 U of insulin aspart was started before each meal, and the dose was adjusted to achieve a post-prandial plasma glucose concentration of <7.78 mmol/L, 2 hours after meals. Patients were seen monthly during the first 4 months or as needed, based on the results of the plasma glucose concentration, and bimonthly thereafter. The percentage of subjects experiencing hypoglycemia during the 1-year trial was calculated as the number of subjects experiencing at least one single episode of hypoglycemia (blood glucose concentration <60 mg/dL with or without symptoms or hypoglycemic symptoms that subsided following glucose ingestion) divided by the number of patients in that arm as per the protocol in the Qatar Study.15
Diabetic neuropathy assessment
CCM was performed using a Heidelberg Retina Tomograph 3 with the Rostock Cornea Module (Heidelberg Engineering GmbH). The CCM uses a 670 nm diode laser and provides digital images of the cornea. The technique has been previously described.27 Briefly, both eyes were anesthetized using oxybuprocaine hydrochloride 0.4% (Conjuncain EDO; Fabrik GmbH) followed by a drop of carbomer 0.2% eye gel (Blumont Healthcare), and patients were instructed to fixate on a target. Several scans of the sub-basal nerve plexus in the central cornea were captured per eye for 2 min. Adjacent images were separated by approximately 1–4 µm. CCM image extraction was carried out at a separate time by one investigator unaware of the treatment group. Three high-clarity CCM images per eye were selected based on a previously published protocol,27 and images were selected based on depth, focus position and contrast.28 Corneal nerve fiber density (CNFD) (fibers/mm2), corneal nerve branch density (CNBD) (branches/mm2) and corneal nerve fiber length (CNFL) (mm/mm2) were quantified using CCMetrics, a validated image analysis software.29
Vibration perception threshold (VPT) was measured using a Neurothesiometer (Horwell Scientific Laboratory Supplies) on the pulp of the large toe on both feet and the average value of three measurements was recorded as a VPT in volts (V) ranging from 0 to 50 V.
Sudomotor function was measured by electrochemical skin conductance (ESC) using Sudoscan (Impeto Medical SAS) as described previously. Sudoscan evaluates sympathetic innervation based on sweat chloride concentrations generated by the sweat gland in response to the voltage applied and is reported as ESC in microSiemens (µS).
Neuropathic pain was assessed using the Douleur Neuropathique en 4 (DN4) questionnaire as previously described.26
Diabetic retinopathy assessment
Ophthalmic examination was carried using a non-contact slit-lamp biomicroscope (Topcon) with +90 D lens (Volk) and two digital retinal images of both eyes were taken using a digital fundus camera (Zeiss) after pupil dilatation with Tropicamide 1% in 16/21 patients in the combination treatment group and 9/17 patients in the insulin treatment group. Diabetic retinopathy was graded by two qualified investigators according to the NHS Diabetic Eye Screening Programme.30 Diabetic retinopathy was graded as R0 for no diabetic retinopathy; R1 for the presence of microaneurysms, retinal hemorrhages, venous loops, exudates or cotton wool spots in the presence of other features of diabetic retinopathy; and R2 for the presence of venous beading, reduplication, multiple blot hemorrhages or intraretinal microvascular abnormality. Diabetic proliferative retinopathy (R3) was an exclusion criterion. Maculopathy was defined as M0 for no maculopathy or for any microaneurysm or hemorrhage within 1 disc diameter of the center of the fovea if associated with a best visual acuity of 6/12 where the cause of the reduced vision is known and is not diabetic macular edema and M1 for exudate, retinal thickening, microaneurysm or hemorrhage within 1 disc diameter of the center of the fovea or a group of exudates within the macula.
Outcome measures
The primary outcome measures were the CCM measures and the secondary outcome measures were DN4, VPT and sudomotor function.
Statistical analysis
This substudy was not adjusted for multiple comparisons.31 The results were analyzed as an exploratory study. Continuous variables between controls, subjects with T2D treated with exenatide plus pioglitazone and insulin were compared using one-way ANOVA. Continuous variables between the two groups were compared using an unpaired t-test. Categorical variables were compared using χ2. Changes between baseline and 1-year follow-up were compared using a paired t-test. Correlation of the change in CCM measures with the change in HbA1c, body weight and lipids were analyzed using the Pearson correlation coefficient. All analyses were performed using IBM-SPSS (V.23). A two-tailed p value of ≤0.05 was considered significant.
Results
Baseline characteristics
The exenatide plus pioglitazone (n=21) and insulin (n=17) group had comparable HbA1c (92.5±18.8 mmol/mol (10.6%±1.7%) vs 89.9±22.5 mmol/mol (10.4%±2.1%), p=0.7) and significantly higher than the control group (41.6±5.0 mmol/mol (6.0%±0.5%), p<0.0001) (table 1). The mean age, gender, lipid profile, diastolic blood pressure, body weight and body mass index (BMI) were comparable between all three groups. The systolic blood pressure in the combination treatment group was significantly lower than in the control group (126.4 mm Hg vs 143.7 mm Hg, p<0.05). The percentage of patients with diabetic retinopathy was comparable between the two treatment groups (31.3% vs 44.4%, p=0.51).
Baseline characteristics of patients with type 2 diabetes who received exenatide plus pioglitazone or insulin treatment
The combination treatment group had significantly lower CNFD (fibers/mm2) (26.1 vs 33.7, p=0.01), CNBD (branches/mm2) (57.0 vs 110.4, p<0.001) and CNFL (mm/mm2) (17.8 vs 25.1, p=0.0001) compared with the control group. The insulin treatment group had significantly lower CNBD (70.3 branches/mm2, p<0.01) and CNFL (19.4 mm/mm2, p<0.01) compared with the control group. There was no difference in vibration perception threshold and sudomotor function measured by electrochemical skin conductance between the three groups and the percentage of patients with neuropathic pain (DN4 >4) was comparable between the treatment groups.
Change in clinical and metabolic variables
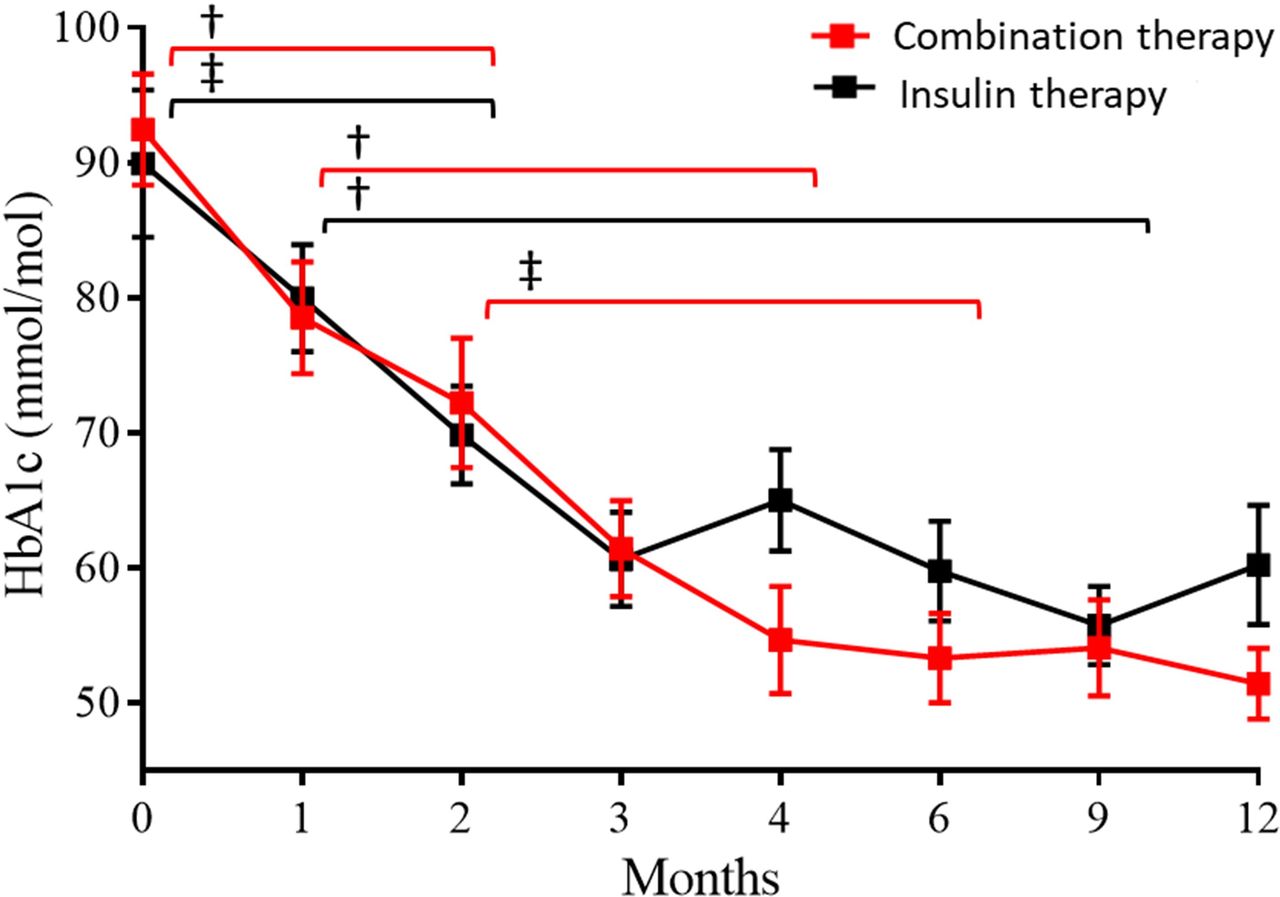
HbA1c reduced significantly in both treatment groups (p<0.0001), more so with exenatide plus pioglitazone compared with basal-bolus insulin (35.2 mmol/mol (3.8%) vs 28.7 mmol/mol (2.7%), p<0.05) (figure 1). The mean HbA1c at 1-year follow-up was lower but not significant in the combination treatment group (51.4±12.0 mmol/mol (6.9%±1.1%) vs 60.2±18.2 mmol/mol (7.7%±1.7%), p=0.1) (table 2). A higher percentage of patients achieved the American Diabetes Association treatment goal of HbA1c <53 mmol/mol (<7.0%) in the combination treatment group compared with the insulin treatment group (15/21 (71.4%) vs 6/17 (35.3%), p<0.05). The percentage of patients with hypoglycemia in the insulin group was significantly higher than the combination group (84.6% vs 38.1%, p=0.008).

Effect of exenatide plus pioglitazone and insulin treatment on HbA1c over 1 year. Overall HbA1c changes between different time points were compared using paired t-test: ‡p≤0.05, †p≤0.01, ††p≤0.001, †††p≤0.0001.
Changes in clinical and metabolic variables and measures of DPN after 1 year of exenatide plus pioglitazone or insulin treatment
Body weight increased by 4.6 kg in the insulin group and by 5.6 kg in the combination treatment group (p<0.01) (figure 2).

Effect of exenatide plus pioglitazone and insulin treatment on HbA1c, lipid profile, blood pressure, body weight, corneal nerve fiber measures, vibration perception threshold and sudomotor function in the feet over 1-year follow-up. DBP, diastolic blood pressure; ESC, electrochemical skin conductance; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure; VPT, vibration perception threshold.
In both treatment groups, total cholesterol decreased by 0.5–0.8 mmol/L (p<0.05–0.001). In the combination treatment group, triglycerides decreased by 0.4 mmol/L (p<0.05) and diastolic blood pressure decreased by 8.9 mm Hg (p<0.0001) and high-density lipoprotein cholesterol (HDL) increased by 0.4 mmol/L (p<0.01).
Change in neuropathy measures
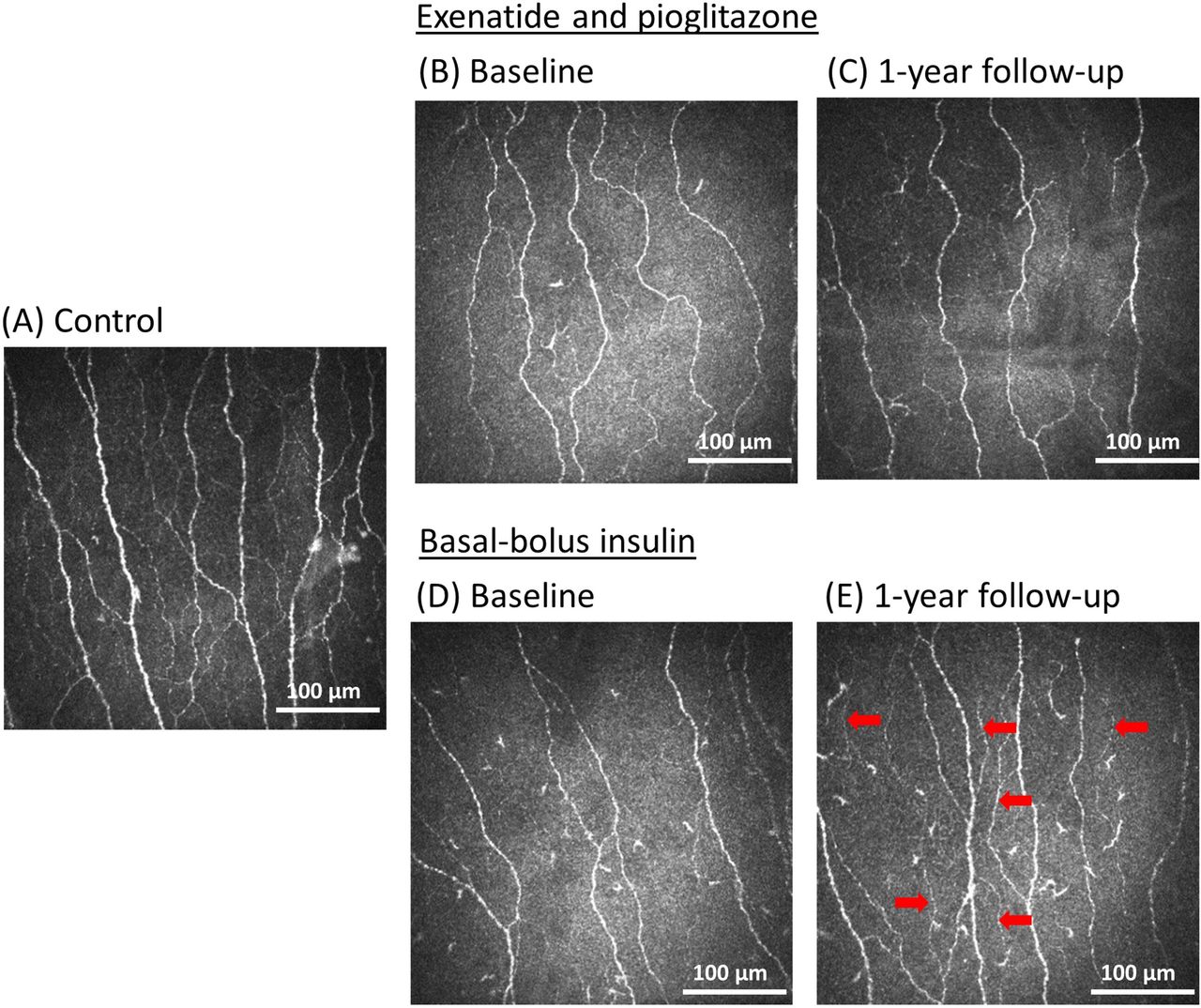
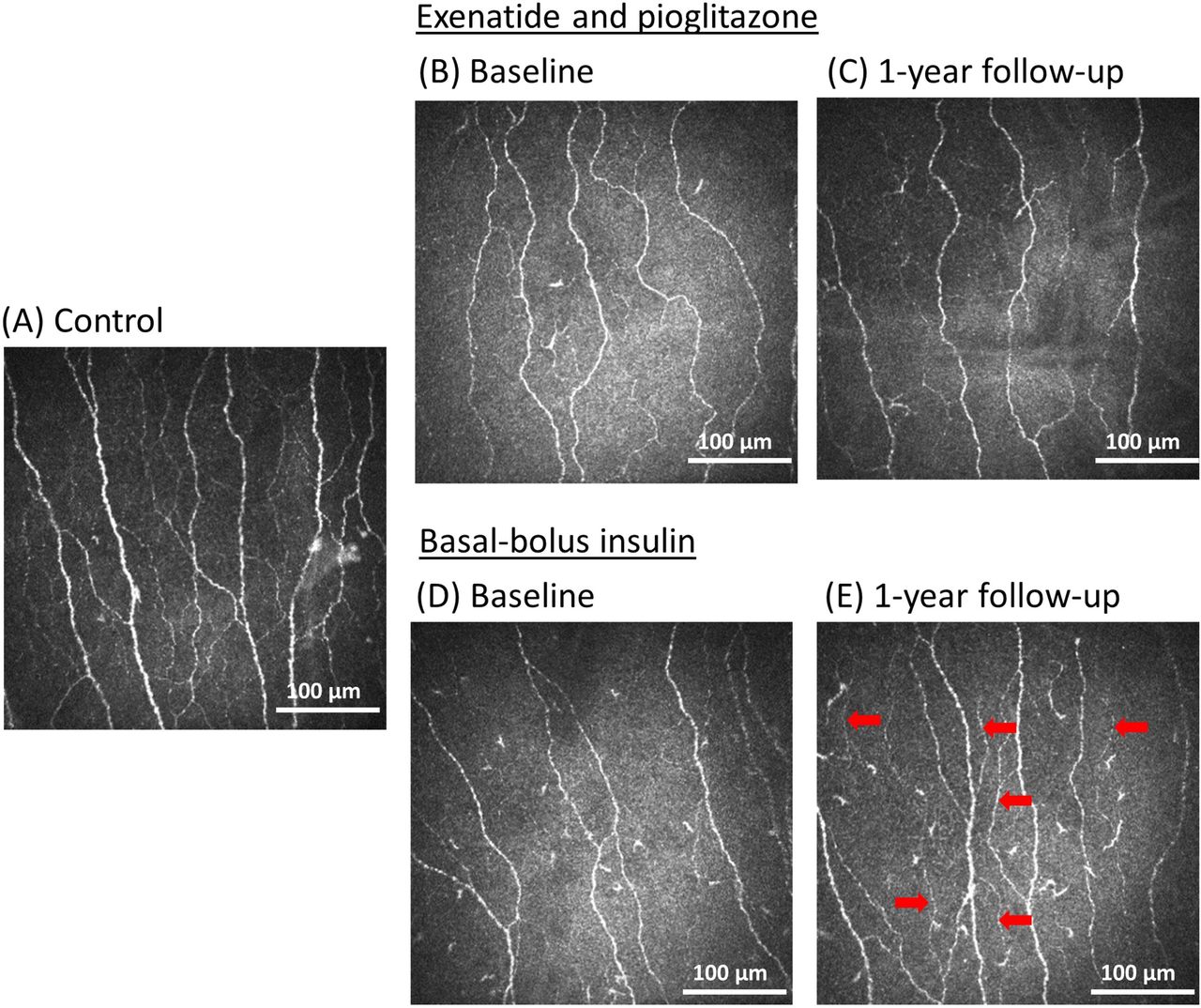
In the insulin treatment group, CNBD and CNFL increased by 27.2 branches/mm2 (p=0.01) and 2.3 mm/mm2 (p<0.01), respectively, with no change in CNFD (figures 2 and 3). In the exenatide plus pioglitazone treatment group, CNBD increased by 19.0 branches/mm2 (p=0.02) with no change in CNFD (p=0.76) and CNFL (p=0.12). Between the treatment groups, the change in CNFD (26.6 fibers/mm2 vs 30.8 fibers/mm2, p=0.11), CNBD (76.0 branches/mm2 vs 97.4 branches/mm2, p=0.20) and CNFL (19.7 mm/mm2 vs 21.7 mm/mm2, p=0.28) were comparable.
{kind=link}
{kind=link}
{kind=link}
Corneal confocal microscopy images of the sub-basal nerve plexus. Corneal nerve morphology in healthy age-matched controls (A), people with type 2 diabetes treated with exenatide and pioglitazone (B, C) and basal-bolus insulin (D, E) at baseline and 1-year follow-up. The red arrows indicate the fibers that might have increased the measurement of nerve branches and fiber length in the insulin treatment group at 1-year follow-up.
Vibration perception threshold decreased by 2.8 V (p<0.01) in the insulin treatment group and increased by 1.7 V (p<0.05) in the combination treatment group, with a significant difference between the two treatment groups at 1-year follow-up (p=0.001) (table 2 and figure 2).
There was no significant change in the percentage of patients with neuropathic pain (DN4 >4). There was no change in sudomotor function in either treatment group (table 2).
Correlation between change in CCM measures with change in Hb1Ac, lipids and weight
There was no correlation between the percentage change in CNFD with percentage change in HbA1c (r=0.06, p=0.74), total cholesterol (r=0.16, p=0.37), triglycerides (r=0.20, p=0.25), HDL (r=0.08, p=0.66) and weight (r=0.24, p=0.17). There was no correlation between percentage change in CNBD with percentage change in HbA1c (r=0.01, p=0.95), total cholesterol (r=0.06, p=0.74), triglycerides (r=0.08, p=0.64), HDL (r=0.06, p=0.73) and weight (r=0.25, p=0.14). There was no correlation between percentage change in CNFL with percentage change in HbA1c (r=0.05, p=0.77), total cholesterol (r=0.12, p=0.49), triglycerides (r=0.14, p=0.42), HDL (r=0.04, p=0.82) and weight (r=0.03, p=0.84).
Diabetic retinopathy
The percentage of patients with new-onset diabetic retinopathy increased significantly from 31.3% to 81.3% (p<0.01) in the combination treatment group and while there was an increase in the insulin treatment group from 44.4% to 66.7%, this was not significant (table 2). Eight subjects in the combination treatment group and two subjects in the insulin group progressed from R0 to R1. There was no progression of retinopathy in subjects graded R1, R2, M0 or M1 at baseline.
Discussion
This study shows that combination treatment with exenatide plus pioglitazone or basal-bolus insulin over 12 months results in a marked improvement in HbA1c, but with weight gain, and hypoglycemia, consistent with the Qatar Study.15 Insulin treatment was associated with a significant improvement in distal corneal nerve morphology characterized by an increase in corneal nerve branch density and length and an improvement in vibration perception, but no change in sudomotor function or incidence of neuropathic pain. Combination treatment was associated with an improvement in the lipid profile, blood pressure and an increase in distal corneal nerve branch density, but a small but significant deterioration in VPT with no change in sudomotor function or incidence of neuropathic pain. The improvement in CCM measures were independent of changes in HbA1c, body weight and lipids. There was an increase in the incidence of diabetic retinopathy in the combination treatment group.
While exenatide results in weight loss,16 pioglitazone is associated with weight gain, explaining the increase in weight observed in the combination treatment group. Obesity32 is a risk factor for DPN. Jaiswal et al16 reported that exenatide resulted in 3 kg weight loss after 1 year, compared with 2 kg weight gain with glargine.4 6 Pioglitazone is associated with a lowering of diastolic blood pressure and triglycerides, and we also observed a significant reduction in diastolic blood pressure and triglycerides in the combination treatment group. Hypertension33 and hyperlipidemia34 are also risk factors for DPN. However, the weight gain in both treatment arms may have limited the overall benefit on neuropathy.
Glucagon-like peptide 1 (GLP-1) receptor agonists have been reported to have a neuroprotective effect. In preclinical studies, Himeno et al11 showed that exendin-4 prevented both sensory and motor nerve conduction slowing and reduction of IENFD. However, Kan et al10 reported that exendin-4 prevented sensory nerve conduction slowing but had no effect on motor nerve conduction slowing and epidermal innervation. Conversely, in T2D mice, exendin-4 prevented motor nerve conduction slowing but had no effect on sensory nerve conduction. In a clinical trial of patients with T2D treated with exenatide, there was no effect on the incidence of DPN, cardiovascular autonomic neuropathy (CAN) or IENFD over 18 months.16 Recently, the LEADER trial35 showed that liraglutide was associated with a significantly lower risk of amputations related to diabetic foot ulceration in patients with T2D. However, a study of 39 patients with T1D and established neuropathy randomized to liraglutide or placebo over 26 weeks recently failed to show a benefit on autonomic function or sensory and motor nerve conduction.36 TZDs have also been reported to have a neuroprotective effect. In preclinical studies, Qiang et al12 reported that troglitazone prevented nerve conduction slowing and maintained normal myelinated fiber architecture and density in T1D rats. Yamagishi et al13 confirmed that pioglitazone prevented nerve conduction slowing and reduced macrophage infiltration in the sciatic nerve in T1D rats. Wiggin et al14 showed that rosiglitazone prevented thermal hypoalgesia and reduced oxidative stress in the sciatic nerve of T1D mice. In the BARI 2D trial,5 rosiglitazone significantly reduced the 4-year cumulative incidence of DPN compared with insulin treatment. The neuroprotective effect of TZDs may be attributed to a reduction in oxidative stress and advanced glycated end products. Our data suggest that exenatide plus pioglitazone treatment may be associated with small fiber regeneration, assessed using CCM.
In preclinical studies, Kan et al10 reported that high-dose insulin prevented a reduction of IENFD in T1D mice but had no effect in T2D mice. In the DCCT, intensive insulin treatment reduced the incidence of clinical DPN by 60%2 and prevented peroneal nerve conduction velocity slowing over a 5-year period in patients with T1D. However, in patients with T2D, the UKPDS6 and VA-CSDM trial7 reported that intensive treatment had no effect on the incidence of DPN and CAN compared with conventional treatment. The Kumamoto study3 showed that intensive treatment prevented nerve conduction slowing over 6 years and the ACCORD trial4 showed a reduction in the incidence of loss of ankle reflexes but no effect on VPT over 6 years.8 Our data suggest that insulin treatment might have a beneficial effect on DPN, independent of the improvement in glycemic control as there was evidence of greater small nerve fiber regeneration and an improvement in vibration perception. In a previous study comparing continuous subcutaneous insulin infusion (CSII) with multiple daily insulin injection, we showed that despite a comparable HbA1c, the CSII group showed an increase in CNFD, CNBD and CNFL,37 which was attributed to a direct neurotrophic effect of insulin.38
Both combination and insulin treatment improved corneal nerve fiber measures but had no effect on neuropathic symptoms or sudomotor function over 1 year. This is consistent with studies showing corneal nerve regeneration 6 months after pancreas and kidney transplantation in T1D with no change in quantitative sensory testing and an improvement in neuropathic symptoms and nerve conduction at 24 and 36 months.25 26 39 Autonomic function has not been shown to improve 3, 8 and 10 years after kidney and pancreas transplantation,26 40 41 but multifactorial risk factor reduction showed an improvement in cardiac autonomic function with no change in vibration perception threshold.42 A recent study from Japan showed that multifactorial risk factor reduction achieved by improving and even normalizing glycemic control and reducing body weight and blood pressure in patients with T2D over 4 years resulted in an improvement in CNFL, CNBD, neurophysiology and vibration perception, which correlated with the reduction in HbA1c.43 The present study shows an improvement in CNBD and CNFL, but no change in sudomotor function over 12 months. Jaiswal et al16 reported a trend for a greater increase in IENFD 1 year after capsaicin denervation in patients on insulin compared with exenatide. In a randomized placebo-controlled trial of once-weekly C-peptide, there was no improvement in sural nerve conduction velocity or the modified Toronto Clinical Neuropathy Score and yet vibration perception threshold improved significantly.44 These findings emphasize the importance of the type and duration of intervention and choice of endpoints in clinical trials of DPN.
A large improvement in HbA1c (>2%–3%) has been reported to be associated with treatment-induced neuropathic pain, autonomic neuropathy, and a worsening of retinopathy and microalbuminuria.45 Our study shows that despite a reduction in HbA1c of 3.8% with a combination of exenatide and pioglitazone and 2.7% with insulin, there was no increase in the incidence of painful DPN. However, the genesis of painful neuropathy is complex and may involve alterations in transient receptor potential channels, which may not have been altered by the current interventions.46 The incidence of diabetic retinopathy increased, especially in the combination treatment group. GLP-1 therapy has been associated with an increase in the risk of retinopathy progression in patients with diabetic retinopathy in a large randomized trial with semaglutide,47 although two large population-based analyses have failed to confirm this association.48 49 Treatment with lixisenatide and once-weekly exenatide have previously shown no adverse effect on retinopathy.49
We acknowledge that this is a small open-label study with a lack of blinding for participants and investigators due to weekly exenatide injections and multiple daily insulin injections. However, the investigator that evaluated the neuropathy outcome measures was masked to the treatment group. Our cohort of patients with T2D had minimal neuropathy and a very effective reduction in HbA1c over 12 months leading to early small nerve fiber repair as observed after simultaneous pancreas–kidney transplantation26 or optimal medical therapy.43
In conclusion, exenatide plus pioglitazone or basal-bolus insulin treatment effectively reduces HbA1c and promotes small fiber regeneration. While the incidence of diabetic retinopathy increased, especially in the combination treatment group, there was no impact on neuropathic pain. Our findings support the utility of CCM as an early surrogate marker of therapeutic response in clinical trials of diabetic neuropathy.
Acknowledgments
We thank all the participants for their efforts and commitment to be involved in the study. Some of the data were presented as an abstract at the 54th EASD Annual Meeting in 2018.
References
Footnotes
Author contributions RAM and GP had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: MAA-G, AJ, RD, RAM and GP. Acquisition, analysis or interpretation of data: all authors. Drafting of the manuscript: RAM and GP. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: GP, ZM and RAM. Obtained funding: RAM. Administrative, technical or material support: all authors. All authors have read and approved the final manuscript.
Funding Qatar National Research Fund, Funding ID: BMRP-5726113101, Qatar National Research Fund, Funding ID: NPRP 5-273-3-079. AstraZeneca provided exenatide for the Qatar Study.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study obtained ethics approval by the Institutional Review Board of Hamad Medical Corporation (IRB no. 13-00076) and all participants gave informed consent before taking part in the study. The research adhered to the tenets of the declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article. The data sets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.