





Abstract
Undocumented migrants, in particular pregnant women and their newborns, constitute a particularly vulnerable group of migrants. The aim of this study was to systematically review the academic literature on the use and outcomes of maternal and child healthcare by undocumented migrants in the European Union (EU) and European Free Trade Association (EFTA) countries.
The databases, MEDLINE, Embase, CINAHL Plus, Global Health and Popline were searched for the period 2007 to 2017. Two independent reviewers judged the eligibility of studies. The final number of included studies was 33.
The results of quantitative, qualitative and mixed methods studies were analysed separately due to their differences in study design, sample size and quality. Overall, the quantitative studies found that undocumented women underutilised essential maternal and child healthcare services, and experienced worse health outcomes. Qualitative studies supported these results, indicating that undocumented migrants were hesitant to use services due to a lack of knowledge and fear of deportation. Studies included in the review covered 10 of 32 EU or EFTA countries, making a European comparison impossible.
Despite major methodological differences between included studies, the results of this review indicate that the status of undocumented migrants exacerbates known health risks and hampers service use.
Introduction
Immigration has become a permanent reality for most European countries.1 The latest statistics suggest a total of 55.8 million migrants living in the European Union (EU) in 2016.2 The topic of migration has gained traction in academia and mainstream society but limited research has focused on the group of undocumented migrants. The Platform for International Cooperation on Undocumented Migrants (PICUM)3 defines undocumented migrants as “migrants without a residence permit authorising them to regularly stay in the country of destination”. “They may have been unsuccessful in the asylum procedure, have overstayed visa or have entered irregularly.”3 Due to the difficulties of accurately measuring the number of undocumented migrants living in the EU, reliable statistics are extremely limited.3 The Clandestino project funded by the European Commission, estimated a total of 1.9–3.8 million undocumented migrants living in the EU-27 in 2009, constituting the most recent account for the EU.3 Estimates for individual European countries have also been drawn up, but they are subject to frequent change.3
Making sure migrants’ health is adequately taken care of is a matter of human rights and an essential way of tackling health inequalities.1 Maternal and child health is integral in this regard due to the increasing feminisation of migration, as well as pregnant women and children comprising an exceptionally vulnerable group of undocumented migrants.1 Both the utilisation and outcomes of maternal and child healthcare can act as indicators of social inequality; they can also be used to tailor and increase the responsiveness of health services to the needs of undocumented migrants. The utilisation of maternal and child healthcare services by undocumented migrants in the EU is influenced not only by their legal access, but also by language barriers, health literacy, economic issues, cultural differences or fear of deportation due to ones’ undocumented status.4 Cultural differences in beliefs concerning health and illness often trace back to a migrant’s country of origin and likely transcend the utilisation of services.5 Almeida and Caldas4 published a systematic review on maternal healthcare in migrants in 2013, focusing on access, use and quality of healthcare. Keygnaert et al. published the most recent systematic review on access to and quality of maternal healthcare for migrants in 2016.6 However, the link between the use and outcomes of maternal and child healthcare services is under-researched in the current academic literature, especially when it comes to undocumented migrants.
The aim of our study was to systematically review the academic literature on the use and outcomes of maternal and child healthcare services by undocumented migrants from 2007 to 2017 in the EU and EFTA countries. The focus was on undocumented pregnant women and their infants in the first year of life, in which vulnerability is highest.5
Methods
A systematic literature search was conducted in May 2017, using the scientific databases MEDLINE, Embase, CINAHL Plus, Global health and Popline. The initial search in each database was performed on 12 May 2017 and updated on 6 June 2017. After consultation with a librarian, the final search strategy with a total of 126 search terms was employed in each database (see Supplementary Appendix S1). Although grey literature is increasingly being used in systematic reviews in health sciences and Health services research, we decided to focus on scientific databases, as grey literature is usually not subject to rigorous peer-review, raising questions about quality and credibility. Our review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.7
Inclusion and exclusion criteria
Studies were deemed eligible for inclusion if they (i) were published between 2007 and 2017; (ii) were published in English, German or Dutch; (iii) had the geographical focus of one or more of the EU or EFTA countries; (iv) reported peer-reviewed, original qualitative or quantitative data; (v) focused or specifically included undocumented migrants as study participants; (vi) reported data on the utilisation or outcomes of maternal and child healthcare. Studies were excluded if they (i) were published prior to 2007; (ii) were published in a language other than English, German or Dutch; (iii) had a geographical focus outside the EU or EFTA countries; (iv) did not report original, peer-reviewed data (such as letters to the editors, reviews, reports, poster presentations and book chapters); (v) did not include undocumented migrants, in particular pregnant women and their children (limited to the first year of life) as their study participants; (vi) focused on access or quality of maternal and child healthcare services with no reference to utilisation or outcomes.
The initial database search was performed in Medline. An advanced search was conducted with a total of 126 ‘all fields’ and MeSH terms, taking notice of truncation symbols, and connecting the search terms with the Boolean operators OR and AND. MeSH terms were exploded (exp) and all subheadings included to ensure that the selected search terms as well as more narrow terms were retrieved. In addition to connecting the synonyms of the concept ‘undocumented’ and ‘migrant’ with Boolean operators, the two concepts were also connected with the adjacent (adj) operator. Thus, articles with the terms ‘undocumented’ adjacent to ‘migrant’ were also included within a distance of 10 spaces (adj10). The search was then extended to the other four databases, with database-specific adjustments if necessary. In the database Popline, only the search terms for ‘undocumented’, ‘migrant’ and ‘Europe’ were searched, as the thematic focus of Popline is reproductive health. The detailed search query can be found in Supplementary Appendix S1.
On the basis of the pre-defined inclusion and exclusion criteria, two independent reviewers made a first selection following screening of titles and abstracts. The lead author then performed a full-text screening. In case of disagreement in the selection process, a third reviewer was consulted. Studies were only included if all reviewers agreed. In addition, the reference lists of included studies were hand-searched by the lead author. Following deletion of duplicates, key data were extracted and collected in an Excel file. Key data included the general characteristics of the studies, specifically information on the group of undocumented migrants studied, the methodology used as well as the main study results related to the use and outcomes of maternal and child healthcare services by undocumented migrants. Thus, a qualitative content analysis was performed to synthesise the relevant information. Two quality assessment tools were used to evaluate the quality of quantitative and qualitative studies.8,9 The quality of the systematic review itself was ensured using the PRISMA 2009 Checklist7 (see Supplementary Appendix S2).
Results
The systematic literature search resulted in a total of 367 records. After deletion of duplicates, 288 studies were eligible for the screening of abstracts and titles by two independent reviewers, after which 199 were excluded on the basis of the pre-defined criteria. After full-text screening the remaining studies, 33 articles were included in the review, as illustrated in figure 1.
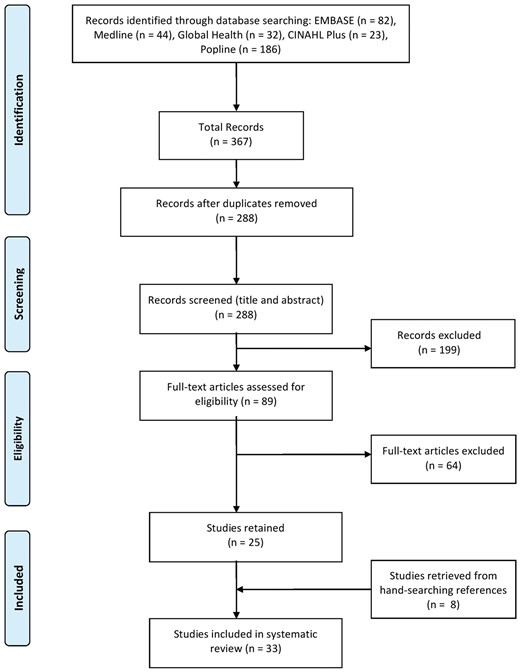
PRISMA flowchart
An overview of study characteristics is provided in table 1. Of the 33 included studies, 3 were published in German, while the rest were published in English. The included studies were conducted in only 10 of the 32 EU and EFTA countries, namely Denmark (n = 2), France (n = 1), Germany (n = 4), Italy (n = 5), Malta (n = 1), Netherlands (n = 4), Portugal (n = 6), Spain (n = 2), Switzerland (n = 5), United Kingdom (n = 2) and one study was conducted in both Germany and Italy. The majority of studies (n = 30) was performed at a local or regional level, while three studies were carried out at national level.
Description of included studies (n = 33)
| n (%) | References | |
|---|---|---|
| General characteristics of studies | ||
| Receiving countries | ||
| Denmark | 2 (6) | 10,11 |
| France | 1 (3) | 12 |
| Germany | 4 (12) | 13–16 |
| Italy | 5 (15) | 17–21 |
| Malta | 1 (3) | 22 |
| Netherlands | 4 (12) | 23–26 |
| Portugal | 6 (18) | 27–32 |
| Spain | 2 (6) | 33,34 |
| Switzerland | 5 (15) | 35–39 |
| United Kingdom | 2 (6) | 40,41 |
| Multi-country analysis | 1 (3) | 42 |
| Geographical setting | ||
| National | 3 (9) | 20,22,41 |
| Regional or local | 30 (91) | 10–19, 21, 23–40, 42 |
| Focus of the study | ||
| Use of maternal and child healthcare services | 12 (36) | 10, 13–17, 26, 28, 29, 31, 34, 42 |
| Both use and outcomes of maternal and child healthcare | 21 (64) | 11, 12, 16, 18–21, 23–25, 27, 30, 32, 33, 35–41 |
| Characteristics of undocumented migrants | ||
| Number of undocumented migrants included | ||
| Sample less than 500 | 23 (70) | 11, 15, 16, 21–28, 30–41 |
| Sample between 500 and 1000 | 4 (12) | 10, 12, 19, 29 |
| Sample more than 1000 | 6 (18) | 13, 14, 17, 18, 20, 42 |
| Percentage of undocumented migrants in total study sample | ||
| Less than 10% | 5 (15) | 12, 18, 19, 27, 39 |
| 10–49% | 12 (36) | 20–22, 28–33, 35, 37, 38 |
| 50–99% | 4 (12) | 14, 23, 40, 42 |
| 100% | 12 (36) | 10, 11, 13, 15–17, 24–26, 34, 36, 41 |
| Information on place of birth | ||
| Specific country of birth | 4 (12) | 32–34, 39 |
| Specific region of birth | 13 (39) | 12, 14, 15, 18–21, 26, 28, 31, 35, 37, 38 |
| Both specific country and region of birth | 14 (42) | 10, 11, 13, 16, 17, 22–25, 27, 29, 30, 36, 42 |
| Not reported | 2 (6) | 40, 41 |
| Information on reason for migration | ||
| Yes | 6 (18) | 15, 24–26, 38, 39 |
| No | 27 (82) | 10–14, 16–23, 27–37, 40–42 |
| Included study participants | ||
| Only undocumented migrants | 16 (48) | 10, 11, 13–17, 20, 24–26, 34, 36, 40–42 |
| Different migrant populations | 9 (27) | 12, 19, 21, 28–30, 32, 33, 39 |
| Undocumented migrants and comparator group | 8 (24) | 18, 22, 23, 27, 31, 35, 37, 38 |
| Methodological characteristics | ||
| Study design | ||
| Quantitative | ||
| Cross-sectional | 14 (42) | 10, 11, 13, 14, 17–19, 22, 27–29, 35, 36, 42 |
| Cohort | 6 (18) | 12, 21, 23, 37, 38, 40 |
| Quasi-experimental | 1 (3) | 20 |
| Qualitative | 10 (30) | 15, 16, 24, 30–34, 39, 41 |
| Mixed methods | 2 (6) | 25, 26 |
| Data source | ||
| Survey | 7 (21) | 12, 19, 20, 28, 29, 36, 38 |
| Registry | 10 (30) | 10, 11, 13, 14, 17, 18, 21–23, 27 |
| Interview | 4 (12) | 24, 30, 34, 41 |
| Multiple data sources | 12 (36) | 15, 16, 21, 25, 26, 31, 33, 35, 37, 38, 40, 42 |
| Adjustment for potential confounders | ||
| Yes | 17 (52) | 11, 12, 18–23, 25–29, 35–38 |
| Not defined | 16 (48) | 10, 13–17, 24, 30–34, 39–42 |
| n (%) | References | |
|---|---|---|
| General characteristics of studies | ||
| Receiving countries | ||
| Denmark | 2 (6) | 10,11 |
| France | 1 (3) | 12 |
| Germany | 4 (12) | 13–16 |
| Italy | 5 (15) | 17–21 |
| Malta | 1 (3) | 22 |
| Netherlands | 4 (12) | 23–26 |
| Portugal | 6 (18) | 27–32 |
| Spain | 2 (6) | 33,34 |
| Switzerland | 5 (15) | 35–39 |
| United Kingdom | 2 (6) | 40,41 |
| Multi-country analysis | 1 (3) | 42 |
| Geographical setting | ||
| National | 3 (9) | 20,22,41 |
| Regional or local | 30 (91) | 10–19, 21, 23–40, 42 |
| Focus of the study | ||
| Use of maternal and child healthcare services | 12 (36) | 10, 13–17, 26, 28, 29, 31, 34, 42 |
| Both use and outcomes of maternal and child healthcare | 21 (64) | 11, 12, 16, 18–21, 23–25, 27, 30, 32, 33, 35–41 |
| Characteristics of undocumented migrants | ||
| Number of undocumented migrants included | ||
| Sample less than 500 | 23 (70) | 11, 15, 16, 21–28, 30–41 |
| Sample between 500 and 1000 | 4 (12) | 10, 12, 19, 29 |
| Sample more than 1000 | 6 (18) | 13, 14, 17, 18, 20, 42 |
| Percentage of undocumented migrants in total study sample | ||
| Less than 10% | 5 (15) | 12, 18, 19, 27, 39 |
| 10–49% | 12 (36) | 20–22, 28–33, 35, 37, 38 |
| 50–99% | 4 (12) | 14, 23, 40, 42 |
| 100% | 12 (36) | 10, 11, 13, 15–17, 24–26, 34, 36, 41 |
| Information on place of birth | ||
| Specific country of birth | 4 (12) | 32–34, 39 |
| Specific region of birth | 13 (39) | 12, 14, 15, 18–21, 26, 28, 31, 35, 37, 38 |
| Both specific country and region of birth | 14 (42) | 10, 11, 13, 16, 17, 22–25, 27, 29, 30, 36, 42 |
| Not reported | 2 (6) | 40, 41 |
| Information on reason for migration | ||
| Yes | 6 (18) | 15, 24–26, 38, 39 |
| No | 27 (82) | 10–14, 16–23, 27–37, 40–42 |
| Included study participants | ||
| Only undocumented migrants | 16 (48) | 10, 11, 13–17, 20, 24–26, 34, 36, 40–42 |
| Different migrant populations | 9 (27) | 12, 19, 21, 28–30, 32, 33, 39 |
| Undocumented migrants and comparator group | 8 (24) | 18, 22, 23, 27, 31, 35, 37, 38 |
| Methodological characteristics | ||
| Study design | ||
| Quantitative | ||
| Cross-sectional | 14 (42) | 10, 11, 13, 14, 17–19, 22, 27–29, 35, 36, 42 |
| Cohort | 6 (18) | 12, 21, 23, 37, 38, 40 |
| Quasi-experimental | 1 (3) | 20 |
| Qualitative | 10 (30) | 15, 16, 24, 30–34, 39, 41 |
| Mixed methods | 2 (6) | 25, 26 |
| Data source | ||
| Survey | 7 (21) | 12, 19, 20, 28, 29, 36, 38 |
| Registry | 10 (30) | 10, 11, 13, 14, 17, 18, 21–23, 27 |
| Interview | 4 (12) | 24, 30, 34, 41 |
| Multiple data sources | 12 (36) | 15, 16, 21, 25, 26, 31, 33, 35, 37, 38, 40, 42 |
| Adjustment for potential confounders | ||
| Yes | 17 (52) | 11, 12, 18–23, 25–29, 35–38 |
| Not defined | 16 (48) | 10, 13–17, 24, 30–34, 39–42 |
Description of included studies (n = 33)
| n (%) | References | |
|---|---|---|
| General characteristics of studies | ||
| Receiving countries | ||
| Denmark | 2 (6) | 10,11 |
| France | 1 (3) | 12 |
| Germany | 4 (12) | 13–16 |
| Italy | 5 (15) | 17–21 |
| Malta | 1 (3) | 22 |
| Netherlands | 4 (12) | 23–26 |
| Portugal | 6 (18) | 27–32 |
| Spain | 2 (6) | 33,34 |
| Switzerland | 5 (15) | 35–39 |
| United Kingdom | 2 (6) | 40,41 |
| Multi-country analysis | 1 (3) | 42 |
| Geographical setting | ||
| National | 3 (9) | 20,22,41 |
| Regional or local | 30 (91) | 10–19, 21, 23–40, 42 |
| Focus of the study | ||
| Use of maternal and child healthcare services | 12 (36) | 10, 13–17, 26, 28, 29, 31, 34, 42 |
| Both use and outcomes of maternal and child healthcare | 21 (64) | 11, 12, 16, 18–21, 23–25, 27, 30, 32, 33, 35–41 |
| Characteristics of undocumented migrants | ||
| Number of undocumented migrants included | ||
| Sample less than 500 | 23 (70) | 11, 15, 16, 21–28, 30–41 |
| Sample between 500 and 1000 | 4 (12) | 10, 12, 19, 29 |
| Sample more than 1000 | 6 (18) | 13, 14, 17, 18, 20, 42 |
| Percentage of undocumented migrants in total study sample | ||
| Less than 10% | 5 (15) | 12, 18, 19, 27, 39 |
| 10–49% | 12 (36) | 20–22, 28–33, 35, 37, 38 |
| 50–99% | 4 (12) | 14, 23, 40, 42 |
| 100% | 12 (36) | 10, 11, 13, 15–17, 24–26, 34, 36, 41 |
| Information on place of birth | ||
| Specific country of birth | 4 (12) | 32–34, 39 |
| Specific region of birth | 13 (39) | 12, 14, 15, 18–21, 26, 28, 31, 35, 37, 38 |
| Both specific country and region of birth | 14 (42) | 10, 11, 13, 16, 17, 22–25, 27, 29, 30, 36, 42 |
| Not reported | 2 (6) | 40, 41 |
| Information on reason for migration | ||
| Yes | 6 (18) | 15, 24–26, 38, 39 |
| No | 27 (82) | 10–14, 16–23, 27–37, 40–42 |
| Included study participants | ||
| Only undocumented migrants | 16 (48) | 10, 11, 13–17, 20, 24–26, 34, 36, 40–42 |
| Different migrant populations | 9 (27) | 12, 19, 21, 28–30, 32, 33, 39 |
| Undocumented migrants and comparator group | 8 (24) | 18, 22, 23, 27, 31, 35, 37, 38 |
| Methodological characteristics | ||
| Study design | ||
| Quantitative | ||
| Cross-sectional | 14 (42) | 10, 11, 13, 14, 17–19, 22, 27–29, 35, 36, 42 |
| Cohort | 6 (18) | 12, 21, 23, 37, 38, 40 |
| Quasi-experimental | 1 (3) | 20 |
| Qualitative | 10 (30) | 15, 16, 24, 30–34, 39, 41 |
| Mixed methods | 2 (6) | 25, 26 |
| Data source | ||
| Survey | 7 (21) | 12, 19, 20, 28, 29, 36, 38 |
| Registry | 10 (30) | 10, 11, 13, 14, 17, 18, 21–23, 27 |
| Interview | 4 (12) | 24, 30, 34, 41 |
| Multiple data sources | 12 (36) | 15, 16, 21, 25, 26, 31, 33, 35, 37, 38, 40, 42 |
| Adjustment for potential confounders | ||
| Yes | 17 (52) | 11, 12, 18–23, 25–29, 35–38 |
| Not defined | 16 (48) | 10, 13–17, 24, 30–34, 39–42 |
| n (%) | References | |
|---|---|---|
| General characteristics of studies | ||
| Receiving countries | ||
| Denmark | 2 (6) | 10,11 |
| France | 1 (3) | 12 |
| Germany | 4 (12) | 13–16 |
| Italy | 5 (15) | 17–21 |
| Malta | 1 (3) | 22 |
| Netherlands | 4 (12) | 23–26 |
| Portugal | 6 (18) | 27–32 |
| Spain | 2 (6) | 33,34 |
| Switzerland | 5 (15) | 35–39 |
| United Kingdom | 2 (6) | 40,41 |
| Multi-country analysis | 1 (3) | 42 |
| Geographical setting | ||
| National | 3 (9) | 20,22,41 |
| Regional or local | 30 (91) | 10–19, 21, 23–40, 42 |
| Focus of the study | ||
| Use of maternal and child healthcare services | 12 (36) | 10, 13–17, 26, 28, 29, 31, 34, 42 |
| Both use and outcomes of maternal and child healthcare | 21 (64) | 11, 12, 16, 18–21, 23–25, 27, 30, 32, 33, 35–41 |
| Characteristics of undocumented migrants | ||
| Number of undocumented migrants included | ||
| Sample less than 500 | 23 (70) | 11, 15, 16, 21–28, 30–41 |
| Sample between 500 and 1000 | 4 (12) | 10, 12, 19, 29 |
| Sample more than 1000 | 6 (18) | 13, 14, 17, 18, 20, 42 |
| Percentage of undocumented migrants in total study sample | ||
| Less than 10% | 5 (15) | 12, 18, 19, 27, 39 |
| 10–49% | 12 (36) | 20–22, 28–33, 35, 37, 38 |
| 50–99% | 4 (12) | 14, 23, 40, 42 |
| 100% | 12 (36) | 10, 11, 13, 15–17, 24–26, 34, 36, 41 |
| Information on place of birth | ||
| Specific country of birth | 4 (12) | 32–34, 39 |
| Specific region of birth | 13 (39) | 12, 14, 15, 18–21, 26, 28, 31, 35, 37, 38 |
| Both specific country and region of birth | 14 (42) | 10, 11, 13, 16, 17, 22–25, 27, 29, 30, 36, 42 |
| Not reported | 2 (6) | 40, 41 |
| Information on reason for migration | ||
| Yes | 6 (18) | 15, 24–26, 38, 39 |
| No | 27 (82) | 10–14, 16–23, 27–37, 40–42 |
| Included study participants | ||
| Only undocumented migrants | 16 (48) | 10, 11, 13–17, 20, 24–26, 34, 36, 40–42 |
| Different migrant populations | 9 (27) | 12, 19, 21, 28–30, 32, 33, 39 |
| Undocumented migrants and comparator group | 8 (24) | 18, 22, 23, 27, 31, 35, 37, 38 |
| Methodological characteristics | ||
| Study design | ||
| Quantitative | ||
| Cross-sectional | 14 (42) | 10, 11, 13, 14, 17–19, 22, 27–29, 35, 36, 42 |
| Cohort | 6 (18) | 12, 21, 23, 37, 38, 40 |
| Quasi-experimental | 1 (3) | 20 |
| Qualitative | 10 (30) | 15, 16, 24, 30–34, 39, 41 |
| Mixed methods | 2 (6) | 25, 26 |
| Data source | ||
| Survey | 7 (21) | 12, 19, 20, 28, 29, 36, 38 |
| Registry | 10 (30) | 10, 11, 13, 14, 17, 18, 21–23, 27 |
| Interview | 4 (12) | 24, 30, 34, 41 |
| Multiple data sources | 12 (36) | 15, 16, 21, 25, 26, 31, 33, 35, 37, 38, 40, 42 |
| Adjustment for potential confounders | ||
| Yes | 17 (52) | 11, 12, 18–23, 25–29, 35–38 |
| Not defined | 16 (48) | 10, 13–17, 24, 30–34, 39–42 |
In total, 10 qualitative and 21 quantitative studies were included, of which cross-sectional (n = 14) and cohort (n = 6) studies were most prevalent. Seventeen of the quantitative studies adjusted for potential confounders, such as age, gender, socio-economic or marital status. The chosen data sources included registry (n = 10), survey (n = 7), interview (n = 4) and multiple sources (n = 12). With regard to multiple sources, six qualitative studies used both interviews and observations, four quantitative studies used a combination of registry and survey data, and two mixed method studies utilised face-to-face interviews and questionnaires. Regarding the topic of each study, 12 articles reported data on the utilisation of maternal and child healthcare services, while 21 articles reported data on both the use and outcomes of maternal and child healthcare. No study focused solely on the outcomes of maternal and child healthcare.
The sample size of undocumented migrants varied greatly between studies, as both qualitative and quantitative studies were included. From the 23 studies with a sample size below 500 participants, 10 had a sample size below 20, while the remaining 13 recruited a sample between 100 and 346 participants. The remaining 10 articles had a sample size of between 564 and 830 (n = 4) and between 1758 and 13 626 (n = 6). In addition to the absolute sample size of undocumented migrants, the percentage of undocumented migrants in the total sample is important, as it indicates the focus of studies. The sample of undocumented migrants in the total study population of 17 studies was below 50%, and <10% in 5 of them. For 12 studies, the percentage of the undocumented migrant sample in the overall sample was 100%. Percentages around 50% are related to the presence of a comparator group (n = 8). All studies except two mentioned a specific country (n = 4), region (n = 13) or both country and region of birth (n = 14). Only 6 of the 33 included studies mentioned the reason behind migration, such as political, economic or family-related motivations.
The main findings of the 33 included studies are presented in tables 2 and 3 and elaborated on in more detail in the following text. Some studies only generally addressed the utilisation or outcomes of maternal and child healthcare, without going into further specifics.26,28,29 These were subsequently categorised as “maternal and child healthcare” and/or “poor maternal and child health outcomes”.
Summary table—utilisation of maternal and child healthcare services
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Maternal and child healthcare | 3 | 28, 29, 40 | 1 | 26 | 4 (12) | ||
| Prenatal/antenatal care | 20 | 10–14, 17–23, 27–29, 35, 37, 38, 40, 42 | 8 | 15, 16, 30, 31, 33, 34, 39, 41 | 2 | 25, 26 | 30 (91) |
| Pregnancy screening and testing | 9 | 10, 11, 21, 23, 35, 37, 38, 40, 42 | 4 | 15, 16, 30, 31 | 1 | 25 | 14 (42) |
| Consultations | 4 | 10, 13, 14, 17 | 4 (12) | ||||
| Antepartum hospitalisation | 2 | 18, 19 | 2 (6) | ||||
| Intrapartum care | 11 | 10, 18, 19, 21–23, 27, 36–38, 40 | 6 | 15, 24, 30, 32, 33, 39 | 1 | 25 | 18 (55) |
| Childbirth/delivery | 10 | 10, 18, 19, 21–23, 27, 37, 38, 40 | 5 | 15, 30, 32, 33, 39 | 1 | 25 | 16 (49) |
| Spontaneous vaginal childbirth | 7 | 18, 22, 23, 27, 37, 38, 40 | 7 (21) | ||||
| Caesarean section | 7 | 18, 22, 23, 27, 37, 38, 40 | 2 | 15, 32 | 1 | 25 | 10 (30) |
| Instrumental vaginal childbirth | 4 | 22, 23, 37, 38 | 1 | 32 | 5 (15) | ||
| Pain relief during labour | 1 | 23 | 1 (3) | ||||
| Postnatal and postpartum care | 4 | 11, 23, 38, 40 | 1 | 33 | 5 (15) | ||
| Postpartum hospitalisation | 2 | 38, 40 | 2 (6) | ||||
| Neonatal and infant care | 3 | 10, 23, 40 | 1 | 16 | 4 (12) | ||
| Neonatal admission | 1 | 23 | 1 (3) | ||||
| Infant examination and vaccination | 1 | 10 | 1 | 16 | 2 (6) | ||
| Family planning | 3 | 35, 37, 38 | 3 | 31–33 | 1 | 25 | 7 (21) |
| Abortion | 8 | 11, 17–19, 21, 35, 36, 38 | 1 | 25 | 9 (27) | ||
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Maternal and child healthcare | 3 | 28, 29, 40 | 1 | 26 | 4 (12) | ||
| Prenatal/antenatal care | 20 | 10–14, 17–23, 27–29, 35, 37, 38, 40, 42 | 8 | 15, 16, 30, 31, 33, 34, 39, 41 | 2 | 25, 26 | 30 (91) |
| Pregnancy screening and testing | 9 | 10, 11, 21, 23, 35, 37, 38, 40, 42 | 4 | 15, 16, 30, 31 | 1 | 25 | 14 (42) |
| Consultations | 4 | 10, 13, 14, 17 | 4 (12) | ||||
| Antepartum hospitalisation | 2 | 18, 19 | 2 (6) | ||||
| Intrapartum care | 11 | 10, 18, 19, 21–23, 27, 36–38, 40 | 6 | 15, 24, 30, 32, 33, 39 | 1 | 25 | 18 (55) |
| Childbirth/delivery | 10 | 10, 18, 19, 21–23, 27, 37, 38, 40 | 5 | 15, 30, 32, 33, 39 | 1 | 25 | 16 (49) |
| Spontaneous vaginal childbirth | 7 | 18, 22, 23, 27, 37, 38, 40 | 7 (21) | ||||
| Caesarean section | 7 | 18, 22, 23, 27, 37, 38, 40 | 2 | 15, 32 | 1 | 25 | 10 (30) |
| Instrumental vaginal childbirth | 4 | 22, 23, 37, 38 | 1 | 32 | 5 (15) | ||
| Pain relief during labour | 1 | 23 | 1 (3) | ||||
| Postnatal and postpartum care | 4 | 11, 23, 38, 40 | 1 | 33 | 5 (15) | ||
| Postpartum hospitalisation | 2 | 38, 40 | 2 (6) | ||||
| Neonatal and infant care | 3 | 10, 23, 40 | 1 | 16 | 4 (12) | ||
| Neonatal admission | 1 | 23 | 1 (3) | ||||
| Infant examination and vaccination | 1 | 10 | 1 | 16 | 2 (6) | ||
| Family planning | 3 | 35, 37, 38 | 3 | 31–33 | 1 | 25 | 7 (21) |
| Abortion | 8 | 11, 17–19, 21, 35, 36, 38 | 1 | 25 | 9 (27) | ||
Summary table—utilisation of maternal and child healthcare services
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Maternal and child healthcare | 3 | 28, 29, 40 | 1 | 26 | 4 (12) | ||
| Prenatal/antenatal care | 20 | 10–14, 17–23, 27–29, 35, 37, 38, 40, 42 | 8 | 15, 16, 30, 31, 33, 34, 39, 41 | 2 | 25, 26 | 30 (91) |
| Pregnancy screening and testing | 9 | 10, 11, 21, 23, 35, 37, 38, 40, 42 | 4 | 15, 16, 30, 31 | 1 | 25 | 14 (42) |
| Consultations | 4 | 10, 13, 14, 17 | 4 (12) | ||||
| Antepartum hospitalisation | 2 | 18, 19 | 2 (6) | ||||
| Intrapartum care | 11 | 10, 18, 19, 21–23, 27, 36–38, 40 | 6 | 15, 24, 30, 32, 33, 39 | 1 | 25 | 18 (55) |
| Childbirth/delivery | 10 | 10, 18, 19, 21–23, 27, 37, 38, 40 | 5 | 15, 30, 32, 33, 39 | 1 | 25 | 16 (49) |
| Spontaneous vaginal childbirth | 7 | 18, 22, 23, 27, 37, 38, 40 | 7 (21) | ||||
| Caesarean section | 7 | 18, 22, 23, 27, 37, 38, 40 | 2 | 15, 32 | 1 | 25 | 10 (30) |
| Instrumental vaginal childbirth | 4 | 22, 23, 37, 38 | 1 | 32 | 5 (15) | ||
| Pain relief during labour | 1 | 23 | 1 (3) | ||||
| Postnatal and postpartum care | 4 | 11, 23, 38, 40 | 1 | 33 | 5 (15) | ||
| Postpartum hospitalisation | 2 | 38, 40 | 2 (6) | ||||
| Neonatal and infant care | 3 | 10, 23, 40 | 1 | 16 | 4 (12) | ||
| Neonatal admission | 1 | 23 | 1 (3) | ||||
| Infant examination and vaccination | 1 | 10 | 1 | 16 | 2 (6) | ||
| Family planning | 3 | 35, 37, 38 | 3 | 31–33 | 1 | 25 | 7 (21) |
| Abortion | 8 | 11, 17–19, 21, 35, 36, 38 | 1 | 25 | 9 (27) | ||
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Maternal and child healthcare | 3 | 28, 29, 40 | 1 | 26 | 4 (12) | ||
| Prenatal/antenatal care | 20 | 10–14, 17–23, 27–29, 35, 37, 38, 40, 42 | 8 | 15, 16, 30, 31, 33, 34, 39, 41 | 2 | 25, 26 | 30 (91) |
| Pregnancy screening and testing | 9 | 10, 11, 21, 23, 35, 37, 38, 40, 42 | 4 | 15, 16, 30, 31 | 1 | 25 | 14 (42) |
| Consultations | 4 | 10, 13, 14, 17 | 4 (12) | ||||
| Antepartum hospitalisation | 2 | 18, 19 | 2 (6) | ||||
| Intrapartum care | 11 | 10, 18, 19, 21–23, 27, 36–38, 40 | 6 | 15, 24, 30, 32, 33, 39 | 1 | 25 | 18 (55) |
| Childbirth/delivery | 10 | 10, 18, 19, 21–23, 27, 37, 38, 40 | 5 | 15, 30, 32, 33, 39 | 1 | 25 | 16 (49) |
| Spontaneous vaginal childbirth | 7 | 18, 22, 23, 27, 37, 38, 40 | 7 (21) | ||||
| Caesarean section | 7 | 18, 22, 23, 27, 37, 38, 40 | 2 | 15, 32 | 1 | 25 | 10 (30) |
| Instrumental vaginal childbirth | 4 | 22, 23, 37, 38 | 1 | 32 | 5 (15) | ||
| Pain relief during labour | 1 | 23 | 1 (3) | ||||
| Postnatal and postpartum care | 4 | 11, 23, 38, 40 | 1 | 33 | 5 (15) | ||
| Postpartum hospitalisation | 2 | 38, 40 | 2 (6) | ||||
| Neonatal and infant care | 3 | 10, 23, 40 | 1 | 16 | 4 (12) | ||
| Neonatal admission | 1 | 23 | 1 (3) | ||||
| Infant examination and vaccination | 1 | 10 | 1 | 16 | 2 (6) | ||
| Family planning | 3 | 35, 37, 38 | 3 | 31–33 | 1 | 25 | 7 (21) |
| Abortion | 8 | 11, 17–19, 21, 35, 36, 38 | 1 | 25 | 9 (27) | ||
Summary table—maternal and child health outcomes
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Poor maternal and pregnancy outcomes | 3 | 23, 35, 40 | 1 | 32 | 4 (12) | ||
| Antenatal outcomes | 10 | 11, 18, 19, 22, 23, 27, 36–38, 40 | 5 | 24, 30, 32, 39, 41 | 1 | 25 | 16 (49) |
| Previous adverse obstetric outcomes | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Miscarriage | 3 | 18, 19, 27 | 3 (9) | ||||
| STIs | 5 | 11, 22, 23, 36, 37 | 2 | 24, 32 | 1 | 25 | 8 (24) |
| Other antenatal problems | 5 | 23, 27, 36, 38, 40 | 5 | 24, 30, 32, 39, 41 | 10 (30) | ||
| Intrapartum outcomes | 7 | 19, 21–23, 27, 38, 40 | 4 | 24, 30, 32, 39 | 1 | 25 | 12 (36) |
| Gestational age at childbirth | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Pre-term | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Post-term | 4 | 22, 27, 38, 40 | 4 (12) | ||||
| Neonatal complications during labour | 4 | 19, 23, 27, 38 | 1 | 24 | 5 (15) | ||
| Maternal complications during labour | 5 | 19, 23, 27, 38, 40 | 2 | 24, 30 | 7 (21) | ||
| Postnatal and postpartum outcomes | 4 | 27, 35, 38, 40 | 2 | 30, 32 | 6 (18) | ||
| Postpartum haemorrhage | 1 | 27 | 1 (3) | ||||
| Postpartum depression | 1 | 27 | 2 | 30, 32 | 3 (9) | ||
| Other postnatal problems | 2 | 38, 40 | 1 | 32 | 3 (9) | ||
| Neonatal and infant outcomes | 8 | 12, 20–23, 27, 38, 40 | 4 | 24, 30, 39, 41 | 1 | 25 | 13 (39) |
| Low birth weight | 6 | 20, 22, 23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Birth malformations | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Perinatal mortality | 5 | 21–23, 27, 40 | 1 | 30 | 6 (18) | ||
| Infant mortality | 1 | 22 | 1 | 41 | 2 (6) | ||
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Poor maternal and pregnancy outcomes | 3 | 23, 35, 40 | 1 | 32 | 4 (12) | ||
| Antenatal outcomes | 10 | 11, 18, 19, 22, 23, 27, 36–38, 40 | 5 | 24, 30, 32, 39, 41 | 1 | 25 | 16 (49) |
| Previous adverse obstetric outcomes | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Miscarriage | 3 | 18, 19, 27 | 3 (9) | ||||
| STIs | 5 | 11, 22, 23, 36, 37 | 2 | 24, 32 | 1 | 25 | 8 (24) |
| Other antenatal problems | 5 | 23, 27, 36, 38, 40 | 5 | 24, 30, 32, 39, 41 | 10 (30) | ||
| Intrapartum outcomes | 7 | 19, 21–23, 27, 38, 40 | 4 | 24, 30, 32, 39 | 1 | 25 | 12 (36) |
| Gestational age at childbirth | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Pre-term | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Post-term | 4 | 22, 27, 38, 40 | 4 (12) | ||||
| Neonatal complications during labour | 4 | 19, 23, 27, 38 | 1 | 24 | 5 (15) | ||
| Maternal complications during labour | 5 | 19, 23, 27, 38, 40 | 2 | 24, 30 | 7 (21) | ||
| Postnatal and postpartum outcomes | 4 | 27, 35, 38, 40 | 2 | 30, 32 | 6 (18) | ||
| Postpartum haemorrhage | 1 | 27 | 1 (3) | ||||
| Postpartum depression | 1 | 27 | 2 | 30, 32 | 3 (9) | ||
| Other postnatal problems | 2 | 38, 40 | 1 | 32 | 3 (9) | ||
| Neonatal and infant outcomes | 8 | 12, 20–23, 27, 38, 40 | 4 | 24, 30, 39, 41 | 1 | 25 | 13 (39) |
| Low birth weight | 6 | 20, 22, 23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Birth malformations | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Perinatal mortality | 5 | 21–23, 27, 40 | 1 | 30 | 6 (18) | ||
| Infant mortality | 1 | 22 | 1 | 41 | 2 (6) | ||
Summary table—maternal and child health outcomes
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Poor maternal and pregnancy outcomes | 3 | 23, 35, 40 | 1 | 32 | 4 (12) | ||
| Antenatal outcomes | 10 | 11, 18, 19, 22, 23, 27, 36–38, 40 | 5 | 24, 30, 32, 39, 41 | 1 | 25 | 16 (49) |
| Previous adverse obstetric outcomes | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Miscarriage | 3 | 18, 19, 27 | 3 (9) | ||||
| STIs | 5 | 11, 22, 23, 36, 37 | 2 | 24, 32 | 1 | 25 | 8 (24) |
| Other antenatal problems | 5 | 23, 27, 36, 38, 40 | 5 | 24, 30, 32, 39, 41 | 10 (30) | ||
| Intrapartum outcomes | 7 | 19, 21–23, 27, 38, 40 | 4 | 24, 30, 32, 39 | 1 | 25 | 12 (36) |
| Gestational age at childbirth | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Pre-term | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Post-term | 4 | 22, 27, 38, 40 | 4 (12) | ||||
| Neonatal complications during labour | 4 | 19, 23, 27, 38 | 1 | 24 | 5 (15) | ||
| Maternal complications during labour | 5 | 19, 23, 27, 38, 40 | 2 | 24, 30 | 7 (21) | ||
| Postnatal and postpartum outcomes | 4 | 27, 35, 38, 40 | 2 | 30, 32 | 6 (18) | ||
| Postpartum haemorrhage | 1 | 27 | 1 (3) | ||||
| Postpartum depression | 1 | 27 | 2 | 30, 32 | 3 (9) | ||
| Other postnatal problems | 2 | 38, 40 | 1 | 32 | 3 (9) | ||
| Neonatal and infant outcomes | 8 | 12, 20–23, 27, 38, 40 | 4 | 24, 30, 39, 41 | 1 | 25 | 13 (39) |
| Low birth weight | 6 | 20, 22, 23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Birth malformations | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Perinatal mortality | 5 | 21–23, 27, 40 | 1 | 30 | 6 (18) | ||
| Infant mortality | 1 | 22 | 1 | 41 | 2 (6) | ||
| Quantitative (n = 21) | Qualitative (n = 10) | Mixed methods (n = 2) | Total (n = 33) | ||||
|---|---|---|---|---|---|---|---|
| n | References | n | References | n | References | n (%) | |
| Poor maternal and pregnancy outcomes | 3 | 23, 35, 40 | 1 | 32 | 4 (12) | ||
| Antenatal outcomes | 10 | 11, 18, 19, 22, 23, 27, 36–38, 40 | 5 | 24, 30, 32, 39, 41 | 1 | 25 | 16 (49) |
| Previous adverse obstetric outcomes | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Miscarriage | 3 | 18, 19, 27 | 3 (9) | ||||
| STIs | 5 | 11, 22, 23, 36, 37 | 2 | 24, 32 | 1 | 25 | 8 (24) |
| Other antenatal problems | 5 | 23, 27, 36, 38, 40 | 5 | 24, 30, 32, 39, 41 | 10 (30) | ||
| Intrapartum outcomes | 7 | 19, 21–23, 27, 38, 40 | 4 | 24, 30, 32, 39 | 1 | 25 | 12 (36) |
| Gestational age at childbirth | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Pre-term | 6 | 21–23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Post-term | 4 | 22, 27, 38, 40 | 4 (12) | ||||
| Neonatal complications during labour | 4 | 19, 23, 27, 38 | 1 | 24 | 5 (15) | ||
| Maternal complications during labour | 5 | 19, 23, 27, 38, 40 | 2 | 24, 30 | 7 (21) | ||
| Postnatal and postpartum outcomes | 4 | 27, 35, 38, 40 | 2 | 30, 32 | 6 (18) | ||
| Postpartum haemorrhage | 1 | 27 | 1 (3) | ||||
| Postpartum depression | 1 | 27 | 2 | 30, 32 | 3 (9) | ||
| Other postnatal problems | 2 | 38, 40 | 1 | 32 | 3 (9) | ||
| Neonatal and infant outcomes | 8 | 12, 20–23, 27, 38, 40 | 4 | 24, 30, 39, 41 | 1 | 25 | 13 (39) |
| Low birth weight | 6 | 20, 22, 23, 27, 38, 40 | 2 | 24, 39 | 1 | 25 | 9 (27) |
| Birth malformations | 2 | 22, 27 | 1 | 24 | 3 (9) | ||
| Perinatal mortality | 5 | 21–23, 27, 40 | 1 | 30 | 6 (18) | ||
| Infant mortality | 1 | 22 | 1 | 41 | 2 (6) | ||
Prenatal care and outcomes
Prenatal or antenatal care describes care provided to the pregnant woman and her unborn foetus during pregnancy. The large majority (91%) of included studies assessed prenatal or antenatal care utilisation of undocumented migrants. More precisely, most studies (63%) observed infrequent, late or no use of prenatal care by undocumented women. For example, when compared with documented migrants in the Netherlands, undocumented women came on average five weeks later to their first antenatal appointment and attended three fewer prenatal care visits in total.23 The risk for delayed prenatal care utilisation of undocumented women in Switzerland was found to be up to 11 times higher than a control group of pregnant women with legal residency.37,38 The most prevalent reasons for prenatal visits among undocumented migrants were regular pregnancy screenings, ultrasounds and laboratory tests. One study in Denmark compared the number and results of HIV, HBV and Syphilis screening tests between undocumented and documented women and found significant differences.11 Documented migrants in Denmark utilised the routine pregnancy screenings in 99.8% of all cases, compared with only between 43 and 60% of undocumented cases.11 One explanation given for this difference is that undocumented migrants faced formal and informal barriers to accessing maternal and child healthcare in Denmark at the time of the study, such as restrictive legal entitlements and fear of being handed over to the authorities.11 Significant underuse of preventive pregnancy screening in undocumented migrants compared with legal residents was also found in Switzerland and the Netherlands.25,38
Almost half of the studies assessing the utilisation of prenatal care also presented data on the main antenatal outcomes experienced by undocumented women. Antenatal problems such as anaemia, gestational diabetes, hypertension and preeclampsia were found the most prevalent issues during pregnancy among undocumented migrants.4,22–24,27,37,38 However, in a Swiss study, when compared with a native control group, undocumented women did not have significantly higher rates of antenatal problems.38 Half of the qualitative studies provided in-depth insights into pregnancy issues experienced by the interviewed undocumented women, of which anaemia, hypertension and Hepatitis B were mentioned most often.24,30,39 In several quantitative studies, the incidence of sexually transmitted infections (STIs) was found up to three times higher in undocumented migrants than in documented migrants.11,37
Intrapartum care and outcomes
Intrapartum care refers to the period of care provided during childbirth. Of the different childbirth modes, spontaneous vaginal birth (n = 7) and caesarean section (n = 10) were mentioned most frequently. Nevertheless, several studies did not specify the type of childbirth when presenting data on the childbirth of undocumented women.10,19,21 In a study conducted in Malta, irregular migrants from the Sub-Saharan region in Africa were found to be statistically less likely to have a planned childbirth, meaning an elective or induced caesarean section, and more likely to have an emergency C-section compared with documented migrants and the overall Maltese population.22 In qualitative interviews with undocumented migrants of Brazilian origin in Spain, one participant reported that the health professional was largely not available during her childbirth.32 Other qualitative studies (in Germany and Switzerland) found that many undocumented women feared utilising intrapartum care, even during contractions, afraid of getting deported.15,39 In two German studies, the study participants reported that the increased visibility that a temporary residence permit called “Duldung” provides, only increased their fear of deportation, outweighing the benefits of free maternal and child healthcare access.15,16 Lower utilisation of medication to relieve pain was found in undocumented women in the Netherlands when compared with documented migrants, although the difference was not statistically significant.23
Approximately two-thirds of the studies reporting on the use of intrapartum care also assessed the main intrapartum outcomes and complications. Findings on the incidence of pre-term birth are mixed. While one study in Portugal found no significant differences in pre-term childbirth between migrant and Portuguese women,27 other studies, in the Netherlands and Italy, found significantly higher rates of pre-term deliveries in undocumented women compared with documented and non-migrant women.21,23 Similarly, a study in Switzerland found higher, but not significantly different, rates of pre-term childbirth in undocumented compared with documented migrants.38 Studies with the presence of a comparison group did not find statistically significant differences in neonatal or maternal complications during labour, such as vaginal tear, retention of the placenta or foetal distress.23,27,38 Nevertheless, qualitative insights of several studies in the Netherlands, the United Kingdom and Portugal indicate that undocumented migrants experienced complications such as foetal distress, birth trauma and pre-term delivery during childbirth.24,30,32,41
Postnatal and postpartum care and outcomes
Postnatal care refers to the care provided to the mother and her newborn after childbirth, while the postpartum period only refers to the stage of caregiving after complete childbirth to 42 days after childbirth. Only 15–18% of all 33 studies referred to the postnatal or postpartum period. One study in the United Kingdom reported that 68.57% of study participants were hospitalised longer than expected after childbirth.40 The most prevalent reasons for this were post-caesarean section recovery, excessive blood loss during childbirth or maternal high blood pressure.40 Postpartum depression or haemorrhage was reported most often as postnatal outcomes. Several undocumented migrants in Portugal reported having experienced postpartum depression after childbirth.27,30,32 In a comparative study of migrant and Portuguese women, a higher incidence of postpartum haemorrhage was found in undocumented women.27
Neonatal and infant care and outcomes
The care provided to the newborn after childbirth is strictly speaking part of postnatal care, but discussed here separately to showcase more differentiated outcomes. Generally, most studies focused primarily on maternal care, with only 12% also specifically reporting neonatal or infant care. Two studies in Denmark and Germany reported utilisation of infant examination and vaccination.10,16 In Denmark, such utilisation was reported to be very low, suggesting that only very few undocumented women return for infant care after childbirth.10 A comparative study in the Netherlands found that more babies of undocumented women were admitted during the neonatal period, primarily for prematurity.23
Almost 40% of all 33 studies reported neonatal or infant outcomes, of which low birth weight and perinatal mortality were most prevalent. The findings on low birth weight were mixed. The majority of studies found a higher risk and incidence of low birth weight in infants born to undocumented migrants.20,22–25,38–40 Of these, two studies in Malta and Italy found a statistically significant difference in low birth weight in undocumented migrants compared with documented migrants20,22 and one study in the United Kingdom found a 45% higher risk of low birth weight in undocumented migrants.40. In addition, a study in Italy found a significant association between low birth weight and inadequate prenatal care use in undocumented migrants.20 Only one study, in Portugal, found no statistically significant differences in low birth weight between undocumented migrant and Portuguese women.27 No statistically significant differences in foetal malformations were found between undocumented and documented migrants in Malta and Portugal.22,27
Perinatal mortality includes both stillbirth and early neonatal mortality. Some studies in the Netherlands, United Kingdom and Malta reported a higher incidence of perinatal death in undocumented migrants compared with documented migrants, although there was no statistical significance.22,23,40
Family planning and abortion
Several studies identified family planning services as a way for women to be in control of their pregnancy. Studies conducted in Portugal, Spain and Switzerland all found limited utilisation of family planning services by undocumented migrants and a lack of awareness of contraceptive methods.31–33,37 Some studies linked the lacking utilisation of preventive services, as well as poor access to prenatal care, to a higher incidence of unintended pregnancies.33,35,36 High rates of unintended pregnancy in undocumented migrants were found in both Switzerland and Spain, ranging from 40 to 75% of included participants.33,36,38 When compared with documented migrants, two studies in Switzerland found a statistically significant association between undocumented status and unintended pregnancy, after adjusting for potential confounders.35,38 Unintended pregnancy was in turn linked to poor maternal and child health outcomes in undocumented migrants.35 Twenty-seven per cent of all 33 studies reported large proportions of undocumented migrants having planned abortions, resulting from high levels of unplanned pregnancies.11,17–19,21,25
Results of the quality assessment
For quantitative studies, the Quality Assessment Tool for Observational and Cross-sectional Studies was used.9 The tool encompasses 14 questions, with ratings of ‘good’, ‘fair’ or ‘poor’. For qualitative studies, the 10-item questionnaire Critical Appraisal Skills Programme8 was utilised and the same rating was performed to ensure comparability. In the case of mixed method studies, both tools were applied. Potential risks of bias were judged and taken into consideration in the overall quality assessment of the study. In total, only seven studies were deemed to have a ‘fair’ quality, while the remaining studies achieved a ‘good’ score. The seven studies rated as ‘fair’ failed to provide sufficient information on several checklist items, such as exposure measurements and adjustment for potential confounders, thus making it impossible to judge the quality of these items. In addition, if the risk of selection and information bias was ranked too high without any attempts to reduce or control for these types of bias, the study was ranked ‘fair’. A study was rated as ‘good’ when clear descriptions of study aim, research approach and analysis were provided. Sufficient information for each quality question was necessary to warrant a ‘good’ ranking. Despite varying quality, all 33 studies were deemed eligible for inclusion in the systematic literature review.
Discussion
To our knowledge, this study is the first to systematically review the available academic literature on the use and outcomes of maternal and child healthcare services by undocumented migrants in Europe. Our review found that the majority of included studies reported a lower utilisation and worse maternal and child health outcomes of undocumented migrants. The strength and meaningfulness of the findings of the 33 included studies, however, differ substantially, due to variations in study design, sampling procedures and sample size, as well as contextual differences. Of the included studies, only eight compared undocumented migrants with documented migrants or the general population as a reference group for the findings on undocumented women. The sample size of studies also varied greatly, with two quantitative studies having sample sizes below 20 and others as large as 13 626. The results of the qualitative studies provided in-depth insights into the experiences of undocumented women.
All of the 33 included studies reported findings on the utilisation of maternal and child healthcare services by undocumented migrants. Overall, studies found that undocumented women tend to underutilise available healthcare services. The clearest picture can be seen for prenatal care, assessed by 91% of the studies, of which 63% reported late, infrequent or no use of prenatal care during a woman’s pregnancy. We can link the findings on maternal and child healthcare utilisation to available access to such services, which is supported by the wider literature.1,43,44 Despite the EU governing principle of universal healthcare coverage for all, the reality for undocumented migrants in Europe varies greatly.1,44 Specific maternal and child healthcare entitlements are largely decided at the national level, resulting in vast differences between countries.1,44 The most recent Migrant Integration Policy Index measured the extent to which health policies integrate groups such as undocumented migrants.45 From the 10 countries included in our review, France, Portugal, Spain, Switzerland, Italy and the Netherlands provide full coverage and access to maternal and child healthcare to undocumented migrants.45,46 In contrast, undocumented migrants in the United Kingdom have to pay for maternal and child healthcare47 and in Germany undocumented women are only legally entitled to access care after a successful application for a temporary residence permit, also known as “Duldung”.45,46 In Denmark and Malta, undocumented migrants are entitled to healthcare in emergency situations and thus often face barriers in accessing maternal and child healthcare.45,46 It needs to be noted here that such entitlements are often shifting and complex in each country. Not only legal entitlements, but also the willingness to provide services and knowledge by healthcare professionals influences access to care by undocumented migrants.46 For instance, while in the United Kingdom and Germany, healthcare providers are required to report undocumented women to authorities, this is strictly forbidden in Denmark, France, Italy, Spain, Switzerland and the Netherlands. However, in Germany, there is even a possibility of legal sanctions for providing care to undocumented migrants.45
Nevertheless, even with free access to care for pregnant women and their newborns in countries such as Portugal, undocumented women still underutilised available prenatal and intrapartum care services and were more likely to have pregnancy complications.27,28 The underutilisation of accessible services could be explained by the finding that undocumented migrants often tend to only use healthcare services when severely ill, due to a lack of information and fear of being deported.43 Several studies included in our systematic review corroborate this observation, noting that fear of deportation was the primary reason for undocumented migrants to seek maternal and child healthcare services later and less frequently than recommended by national guidelines.16,24,33,39 A general lack of knowledge and awareness about legal entitlements and the availability of services were also found to result in under-utilizing maternal and child healthcare services during pregnancy, childbirth and the postpartum period.27,33,35,39 PICUM points out that undocumented migrants often think medical centres and hospitals will immediately inform the police of their presence.43 Such concerns were indeed found in studies in Switzerland and Germany.15,16,39
Twenty-one of the 33 studies assessed not only the use, but also the outcomes of maternal and child healthcare services. They generally found an increased incidence of pregnancy complications in undocumented migrants. Although not always linked, underutilising maternal and child healthcare services was found to lead to poor maternal and child health outcomes in studies conducted in Spain, Switzerland, Portugal and the Netherlands.26,28,29,33,35,36 Within the 13 studies assessing neonatal and infant outcomes, mixed results were found for preterm childbirth and low birth weight. In the wider literature, migrant status has been linked to a higher risk of low birth weight, which has been connected to preterm childbirth.1 A higher risk of preterm childbirth and low birth weight was indeed found in the included studies conducted in Switzerland, Italy, Malta, the United Kingdom and the Netherlands.20–25,38–40 One exception is a study conducted in Portugal that found a lower risk of preterm childbirth and a higher, but not statistically significant, risk of low birth weight for undocumented migrants.27 While studies rarely provided a stratified overview of utilisation or outcomes based on country or region of origin, in one study conducted in Malta, irregular migrants from the Sub-Saharan region of Africa were more likely to report perinatal loss, antenatal complications, low birth weight and prematurity.22 Another study, conducted in Italy, also found migrants from Africa to be at an increased risk of preterm childbirth.21
Relevance of findings
Compared with the most recent reviews on migrants’ use of maternal healthcare, this systematic review is the first to focus on the group of undocumented migrants. Previous reviews published on maternal health and specifically prenatal care in 2013 did not focus on Europe and only had 1 of 30 studies that included undocumented migrants in the study population.4,48 The most recent systematic review published in 2016 included irregular migrants as one target group among many.6 Findings indicated that documented migrants tend to underutilise available services and seek healthcare later than recommended when compared with the general population.4,48 Similar results have been found in the literature included in this systematic review, with the exception that already existing risks for documented migrants seem to be exacerbated in undocumented migrants. As an example, a significant reduction in low birth weight has been found in Italy after the new immigration law regularised the majority of undocumented migrants.19 In the available literature, undocumented migrants are singled out as a particularly vulnerable group, and pregnant women and their newborns are especially at risk of ill-heath and underutilising essential healthcare services.1,4,43,44,48 Due to difficulties in recruiting undocumented migrants and the therefore underrepresented sample, the findings likely underestimate the true effect an undocumented status has on utilisation and outcomes of maternal and child healthcare utilisation.18,23,27
Limitations of included studies
One limitation of several included studies is their small sample size. While qualitative studies tend to have a small sample size to be able to gain a deeper understanding of the study phenomenon, 7 of the 10 studies included in our review had a sample size of <20. These studies can still provide rich descriptions of individual cases but it may be difficult to make generalisations. The sample size of 7 quantitative studies was below 200, which limits their statistical power compared with other much bigger samples. The high diversity in sample size limits the comparability between studies in this systematic review.
Undocumented migrants have been described by many as a ‘hidden’ population,16 making it extremely difficult to recruit representative samples. Thus, the majority of studies made use of snowball or purposive sampling, which increases the risk for selection bias, although there were also 14 studies using a cross-sectional design. Not all of the included quantitative studies adjusted for the potential influence of confounders through statistical control or matching. Finally, methodological differences in the definition of undocumented migrants and the use of control groups further limit comparability between studies.
Limitations of the search strategy
One limitation of the search strategy used was to exclude studies not published in English, German or Dutch. Therefore, studies published in other languages might have been missed. Our research was limited to studies published after 2007, potentially excluding important findings published before that year. We considered only utilisation and outcomes of maternal and child healthcare, potentially neglecting associations with access to or quality of care. Furthermore, no grey literature was searched, which might have yielded additional results.
Conclusion
This systematic review presents the findings of quantitative, qualitative and mixed methods studies concerning the use and outcomes of maternal and child healthcare by undocumented migrants in Europe. Eligible studies were found from only 10 EU or EFTA countries, making a European comparison impossible. Additionally, significant methodological differences in study design, sample size and quality imply that conclusions need to be drawn with extreme caution. Nevertheless, the findings indicate that undocumented women tend to underutilise available maternal and child healthcare services and often experience worse health outcomes. Lack of knowledge and fear of deportation acted as the primary barriers for undocumented migrants to use accessible services. However, healthcare professionals also often lack the necessary knowledge concerning legal entitlements for undocumented women. The divide between access to and use of maternal and child healthcare services has serious implications for the health of undocumented migrants. Further research is needed with greater samples of undocumented migrants, ideally with control groups, in order to study differences in utilisation and outcomes of maternal and child healthcare services in greater depth. Additionally, further research is needed on the links between the use of maternal and child healthcare and existing barriers to access, such as the vastly differing entitlements of undocumented migrants to accessing essential health services.
Acknowledgements
We gratefully acknowledge the Maastricht University travel grant and the help of the London School of Hygiene and Tropical Medicine library services.
Funding
This work was supported by a Maastricht University travel grant to the lead author.
Supplementary data
Supplementary data are available at EURPUB online.
Conflicts of interest: None declared.
Key points
This study is the first systematic review on the use and outcomes of maternal and child healthcare services by undocumented migrants in Europe.
The 33 included studies indicate that undocumented migrants tend to underutilise maternal and child healthcare services and have an increased risk of pregnancy complications as well as poor maternal and child health outcomes.
The findings imply that public health professionals need to work together with policy-makers to better tailor health systems to the needs of undocumented migrants and to reduce health inequities.

{kind=link}
Comments