




Abstract
Although research on Health Behavior Theory (HBT) is being conducted at a rapid pace, the extent to which the field is truly moving forward in understanding health behavior has been questioned. This issue is examined in the current article. First, we discuss the problems within the HBT literature. Second, we discuss the proliferation of HBT and why theory comparison is essential to this area of research. Finally, we reflect on ways that the field might move forward by suggesting a new agenda for HBT research. It is argued that increased recognition of the similarity of health behavior constructs as well as increased empirical comparisons of theories are essential for true scientific progress in this line of inquiry.
Introduction
It is the goal of many researchers interested in health behavior to understand both the determinants of health behaviors and the process of health behavior change. One key route to an understanding of health behavior has been the development and empirical testing of Health Behavior Theory (HBT). Research in this area has implications including (1) a better understanding of health behavior, and (2) a basis upon which interventions to improve the public health of individuals and communities can be developed and evaluated.
Although research in this area continues at a rapid pace (Norman and Conner, 1996; Glanz et al., 1997b, 2002; Fisher and Fisher, 2000; DiClemente et al., 2002), the extent to which the field is truly moving forward has been questioned [e.g. (Weinstein, 1993; Zimmerman and Vernberg, 1994; Bandura, 1998; Smedslund, 2000a,b; Noar et al., 2003; Ogden, 2003)]. That is, because we are conducting more research on health behaviors does not necessarily mean that we are adding substantive cumulative knowledge to this area of research. Approximately 10 years ago Neil Weinstein (Weinstein, 1993) quite clearly articulated the problems in this area of research and suggested some potential solutions. Weinstein made the case that we may not be moving forward toward a better understanding of health behavior because of a lack of empirical comparisons between the numerous HBTs that exist. He stated [(Weinstein, 1993), p. 324]:
Not only did Weinstein challenge researchers to carry out more empirical comparisons of such theories, but he laid out guidelines for how one might design studies to do just that. Other researchers have echoed such sentiments for theory comparison research [e.g. (Zimmerman and Vernberg, 1994; Murray-Johnson et al., 2001; Nigg et al., 2002a; Noar et al., 2003)].…despite a large empirical literature, there is still no consensus that certain models of health behavior are more accurate than others, that certain variables are more influential than others, or that certain behaviors or situations are understood better than others. In general, researchers have failed to carry out the winnowing process that is necessary for scientific progress.
However, it is not clear whether anything has changed since Weinstein's (Weinstein, 1993) article. This leads us to ask the question: what is the best way for the field to move forward? The overriding purpose of the current article is to offer a critique of the current direction of HBT research and to suggest a new agenda of research in this area. We move to accomplish this task in three parts. First, we discuss in detail the problems within this area of research and how these problems may lead to fragmentation rather than cumulative knowledge. Second, we discuss the proliferation of HBT and why theory comparison is essential to this area of research. Finally, we reflect on ways that the field might move forward, including specific suggestions for new studies to be undertaken. It is not the purpose of the current article to review all the available evidence regarding what HBTs are most accurate in explaining health behavior. Rather, the purpose is to continue and extend a dialogue on the direction this field might move in—one that has been the topic of articles by theorists in the area [see, e.g. (Cummings et al., 1980; Bandura, 1998; Rosenstock et al., 1988), as well as recent special issues of Health Education Research (Connelly, 2002; Glasgow et al., 2002; Nigg et al., 2002b) and Journal of Health Psychology (Glanz and Maddock, 2000; Smedslund, 2000a,b).
What is theory in the first place?
A theory has been defined as [(Glanz et al., 1997a), p. 21]:
Thus, according to this definition, HBT should describe (1) what variables are most important and (2) how the variables relate or interact, and perhaps HBT should explain differences across situations, contexts, populations and with regard to different behaviors.A set of interrelated concepts, definitions, and propositions that presents a systematic view of events or situations by specifying relations among variables in order to explain and predict events or situations.
Within the study of health behavior, theories have been proposed at a variety of levels, including the individual, interpersonal, group, organizational and community levels. Further, theories vary in their focus on individual as compared to environmental determinants of behavior and cognitive as compared to affective determinants (Glanz et al., 1997b; Crosby et al., 2002). The primary focus of HBT has been at the individual level [see (Crosby et al., 2002)] and thus this article focuses on individual-level HBTs.
Kegler et al. (Kegler et al., 2002) describe a number of ways in which theories are developed, including refining existing theories (e.g. adding new constructs, making theory more parsimonious) as well as formalizing practitioner-based approaches into theory. In addition, Crosby et al. (Crosby et al., 2002) describe a trajectory of how theories are developed, modified, and discarded. They state [(Crosby et al., 2002), p. 5]:
Although these may be ideal ways to develop, modify and discard theory, it is not clear that the literature has always followed such systematic methods. Specifically, it is not clear that significant modification of theories takes place very often and we would argue that rarely, if ever, are theories completely discarded. In fact, a recent study found that many HBTs are not falsifiable according to the field's current standards for testing such theories [see (Ogden, 2003)]. Further, when new theories are introduced, it is not always clear why. That is, new theories are often introduced to explain health phenomena when it is not clear that existing theories are inadequate for explaining such phenomena.Theory development is a dynamic process…as theories become less useful…they are modified or even discarded… As new theories are synthesized and embraced, they too are subject to empirical validation, and if they are found lacking, they are similarly discarded.
The problem: numerous theories, little consensus
Numerous individual-level HBTs exist in the literature. These include the Health Belief Model [HBM (Becker, 1974)], Theory of Reasoned Action [TRA (Ajzen and Fishbein, 1980)] and Theory of Planned Behavior [TPB (Ajzen and Madden, 1986)], Social Cognitive Theory [SCT (Bandura, 1986)], and the Transtheoretical Model [TTM (Prochaska and DiClemente, 1983)]. There are models specific to behavioral areas such as safer sex (Catania et al., 1990; Fisher and Fisher, 1992) and alcohol use (Werch et al., 2000; Jones et al., 2001). Further, Fishbein (Fishbein, 2000) has proposed an integrated theory that combines concepts from several existing theories. In sum, there seems to be no lack of HBTs in the literature [also see (Glanz et al., 1997b, 2002; DiClemente et al., 2002)].
Which of the many theories that exist is most precise in explaining health-related behavior? Glanz et al. (Glanz et al., 1997a) found in their review of the literature that the HBM, TRA/TPB, SCT and TTM were among the most widely used theories in the literature. Is one of these theories ‘best’ in terms of explaining health behavior? Reviews and meta-analyses of the HBM (Becker, 1974; Janz and Becker, 1984; Harrison et al., 1992), TRA and TPB (Ajzen and Fishbein, 1980; Godin and Kok, 1996; Hausenblaus et al., 1997; Albarracin et al., 2001; Hagger et al., 2002), SCT (Bandura, 1986, 1998; Strecher et al., 1986), and TTM (Prochaska et al., 1992, 1994; Rosen, 2000; Burkholder and Evers, 2002; Spencer et al., 2002) all demonstrate support for their respective theories. Given this apparent parity in the literature, how do we move toward a better understanding of health behavior? How are researchers supposed to choose the most precise and fruitful theory or theories to apply in their studies? The recent Special Issue of Health Education Research highlighted 15 health intervention research projects, and in the articles each researcher was asked to describe how and why a certain theory was chosen to guide one's particular health intervention (Nigg et al., 2002b). Various reasons were offered, although empirical studies showing the superiority of the chosen theory over other theories was rarely among the reasons.
Problems resulting from a lack of consensus
In addition, each of these theories can be viewed as producing ‘mini-literatures’, where knowledge accumulates with regard to theories on parallel tracks that inform a particular theory but offer little contribution to cumulative knowledge across theories. This creates several related problems.
First, as Weinstein (Weinstein, 1993) and others have discussed [e.g. (Norman and Conner, 1996; Rimer, 1997; Bandura, 1998; Rosenstock et al., 1988; Institute of Medicine, 2002; Nigg et al., 2002a; Noar et al., 2003)], many of these theories contain constructs that are very similar (or identical), but use different terminology, creating the illusion that they are different. Whether similar constructs are indeed essentially the same is an important question that deserves much research attention. If constructs in different theories are the same, then this adds to our ability to synthesize knowledge if we are able to recognize this. Said another way, the lack of consensus regarding what to call certain constructs has resulted in a fragmented literature that could be better integrated if a common set of terminology was agreed upon.
In addition, constructs may come from different theoretical and conceptual origins, and have different names, yet when they are measured are essentially the same. Table I presents an example of constructs across different theories that are either similar or exactly the same. For instance, there is likely to be little difference between benefits and barriers, attitudes, positive and negative expectancies, and pros and cons. In fact, in a paper comparing alcohol expectancies and pros and cons, we found that they were quite similar (Noar et al., 2003). On the other hand, in the exercise arena a study demonstrated that attitudes (from the TRA/TPB) and pros and cons are quite different (Jordan et al., 2002). What is clear is that more work is needed in this area, and in addition that both conceptual and empirical points of view should be carefully considered when such constructs are compared.
Similar or identical elements within five health behavior theories
Concept | General tenet of the concept ‘Engaging in the behavior is likely if…’ | HBM | TRA | TPB | SCT | TTM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attitudinal beliefs | ||||||||||||
| Appraisal of the positive and negative aspects of the behavior and expected outcome of the behavior | the positive aspects outweigh the negative aspects | benefits, barriers/health motive | behavioral beliefs and evaluation of those beliefs (attitudes) | behavioral beliefs and evaluation of those beliefs (attitudes) | outcome expectations/expectancies | pros, cons (decisional balance) | ||||||
| Self-efficacy beliefs/beliefs about control over the behavior | ||||||||||||
| Belief in one's ability to perform the behavior; confidence | one believes in their ability to perform the behavior | self-efficacy | – | perceived behavioral control | self-efficacy | self-efficacy/temptation | ||||||
| Normative and norm-related beliefs and activities | ||||||||||||
| Belief that others want you to engage in the behavior (and one's motivation to comply); may include actual support of others | one believes that people important to them want them to engage in the behavior; person has others' support | cues from media, friends (cues to action) | normative beliefs and motivation to comply (subjective norms) | normative beliefs and motivation to comply (subjective norms) | social support | helping relationships (process of change) | ||||||
| Belief that others (e.g. peers) are engaging in the behavior | one believes that other people are engaging in the behavior | – | – | – | social environment/norms; modeling | social liberation (process of change) | ||||||
| Responses to one's behavior that increase or decrease the likelihood one will engage in the behavior; may include reminders | one receives positive reinforcement from others or creates positive reinforcements for themselves | cues from media, friends (cues to action) | –a | –a | reinforcement | reinforcement management/stimulus control (processes of change) | ||||||
| Risk-related beliefs and emotional responses | ||||||||||||
| Belief that one is at risk if one does not engage in the behavior, and that the consequences may be severe; may include actually experiencing negative emotions or symptoms and coping with them | one feels at risk with regard to a negative outcome or disease | perceived susceptibility/severity (perceived threat) | – | – | emotional coping responses/expectancies about environmental cues | dramatic relief (process of change) | ||||||
| Intention/commitment/planning | ||||||||||||
| Intending or planning to perform the behavior; setting goals or making a commitment to perform the behavior | one has formed strong behavioral intentions to engage in the behavior; one has set realistic goals or made a firm commitment to engage in the behavior | – | behavioral intentions | behavioral intentions | self-control/self-regulation | contemplation/preparation (stages of change); self-liberation (process of change) | ||||||
Concept | General tenet of the concept ‘Engaging in the behavior is likely if…’ | HBM | TRA | TPB | SCT | TTM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attitudinal beliefs | ||||||||||||
| Appraisal of the positive and negative aspects of the behavior and expected outcome of the behavior | the positive aspects outweigh the negative aspects | benefits, barriers/health motive | behavioral beliefs and evaluation of those beliefs (attitudes) | behavioral beliefs and evaluation of those beliefs (attitudes) | outcome expectations/expectancies | pros, cons (decisional balance) | ||||||
| Self-efficacy beliefs/beliefs about control over the behavior | ||||||||||||
| Belief in one's ability to perform the behavior; confidence | one believes in their ability to perform the behavior | self-efficacy | – | perceived behavioral control | self-efficacy | self-efficacy/temptation | ||||||
| Normative and norm-related beliefs and activities | ||||||||||||
| Belief that others want you to engage in the behavior (and one's motivation to comply); may include actual support of others | one believes that people important to them want them to engage in the behavior; person has others' support | cues from media, friends (cues to action) | normative beliefs and motivation to comply (subjective norms) | normative beliefs and motivation to comply (subjective norms) | social support | helping relationships (process of change) | ||||||
| Belief that others (e.g. peers) are engaging in the behavior | one believes that other people are engaging in the behavior | – | – | – | social environment/norms; modeling | social liberation (process of change) | ||||||
| Responses to one's behavior that increase or decrease the likelihood one will engage in the behavior; may include reminders | one receives positive reinforcement from others or creates positive reinforcements for themselves | cues from media, friends (cues to action) | –a | –a | reinforcement | reinforcement management/stimulus control (processes of change) | ||||||
| Risk-related beliefs and emotional responses | ||||||||||||
| Belief that one is at risk if one does not engage in the behavior, and that the consequences may be severe; may include actually experiencing negative emotions or symptoms and coping with them | one feels at risk with regard to a negative outcome or disease | perceived susceptibility/severity (perceived threat) | – | – | emotional coping responses/expectancies about environmental cues | dramatic relief (process of change) | ||||||
| Intention/commitment/planning | ||||||||||||
| Intending or planning to perform the behavior; setting goals or making a commitment to perform the behavior | one has formed strong behavioral intentions to engage in the behavior; one has set realistic goals or made a firm commitment to engage in the behavior | – | behavioral intentions | behavioral intentions | self-control/self-regulation | contemplation/preparation (stages of change); self-liberation (process of change) | ||||||
Variable names in parentheses indicate that the variable(s) above it are part of that larger category, according to the theory.
Both the TRA and TPB contain normative components that are conceptualized as beliefs in reinforcement (normative beliefs), rather than the actual reinforcement itself. It is not clear which conceptualization of these ideas is best for a theoretical framework.
Similar or identical elements within five health behavior theories
Concept | General tenet of the concept ‘Engaging in the behavior is likely if…’ | HBM | TRA | TPB | SCT | TTM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attitudinal beliefs | ||||||||||||
| Appraisal of the positive and negative aspects of the behavior and expected outcome of the behavior | the positive aspects outweigh the negative aspects | benefits, barriers/health motive | behavioral beliefs and evaluation of those beliefs (attitudes) | behavioral beliefs and evaluation of those beliefs (attitudes) | outcome expectations/expectancies | pros, cons (decisional balance) | ||||||
| Self-efficacy beliefs/beliefs about control over the behavior | ||||||||||||
| Belief in one's ability to perform the behavior; confidence | one believes in their ability to perform the behavior | self-efficacy | – | perceived behavioral control | self-efficacy | self-efficacy/temptation | ||||||
| Normative and norm-related beliefs and activities | ||||||||||||
| Belief that others want you to engage in the behavior (and one's motivation to comply); may include actual support of others | one believes that people important to them want them to engage in the behavior; person has others' support | cues from media, friends (cues to action) | normative beliefs and motivation to comply (subjective norms) | normative beliefs and motivation to comply (subjective norms) | social support | helping relationships (process of change) | ||||||
| Belief that others (e.g. peers) are engaging in the behavior | one believes that other people are engaging in the behavior | – | – | – | social environment/norms; modeling | social liberation (process of change) | ||||||
| Responses to one's behavior that increase or decrease the likelihood one will engage in the behavior; may include reminders | one receives positive reinforcement from others or creates positive reinforcements for themselves | cues from media, friends (cues to action) | –a | –a | reinforcement | reinforcement management/stimulus control (processes of change) | ||||||
| Risk-related beliefs and emotional responses | ||||||||||||
| Belief that one is at risk if one does not engage in the behavior, and that the consequences may be severe; may include actually experiencing negative emotions or symptoms and coping with them | one feels at risk with regard to a negative outcome or disease | perceived susceptibility/severity (perceived threat) | – | – | emotional coping responses/expectancies about environmental cues | dramatic relief (process of change) | ||||||
| Intention/commitment/planning | ||||||||||||
| Intending or planning to perform the behavior; setting goals or making a commitment to perform the behavior | one has formed strong behavioral intentions to engage in the behavior; one has set realistic goals or made a firm commitment to engage in the behavior | – | behavioral intentions | behavioral intentions | self-control/self-regulation | contemplation/preparation (stages of change); self-liberation (process of change) | ||||||
Concept | General tenet of the concept ‘Engaging in the behavior is likely if…’ | HBM | TRA | TPB | SCT | TTM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attitudinal beliefs | ||||||||||||
| Appraisal of the positive and negative aspects of the behavior and expected outcome of the behavior | the positive aspects outweigh the negative aspects | benefits, barriers/health motive | behavioral beliefs and evaluation of those beliefs (attitudes) | behavioral beliefs and evaluation of those beliefs (attitudes) | outcome expectations/expectancies | pros, cons (decisional balance) | ||||||
| Self-efficacy beliefs/beliefs about control over the behavior | ||||||||||||
| Belief in one's ability to perform the behavior; confidence | one believes in their ability to perform the behavior | self-efficacy | – | perceived behavioral control | self-efficacy | self-efficacy/temptation | ||||||
| Normative and norm-related beliefs and activities | ||||||||||||
| Belief that others want you to engage in the behavior (and one's motivation to comply); may include actual support of others | one believes that people important to them want them to engage in the behavior; person has others' support | cues from media, friends (cues to action) | normative beliefs and motivation to comply (subjective norms) | normative beliefs and motivation to comply (subjective norms) | social support | helping relationships (process of change) | ||||||
| Belief that others (e.g. peers) are engaging in the behavior | one believes that other people are engaging in the behavior | – | – | – | social environment/norms; modeling | social liberation (process of change) | ||||||
| Responses to one's behavior that increase or decrease the likelihood one will engage in the behavior; may include reminders | one receives positive reinforcement from others or creates positive reinforcements for themselves | cues from media, friends (cues to action) | –a | –a | reinforcement | reinforcement management/stimulus control (processes of change) | ||||||
| Risk-related beliefs and emotional responses | ||||||||||||
| Belief that one is at risk if one does not engage in the behavior, and that the consequences may be severe; may include actually experiencing negative emotions or symptoms and coping with them | one feels at risk with regard to a negative outcome or disease | perceived susceptibility/severity (perceived threat) | – | – | emotional coping responses/expectancies about environmental cues | dramatic relief (process of change) | ||||||
| Intention/commitment/planning | ||||||||||||
| Intending or planning to perform the behavior; setting goals or making a commitment to perform the behavior | one has formed strong behavioral intentions to engage in the behavior; one has set realistic goals or made a firm commitment to engage in the behavior | – | behavioral intentions | behavioral intentions | self-control/self-regulation | contemplation/preparation (stages of change); self-liberation (process of change) | ||||||
Variable names in parentheses indicate that the variable(s) above it are part of that larger category, according to the theory.
Both the TRA and TPB contain normative components that are conceptualized as beliefs in reinforcement (normative beliefs), rather than the actual reinforcement itself. It is not clear which conceptualization of these ideas is best for a theoretical framework.
In addition, we as a field should never be blind advocates interested only in finding support for particular theories. Rather, we should put theories to the strongest possible tests and when such theories do not stand up to rigorous evaluation, appropriate modifications should be made. As Greenwald et al. [(Greenwald et al., 1986), p. 227] state:
Ogden (Ogden, 2003) recently examined a systematic sample of 47 HBT studies and found that when data did not demonstrate support for certain aspects of theories, the authors tended to offer various explanations, none of which included that the theory may be incorrect. Ogden concluded that such theories cannot be tested because data are used to support HBT but are rarely if ever used to refute HBT. In fact, though a basic tenet of theory development is that theories should be falsifiable, this work by Ogden strongly suggests that many HBT's are in fact not falsifiable. In addition, many have suggested that a number of HBT's are not well specified in terms of the relations between variables [e.g. Fisher and Fisher, 1992; Weinstein, 1993; Rimer, 1997)], making them difficult to test and subsequently verify or falsify.Theory obstructs research progress when…the researcher has more faith in the correctness of the theory than in the suitability of the procedures that were used to test it.
Further, as already discussed, there are a finite number of questions that HBT should address. Our reading of the literature is that there is some consensus regarding which variables are most important to health behavior, though we use the word some generously [see Table I (Fishbein et al., 2001; Noar et al., 2004)]. There is much less consensus as to how the variables combine in an equation to predict behavior (Weinstein, 1993; Fishbein et al., 2001). This is a much more complex question, which may be facilitated by answers to the first question. Finally, whether there are differences (or similarities) across different behaviors and situations has been addressed somewhat within theories [e.g. (Madden et al., 1992; Prochaska et al., 1994)], but has rarely been addressed across theories. This is a question that may be better facilitated by answers to the more basic questions.
Finally, we should note that an issue that has been discussed in the literature is whether or not a single theory is appropriate across multiple behaviors, as compared to theories that are specific to certain behaviors. For instance, where illness avoidance and perceived threat are the most salient issues, a theory such as the HBM may be most appropriate (Biddle and Nigg, 2000; Murray-Johnson et al., 2001). For behaviors that are more rational in nature and in which the intention–behavior link is strong, theories such as the TRA/TPB may be most appropriate (Biddle and Nigg, 2000; Murray-Johnson et al., 2001). In addition, some suggest that stage models such as the TTM may be most applicable to deliberate behaviors (e.g. exercise) and less applicable to automatic behaviors that are simplistic [e.g. seatbelt use (Norman and Conner, 1996)]. Finally, a number of researchers point to the need for theoretical approaches to the maintenance of behavior change being distinct from initiation of behavior change [see (Wing et al., 2000). Clearly, more empirical work on the issue of specific versus general theories is warranted.
What is the best way to move forward?
Is the proposition and study of numerous HBTs the best way for the field to move forward? We next present three possible directions that the field could move in.
The current direction: proliferation and testing of theories
Theory drives research. It serves as a guide for knowing what variables to measure, how to measure them, and how to combine them. It also serves as a framework for aiding researchers in developing and evaluating intervention approaches. If a researcher believes that existing theories are inappropriate or incomplete, he or she can extend upon an existing theory or create a new theory altogether. When Ajzen and Madden (Ajzen and Madden, 1986) observed that the TRA could be improved, they proposed the TPB. Their research demonstrated that the addition of perceived behavioral control added variance in the prediction of health behaviors (Madden et al., 1992) and subsequent research found success in using the TPB as a guide for developing interventions [see (Hardeman et al., 2002)]. In addition, out of Prochaska and DiClemente's (Prochaska and DiClemente, 1983) work on smoking cessation came a new paradigm—a stage paradigm for understanding health behavior. This has resulted in successful intervention approaches across a variety of health behaviors [see (Burkholder and Evers, 2002)]. The current research model gives investigators complete autonomy to create their own theories and interventions based upon their own judgment.
Further, Glanz and Maddock (Glanz and Maddock, 2000) argue that out of what is sometimes a confusing literature, the best and brightest will emerge. That is, every health researcher could propose a theory, but only those best supported empirically and those that resonate with researchers would proliferate further inquiry. This is likely the current state of the literature, as numerous theories exist, but some theories are used much more than others. Researchers may use theory for other reasons than suggested by Glanz and Maddock (Glanz and Maddock, 2000), however. For instance, using a particular theory because it is easy to understand or it is the one learned during one's academic training. In addition, the fragmentation of the HBT literature because of multiple theories and its potential slowing of our understanding of health behavior have already been discussed as problems with this approach.
Another direction: the case for integration
If the case is made for theoretical integration, what would that mean? An integrated theory might take the constructs with the most support from varying theories and combine them into a single theory. This theory could then be subjected to rigorous testing across behaviors and situations, and refined as necessary. An integrated theory would first require that theorists agree on common conceptualizations and names for similar constructs.
There have been various attempts to create integrated theories of health behavior, and a recent example is Fishbein's (Fishbein, 2000) integrated theory [see also (Institute of Medicine, 2002)]. The core constructs of the theory are essentially the TRA constructs with the addition of self-efficacy. The theory also includes constructs such as demographics and personality variables as well as skills and environmental constraints. Fishbein's (Fishbein, 2000) integrated model grew out of a theorists' workshop that took place in 1991, in which many prominent theorists came together to identify core determinants of health behavior. The theorists produced a chapter that listed and described eight variables believed to be most important to health behavior and specifically to safer sexual behavior [see (Fishbein et al., 2001)]. They discussed similarities between constructs and theories, though a common set of terminology was not proposed. The way in which these constructs combine to effect behavior was not agreed upon and was discussed as an ‘unresolved issue’. Although Fishbein (Fishbein, 2000) suggests one conceptualization, additional conceptualizations of the same variables could also be tested. However, it is likely that many researchers would disagree with these core determinants, which is a major difficulty with the integrated approach.
A new direction: the case for theory comparison and beyond
While both proliferation and integration of theories have many problems associated with them, comparison of theories, we believe, is the most compelling direction to move in. Why empirically compare theories of health behavior to one another? Several reasons could be given, not the least of which is that we may not truly know which theories are most accurate if we do not do so. Consumers faced with making decisions regarding buying products (e.g. a stereo system, an automobile) often rely on product comparisons conducted by magazines such as Consumer Reports. How else can one know what product is best, if we do not compare one to the other? Theories are, in fact, academic products that are fashioned from well thought out conceptual work. Do they not justify comparison if they all claim to explain the same phenomena, yet have fundamental differences among them?
Theoretical comparisons are in many cases not difficult to conduct, they yield important results and we have the potential to learn much about HBT as a result of such comparisons. The fact that theories have so many similar constructs demands that we (1) try and discover what the best conceptualization of those constructs is, and (2) compare theories to discover how these constructs combine and result in the enactment of health behavior. Further, since many constructs in theories are similar or the same, when we measure one variable (e.g. self-efficacy) it may cut across many theories, allowing for a reasonable level of response burden on study participants.
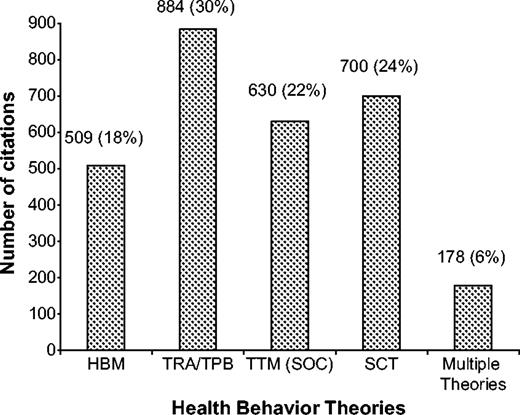
Despite this, few data-based empirical comparisons exist in the literature. Weinstein (Weinstein, 1993) reported that out of 205 theoretically based articles published between 1974 and 1991, only 10 articles mentioned more than one theory and only four of these 10 were empirical comparisons. In order to examine an updated state of empirical comparisons in the literature, we conducted a comprehensive search of the PsycInfo database through June of 2003. We searched for articles that were classified in PsycInfo as health-related articles (using the keyword health which includes health behavior, health attitude, etc.), and included peer-reviewed articles, book chapters, books and dissertations. We searched for the major theories discussed in this article (HBM, TRA/TPB, TTM, SCT), using advanced search commands so that we would not count articles twice. In addition, the PsycInfo search examined the title, abstract and keywords for potential matches to these criteria.
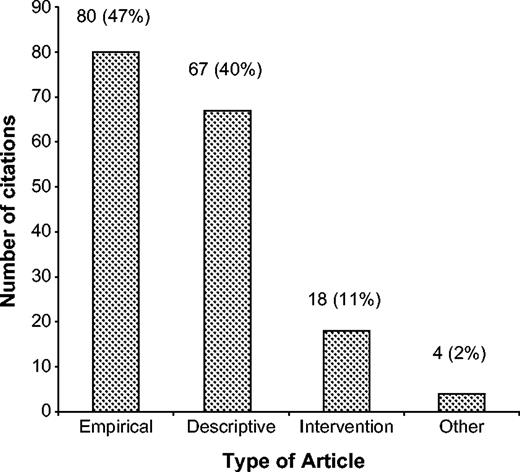
As can be seen in Figure 1, the vast majority of articles utilize just one theory (though we should note that some of the TRA/TPB studies compared the TRA with the TPB and we did not distinguish between them because these theories are so similar to one another). Only 178 (6%) out of a total of 2901 unique citations contained two or more theories in the search record. Further, when we more closely examined these 178 citations, we found the following. First, nine articles were excluded for various reasons (e.g. they were improperly coded in PsycInfo and had no relevance here). This left 169 articles, which were broken down into various categories in Figure 2. As one can see, N = 67 were not empirical studies, but rather were descriptive theoretical articles [e.g. (Sutton, 1987; Bandura, 1998)]. Next, N = 18 of the studies were intervention projects [e.g. (Pinto et al., 2002)], while N = 4 were categorized as ‘other,’ which contained studies such as qualitative focus group investigations [e.g. (Levy and Bavendam, 1995)]. Finally, N = 80 were empirical articles that utilized two or more of the theories or concepts from the theories (these were correlational/behavioral prediction articles). Thus, it is clear that more investigators are using multiple theories to inform their empirical investigations. Of these 80 empirical articles, seven were published before 1990, 47 were published between 1990 and 1999, and 26 were published between 2000 and June of 2003.
{kind=link}
Number of unique citations (total N = 2901) for individual versus multiple theories found in PsycInfo through June 2003.
{kind=link}
Categorization of N = 169 multiple theory citations found in PsycInfo through June 2003.
However, the major caveat here is that most of these articles were not empirical comparisons of two or more theories. Rather, many were ‘predictors’ articles that looked at selected concepts derived from various theories and examined their ability to predict health behavior [e.g. (Manfredi et al., 1998; Adih and Alexander, 1999)]. In fact, when we examined these 80 articles more closely, we identified only 13 published articles (in a journal or book chapter) that were true theoretical comparisons (0.4% of the 2901 total citations). Thus, though many more studies are utilizing multiple theories, empirical comparisons of these theories are still extremely rare in the research literature.
If more such comparisons were undertaken, we might start to have a clearer picture of the similarity or difference of constructs. The field could come to better agreement on what names to give to certain concepts, resulting in greater consensus and a shared conceptual language. And, although the end result might not be one unified theory of health behavior, we would certainly be moving in the direction of theories and models that truly integrate what we are learning from research. If we do not move in this direction, then we wish to pose a question. What is the point of the massive literature on theory testing? If it is to find support for numerous theories, then we are doing quite well. If it is to understand which concepts and theories are most related to health behavior, then some changes to the way we conduct such research are necessary.
How should researchers empirically compare theories?
We next consider how one might empirically compare theories and concepts from theories. We believe that studies that empirically compare individual concepts from theories are important because they suggest commonalties (or refute the idea of commonalties) across theories. A specific example of this are the numerous types of attitudinal beliefs described in Table I. If one is able to say with confidence that some of these concepts are identical, then response burden on participants will be lessened. On the other hand, if these concepts are indeed shown to be conceptually distinct, then more concepts will need to be measured. Comparison of concepts can be examined using a variety of correlational techniques (e.g. regression) to assess whether or not unique variance is added when a second concept is considered above and beyond a first concept (Noar et al., 2003). In addition, structural equation modeling (SEM) techniques can be used to examine measurement models of concepts in order to examine their similarity or difference (Jordan et al., 2002).
A more complex issue is how one might carry out comparisons of entire theories as advocated in this article. In order to examine theory comparison articles in the literature, we compiled articles from the PsycInfo search conducted, and supplemented the search with additional articles identified from the reference sections of the 13 theory comparison articles. All studies had to meet the following criteria in order to be included. First, they had to be English language journal articles or book chapters (dissertations were excluded). Second, they had to be non-redundant studies. If results from one study were published multiple times, only one article was chosen. Finally, they had to truly test theories, rather than testing selected components from theories. Although our list of theoretical comparisons is not exhaustive, we believe that our search captured a number of important comparisons in the literature.
Nineteen studies met the criteria and are described in Table II. All of the studies were correlational in nature and used survey data; none were lab-based or experimental studies. In terms of analytic techniques, by far the most common technique used was multiple regression, in which each theory was tested separately and the R2 values as well as the standardized regression coefficients (β weights) were compared. This allows one to examine the overall variance accounted for in the dependent variable (DV) as well as examine which specific variables were responsible for prediction of that variance. A second analytic technique, used in far fewer of the studies, was SEM. The approach here is similar to regression in that the overall fit of models is examined using various SEM fit indices and R2, while the contribution of specific variables is examined by standardized path coefficients. While multiple regression is a strong technique for testing and comparing theories, many would consider SEM (and path analysis) to be superior in part because it allows for several layers of endogenous variables (e.g. attitudes predict intentions which in turn predict behavior).
Empirical comparisons of HBTs (N = 19)
Article | Behavioral domain | Study design | Sample(s) | Theories compared | DV | Comparative strategy |
|---|---|---|---|---|---|---|
| Bish et al. (2000) | cervical cancer screening | longitudinal (baseline, 3 months) | N = 133 females, mean age: 38.1 (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Boyd and Wandersman (1991) | safer sex | longitudinal (baseline, 3 months) | N = 190 undergraduates, mean age: 18.9 (US) | TRA, TABM | intention, behavior | multiple regression for complete theories; R2. and significance of β weights compared |
| Conner and Graham (1993) | safer sex | cross-sectional | N = 218 undergraduates, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Conner and Norman (1994) | health screening | longitudinal (baseline, 6 months) | N = 407 individuals, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Garcia and Mann (2003) | resisting dieting and breast self-exam | cross-sectional | study 1: N = 159 female undergraduates; study 2: N = 120 female undergraduates; ages not reported (US) | HBM, HBM plus self-efficacy, TRA, TPB, HAPA | intention | multiple regression for complete theories; R2. and β weights compared |
| Hennig and Knowles (1990) | cervical cancer screening | cross-sectional | N = 144 females, mean age: 54 (US) | HBM, TRA | intention | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Hill et al. (1985) | breast self-examination, cervical cancer screening | cross-sectional | N = 123 females, median age: 34 (US) | HBM, TRA, SPM | intention | multiple regression for complete theories; R2. and β weights compared |
| Kloeblen et al. (1999) | breast-feeding | cross-sectional | N = 1001 females, mean age: 23 (US) | TRA, TTM | intention, stage of change | correlations for theoretical components. multiple regression for complete theories; R2. and partial R2 compared |
| Mullen et al., 1987 | smoking, exercise, dietary habits | longitudinal (baseline, 8 months) | N = 326 individuals aged 17–65 (US) | HBM, TRA, PRECEDE | behavior | multiple regression for complete theories; R2. and β weights compared |
| Murray-Johnson et al. (2001) | reproductive health | cross-sectional | N = 7540 individuals (Ghana); N = 3 621 individuals (Nepal); N = 2000 individuals (Nicaragua); ages not reported | HBM, TRA, SCT, EPPM | exposure, knowledge, attitudes, fear and danger control, intention, behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared |
| Oliver and Berger (1979) | inoculation behavior (flu shot) | cross-sectional | study 1: N = 323 undergraduates; study 2: N = 469 individuals; ages not reported (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Quine et al. (2000) | bicycle helmet use | longitudinal (baseline, 1 month) | N = 162 males aged 11–18 (UK) | HBM, TPB | behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Reid and Christensen (1988) | medication compliance for urinary tract infection | longitudinal (baseline, 10 days) | N = 107 undergraduate and other females aged 16–79 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Seibold and Roper (1979) | cervical cancer screening | cross-sectional | N = 93 undergraduate and other females aged 18–90 (US) | TRA, TABM | intention | multiple regression for theoretical components and complete theories; multiple correlation (R). and β weights compared |
| Seydel et al. (1990) | cancer prevention behaviors (e.g. breast self-exam, cancer screenings) | cross-sectional | study 1: N = 358 females, mean age: 48; study 2: N = 256 individuals, mean age: 38 (US) | HBM, PMT | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Vanlandingham et al. (1995) | safer sex | cross-sectional | N = 1472 males, mean age: 23 (Thailand) | HBM, TRA | behavior | correlations for theoretical components. logistic regression for complete theories; odds ratios and percent correctly classified compared |
| Warwick et al. (1993) | safer sex | longitudinal (baseline, 1 month) | N = 138 undergraduates, mean age: 18.6 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Wulfert and Wan (1995) | safer sex | two cross-sectional studies, one longitudinal study (baseline, 3 months) | study 1: N = 496 undergraduates, mean age: 20.3; study 2: N = 421 individuals, mean age: 46; study 3: N = 105 undergraduates, mean age: 20.6. (US) | HBM, TRA, SCT | intention, behavior | SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
| Wulfert et al. (1996) | safer sex | cross-sectional | N = 153 males, mean age: 37.4 (US) | HBM, TRA, SCT | behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
Article | Behavioral domain | Study design | Sample(s) | Theories compared | DV | Comparative strategy |
|---|---|---|---|---|---|---|
| Bish et al. (2000) | cervical cancer screening | longitudinal (baseline, 3 months) | N = 133 females, mean age: 38.1 (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Boyd and Wandersman (1991) | safer sex | longitudinal (baseline, 3 months) | N = 190 undergraduates, mean age: 18.9 (US) | TRA, TABM | intention, behavior | multiple regression for complete theories; R2. and significance of β weights compared |
| Conner and Graham (1993) | safer sex | cross-sectional | N = 218 undergraduates, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Conner and Norman (1994) | health screening | longitudinal (baseline, 6 months) | N = 407 individuals, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Garcia and Mann (2003) | resisting dieting and breast self-exam | cross-sectional | study 1: N = 159 female undergraduates; study 2: N = 120 female undergraduates; ages not reported (US) | HBM, HBM plus self-efficacy, TRA, TPB, HAPA | intention | multiple regression for complete theories; R2. and β weights compared |
| Hennig and Knowles (1990) | cervical cancer screening | cross-sectional | N = 144 females, mean age: 54 (US) | HBM, TRA | intention | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Hill et al. (1985) | breast self-examination, cervical cancer screening | cross-sectional | N = 123 females, median age: 34 (US) | HBM, TRA, SPM | intention | multiple regression for complete theories; R2. and β weights compared |
| Kloeblen et al. (1999) | breast-feeding | cross-sectional | N = 1001 females, mean age: 23 (US) | TRA, TTM | intention, stage of change | correlations for theoretical components. multiple regression for complete theories; R2. and partial R2 compared |
| Mullen et al., 1987 | smoking, exercise, dietary habits | longitudinal (baseline, 8 months) | N = 326 individuals aged 17–65 (US) | HBM, TRA, PRECEDE | behavior | multiple regression for complete theories; R2. and β weights compared |
| Murray-Johnson et al. (2001) | reproductive health | cross-sectional | N = 7540 individuals (Ghana); N = 3 621 individuals (Nepal); N = 2000 individuals (Nicaragua); ages not reported | HBM, TRA, SCT, EPPM | exposure, knowledge, attitudes, fear and danger control, intention, behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared |
| Oliver and Berger (1979) | inoculation behavior (flu shot) | cross-sectional | study 1: N = 323 undergraduates; study 2: N = 469 individuals; ages not reported (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Quine et al. (2000) | bicycle helmet use | longitudinal (baseline, 1 month) | N = 162 males aged 11–18 (UK) | HBM, TPB | behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Reid and Christensen (1988) | medication compliance for urinary tract infection | longitudinal (baseline, 10 days) | N = 107 undergraduate and other females aged 16–79 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Seibold and Roper (1979) | cervical cancer screening | cross-sectional | N = 93 undergraduate and other females aged 18–90 (US) | TRA, TABM | intention | multiple regression for theoretical components and complete theories; multiple correlation (R). and β weights compared |
| Seydel et al. (1990) | cancer prevention behaviors (e.g. breast self-exam, cancer screenings) | cross-sectional | study 1: N = 358 females, mean age: 48; study 2: N = 256 individuals, mean age: 38 (US) | HBM, PMT | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Vanlandingham et al. (1995) | safer sex | cross-sectional | N = 1472 males, mean age: 23 (Thailand) | HBM, TRA | behavior | correlations for theoretical components. logistic regression for complete theories; odds ratios and percent correctly classified compared |
| Warwick et al. (1993) | safer sex | longitudinal (baseline, 1 month) | N = 138 undergraduates, mean age: 18.6 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Wulfert and Wan (1995) | safer sex | two cross-sectional studies, one longitudinal study (baseline, 3 months) | study 1: N = 496 undergraduates, mean age: 20.3; study 2: N = 421 individuals, mean age: 46; study 3: N = 105 undergraduates, mean age: 20.6. (US) | HBM, TRA, SCT | intention, behavior | SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
| Wulfert et al. (1996) | safer sex | cross-sectional | N = 153 males, mean age: 37.4 (US) | HBM, TRA, SCT | behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
DV = dependent variable; TABM = Triandis attitude behavior model; HAPA = health action process approach; SPM = subjective probability model; PRECEDE = Predisposing, reinforcing, enabling factors model; EPPM = extended parallel process model; PMT = Protection motivation theory; SEM = structural equation modeling.
Empirical comparisons of HBTs (N = 19)
Article | Behavioral domain | Study design | Sample(s) | Theories compared | DV | Comparative strategy |
|---|---|---|---|---|---|---|
| Bish et al. (2000) | cervical cancer screening | longitudinal (baseline, 3 months) | N = 133 females, mean age: 38.1 (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Boyd and Wandersman (1991) | safer sex | longitudinal (baseline, 3 months) | N = 190 undergraduates, mean age: 18.9 (US) | TRA, TABM | intention, behavior | multiple regression for complete theories; R2. and significance of β weights compared |
| Conner and Graham (1993) | safer sex | cross-sectional | N = 218 undergraduates, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Conner and Norman (1994) | health screening | longitudinal (baseline, 6 months) | N = 407 individuals, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Garcia and Mann (2003) | resisting dieting and breast self-exam | cross-sectional | study 1: N = 159 female undergraduates; study 2: N = 120 female undergraduates; ages not reported (US) | HBM, HBM plus self-efficacy, TRA, TPB, HAPA | intention | multiple regression for complete theories; R2. and β weights compared |
| Hennig and Knowles (1990) | cervical cancer screening | cross-sectional | N = 144 females, mean age: 54 (US) | HBM, TRA | intention | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Hill et al. (1985) | breast self-examination, cervical cancer screening | cross-sectional | N = 123 females, median age: 34 (US) | HBM, TRA, SPM | intention | multiple regression for complete theories; R2. and β weights compared |
| Kloeblen et al. (1999) | breast-feeding | cross-sectional | N = 1001 females, mean age: 23 (US) | TRA, TTM | intention, stage of change | correlations for theoretical components. multiple regression for complete theories; R2. and partial R2 compared |
| Mullen et al., 1987 | smoking, exercise, dietary habits | longitudinal (baseline, 8 months) | N = 326 individuals aged 17–65 (US) | HBM, TRA, PRECEDE | behavior | multiple regression for complete theories; R2. and β weights compared |
| Murray-Johnson et al. (2001) | reproductive health | cross-sectional | N = 7540 individuals (Ghana); N = 3 621 individuals (Nepal); N = 2000 individuals (Nicaragua); ages not reported | HBM, TRA, SCT, EPPM | exposure, knowledge, attitudes, fear and danger control, intention, behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared |
| Oliver and Berger (1979) | inoculation behavior (flu shot) | cross-sectional | study 1: N = 323 undergraduates; study 2: N = 469 individuals; ages not reported (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Quine et al. (2000) | bicycle helmet use | longitudinal (baseline, 1 month) | N = 162 males aged 11–18 (UK) | HBM, TPB | behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Reid and Christensen (1988) | medication compliance for urinary tract infection | longitudinal (baseline, 10 days) | N = 107 undergraduate and other females aged 16–79 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Seibold and Roper (1979) | cervical cancer screening | cross-sectional | N = 93 undergraduate and other females aged 18–90 (US) | TRA, TABM | intention | multiple regression for theoretical components and complete theories; multiple correlation (R). and β weights compared |
| Seydel et al. (1990) | cancer prevention behaviors (e.g. breast self-exam, cancer screenings) | cross-sectional | study 1: N = 358 females, mean age: 48; study 2: N = 256 individuals, mean age: 38 (US) | HBM, PMT | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Vanlandingham et al. (1995) | safer sex | cross-sectional | N = 1472 males, mean age: 23 (Thailand) | HBM, TRA | behavior | correlations for theoretical components. logistic regression for complete theories; odds ratios and percent correctly classified compared |
| Warwick et al. (1993) | safer sex | longitudinal (baseline, 1 month) | N = 138 undergraduates, mean age: 18.6 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Wulfert and Wan (1995) | safer sex | two cross-sectional studies, one longitudinal study (baseline, 3 months) | study 1: N = 496 undergraduates, mean age: 20.3; study 2: N = 421 individuals, mean age: 46; study 3: N = 105 undergraduates, mean age: 20.6. (US) | HBM, TRA, SCT | intention, behavior | SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
| Wulfert et al. (1996) | safer sex | cross-sectional | N = 153 males, mean age: 37.4 (US) | HBM, TRA, SCT | behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
Article | Behavioral domain | Study design | Sample(s) | Theories compared | DV | Comparative strategy |
|---|---|---|---|---|---|---|
| Bish et al. (2000) | cervical cancer screening | longitudinal (baseline, 3 months) | N = 133 females, mean age: 38.1 (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Boyd and Wandersman (1991) | safer sex | longitudinal (baseline, 3 months) | N = 190 undergraduates, mean age: 18.9 (US) | TRA, TABM | intention, behavior | multiple regression for complete theories; R2. and significance of β weights compared |
| Conner and Graham (1993) | safer sex | cross-sectional | N = 218 undergraduates, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Conner and Norman (1994) | health screening | longitudinal (baseline, 6 months) | N = 407 individuals, age not reported (UK) | HBM, TPB | intention, behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Garcia and Mann (2003) | resisting dieting and breast self-exam | cross-sectional | study 1: N = 159 female undergraduates; study 2: N = 120 female undergraduates; ages not reported (US) | HBM, HBM plus self-efficacy, TRA, TPB, HAPA | intention | multiple regression for complete theories; R2. and β weights compared |
| Hennig and Knowles (1990) | cervical cancer screening | cross-sectional | N = 144 females, mean age: 54 (US) | HBM, TRA | intention | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Hill et al. (1985) | breast self-examination, cervical cancer screening | cross-sectional | N = 123 females, median age: 34 (US) | HBM, TRA, SPM | intention | multiple regression for complete theories; R2. and β weights compared |
| Kloeblen et al. (1999) | breast-feeding | cross-sectional | N = 1001 females, mean age: 23 (US) | TRA, TTM | intention, stage of change | correlations for theoretical components. multiple regression for complete theories; R2. and partial R2 compared |
| Mullen et al., 1987 | smoking, exercise, dietary habits | longitudinal (baseline, 8 months) | N = 326 individuals aged 17–65 (US) | HBM, TRA, PRECEDE | behavior | multiple regression for complete theories; R2. and β weights compared |
| Murray-Johnson et al. (2001) | reproductive health | cross-sectional | N = 7540 individuals (Ghana); N = 3 621 individuals (Nepal); N = 2000 individuals (Nicaragua); ages not reported | HBM, TRA, SCT, EPPM | exposure, knowledge, attitudes, fear and danger control, intention, behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared |
| Oliver and Berger (1979) | inoculation behavior (flu shot) | cross-sectional | study 1: N = 323 undergraduates; study 2: N = 469 individuals; ages not reported (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Quine et al. (2000) | bicycle helmet use | longitudinal (baseline, 1 month) | N = 162 males aged 11–18 (UK) | HBM, TPB | behavior | correlations for theoretical components. multiple regression for complete theories (path analysis); R2. and β weights compared |
| Reid and Christensen (1988) | medication compliance for urinary tract infection | longitudinal (baseline, 10 days) | N = 107 undergraduate and other females aged 16–79 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Seibold and Roper (1979) | cervical cancer screening | cross-sectional | N = 93 undergraduate and other females aged 18–90 (US) | TRA, TABM | intention | multiple regression for theoretical components and complete theories; multiple correlation (R). and β weights compared |
| Seydel et al. (1990) | cancer prevention behaviors (e.g. breast self-exam, cancer screenings) | cross-sectional | study 1: N = 358 females, mean age: 48; study 2: N = 256 individuals, mean age: 38 (US) | HBM, PMT | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Vanlandingham et al. (1995) | safer sex | cross-sectional | N = 1472 males, mean age: 23 (Thailand) | HBM, TRA | behavior | correlations for theoretical components. logistic regression for complete theories; odds ratios and percent correctly classified compared |
| Warwick et al. (1993) | safer sex | longitudinal (baseline, 1 month) | N = 138 undergraduates, mean age: 18.6 (US) | HBM, TRA | intention, behavior | correlations for theoretical components. multiple regression for complete theories; R2. and β weights compared |
| Wulfert and Wan (1995) | safer sex | two cross-sectional studies, one longitudinal study (baseline, 3 months) | study 1: N = 496 undergraduates, mean age: 20.3; study 2: N = 421 individuals, mean age: 46; study 3: N = 105 undergraduates, mean age: 20.6. (US) | HBM, TRA, SCT | intention, behavior | SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
| Wulfert et al. (1996) | safer sex | cross-sectional | N = 153 males, mean age: 37.4 (US) | HBM, TRA, SCT | behavior | correlations for theoretical components. SEM for complete theories; SEM fit indices compared (overall indices and specific standardized path coefficients) |
DV = dependent variable; TABM = Triandis attitude behavior model; HAPA = health action process approach; SPM = subjective probability model; PRECEDE = Predisposing, reinforcing, enabling factors model; EPPM = extended parallel process model; PMT = Protection motivation theory; SEM = structural equation modeling.
A number of these studies have some strengths, as well as some having weaknesses. Rather than discuss one particular study as a model study, we focus on characteristics of strong comparisons (see Table III). Most of these characteristics are self-explanatory and thus we elaborate here only briefly. Some methodological strengths of studies included longitudinal designs, using SEM, having a strong sample size, and utilizing non-college samples and multiple samples. Some conceptual strengths included examining more than one behavior, more than one DV, more than two theories and examining an integrated model based on the results of the comparison. These methodological and conceptual strengths of studies are recommended in future theory comparison studies where possible. Further, theories vary in a number of ways such as which DV is most important and whether or not past behavior or demographics are important. Thus, we recommend that theory comparison studies in turn test theories in a number of ways within a single study, including testing multiple DVs [e.g. (Bish et al., 2001)] as well as testing theories with and without past behavior [e.g. (Quine et al. 2000)] and demographics controlled for [e.g. (Vanlandingham et al., 1995)]. We also note that studies examining multiple health behaviors allow us to examine the important question of how generalizable HBTs are across behaviors. Finally, studies examining integrated models [e.g. (Wulfert et al., 1996)] begin to move us in the direction of where this line of inquiry may ultimately take us.
Summary of strong characteristics of theory comparison studies (total N = 19)
Study characteristic | No. of Studies |
|---|---|
| Longitudinal study | 8/19 |
| Used SEM | 3/19 |
| Included past behavior in some or all model tests | 3/19 |
| Included demographics in some or all model tests | 4/19 |
| Included non-college participants in some or all samples | 15/19 |
| Had strong sample size in one or more samples (>200) | 10/19 |
| Utilized multiple samples in model testing | 5/19 |
| Utilized samples from more than one country | 1/19 |
| Had >1 DV (e.g. intention and behavior) | 11/19 |
| Examined more than one behavior | 4/19 |
| Compared more than two theories | 6/19 |
| Empirically examined an integrated model | 6/19 |
Study characteristic | No. of Studies |
|---|---|
| Longitudinal study | 8/19 |
| Used SEM | 3/19 |
| Included past behavior in some or all model tests | 3/19 |
| Included demographics in some or all model tests | 4/19 |
| Included non-college participants in some or all samples | 15/19 |
| Had strong sample size in one or more samples (>200) | 10/19 |
| Utilized multiple samples in model testing | 5/19 |
| Utilized samples from more than one country | 1/19 |
| Had >1 DV (e.g. intention and behavior) | 11/19 |
| Examined more than one behavior | 4/19 |
| Compared more than two theories | 6/19 |
| Empirically examined an integrated model | 6/19 |
Summary of strong characteristics of theory comparison studies (total N = 19)
Study characteristic | No. of Studies |
|---|---|
| Longitudinal study | 8/19 |
| Used SEM | 3/19 |
| Included past behavior in some or all model tests | 3/19 |
| Included demographics in some or all model tests | 4/19 |
| Included non-college participants in some or all samples | 15/19 |
| Had strong sample size in one or more samples (>200) | 10/19 |
| Utilized multiple samples in model testing | 5/19 |
| Utilized samples from more than one country | 1/19 |
| Had >1 DV (e.g. intention and behavior) | 11/19 |
| Examined more than one behavior | 4/19 |
| Compared more than two theories | 6/19 |
| Empirically examined an integrated model | 6/19 |
Study characteristic | No. of Studies |
|---|---|
| Longitudinal study | 8/19 |
| Used SEM | 3/19 |
| Included past behavior in some or all model tests | 3/19 |
| Included demographics in some or all model tests | 4/19 |
| Included non-college participants in some or all samples | 15/19 |
| Had strong sample size in one or more samples (>200) | 10/19 |
| Utilized multiple samples in model testing | 5/19 |
| Utilized samples from more than one country | 1/19 |
| Had >1 DV (e.g. intention and behavior) | 11/19 |
| Examined more than one behavior | 4/19 |
| Compared more than two theories | 6/19 |
| Empirically examined an integrated model | 6/19 |
A brief note on meta-analysis
One may wonder whether meta-analyses and systematic literature reviews have the potential to integrate and compare HBTs in ways we advocate in this article. First, we note that without a doubt, meta-analysis has helped synthesize the literature on correlates of health behavior in a way that few if any other techniques could do. However, meta-analyses and research reviews often examine effect sizes based on bivariate correlations [e.g. (Gerrard et al., 1996; Sheeran et al., 1999)] or significance ratios (Janz and Becker, 1984). Although these are excellent contributions to the literature, they contribute more to our understanding of the relationship of individual variables to behavior rather than theories. Some have recently used meta-analysis as more of a theory testing technique [e.g. (Albarracin et al., 2001; Hagger et al., 2002)] and we view this as an excellent step in the right direction.
Lipsey and Wilson (Lipsey and Wilson, 2001) note that it is still quite difficult to use meta-analysis to analyze findings from multivariate analyses such as multiple regression and SEM. Thus, while meta-analysis can certainly bring some consensus to this area, there are currently some difficulties in using it as a multivariate theory testing and comparison technique. In fact, we are not aware of any published studies that have used meta-analysis to compare HBTs (with the exception of TRA/TPB meta-analyses, which have just one variable to manipulate to make it a theory comparison). We encourage researchers to examine novel ways to use meta-analysis as a theory testing and theory comparison technique.
Moving the dialogue forward
Since so much research on health behavior is theory based, it is crucial that the field ‘audit’ itself to be sure that we are moving in the right direction. Glanz et al.'s (Glanz et al., 1997a) review of the health education literature published between mid-1992 and 1994 found that 526 articles (45%) of 1174 utilized some theory or model. This is no small amount of research and we as a field owe it to ourselves to continue this dialogue on the best way to move forward. Since researchers value and apply theory in the study of health behavior, we believe it remains an important task to refine theory and move toward consensus in the field where possible.
What theory or theories predict behavior most precisely, and what are the key principles of behavior change? We think it is fair to say that at this point in the literature, we are not entirely sure. Table I in this article presented some of the major concepts of HBTs and suggested some key principles of behavior change. It is now up to researchers in the field to uncover how these and other principles work together and result in the enactment of health behaviors, by asking important questions and putting them to empirical tests (see Table IV). We applaud attempts to move in this direction and integrate knowledge in this area, such as Fishbein's (Fishbein, 2000) integrative model and Prochaska et al.'s (Prochaska, 1992) TTM. However, the problem remains that these two theories, as one example, have many differences. Therefore, we must rely on empirical comparisons of such theories to understand which operates best. Rimer [(Rimer, 1997), p. 146] reminds us that ‘Theory is not theology. Theory needs questioners more than loyal followers’. What the field needs are researchers who are willing to put these concepts and theories to the strongest possible tests, so we can progress further in understanding health behavior and health behavior change.
Suggested important theory comparison questions for the field
Research questions | Examples of application |
|---|---|
| 1. What is the extent of similarity or difference regarding constructs from differing theories that appear to be similar or the same in nature? | Is there any difference among behavioral beliefs (TRA), benefits and barriers (HMB), outcome expectancies (SCT), and decisional balance (TTM)? Are there substantive conceptual differences between perceived behavioral control (TPB) and self-efficacy (SCT) or are they essentially the same? |
| 2. Are certain theories or elements of theories more useful in terms of predicting behavior or behavior change as compared to others? | Does the stage-based TTM or continuum-based TRA provide better prediction of behavior? |
| 3. Are the combinatorial rules for one theory better supported empirically than for other theories? | Are health behaviors mediated by intention formation (as TRA/TPB suggest) or not (as the HBM suggests)? |
| 4. Are certain theories or elements of theories better predictors of addictive behaviors (as opposed to non-addictive behaviors)? | Are SCT constructs better at predicting addictive behaviors, while TPB constructs are better at predicting non-addictive behaviors? |
| 5. Are certain theories or elements of theories better predictors of one-time behaviors (e.g. vaccinations) as opposed to behaviors that must be maintained over time (e.g. exercise)? | Are HBM constructs better at predicting one-time behaviors, while constructs from the TTM better at predicting behaviors that must be maintained? |
| 6. Are certain theories or elements of theories better predictors of cessation behaviors (e.g. smoking cessation) as opposed to behaviors that must be adopted (e.g. exercise)? | Do theories such as the TRA/TPB predict adoption behaviors better than cessation behaviors, or vice versa? |
| 7. Are certain theories or elements of theories better predictors in different cultures? | Is self-efficacy a better predictor in cultures with more of a focus on individualism, and beliefs and norms better predictors in cultures with more of a focus on collectivism? |
| 8. Is there one set of behavior change principles that can account for all health behaviors, or are they different according to different behaviors, cultures and contexts? | Questions 4–7 address this |
Research questions | Examples of application |
|---|---|
| 1. What is the extent of similarity or difference regarding constructs from differing theories that appear to be similar or the same in nature? | Is there any difference among behavioral beliefs (TRA), benefits and barriers (HMB), outcome expectancies (SCT), and decisional balance (TTM)? Are there substantive conceptual differences between perceived behavioral control (TPB) and self-efficacy (SCT) or are they essentially the same? |
| 2. Are certain theories or elements of theories more useful in terms of predicting behavior or behavior change as compared to others? | Does the stage-based TTM or continuum-based TRA provide better prediction of behavior? |
| 3. Are the combinatorial rules for one theory better supported empirically than for other theories? | Are health behaviors mediated by intention formation (as TRA/TPB suggest) or not (as the HBM suggests)? |
| 4. Are certain theories or elements of theories better predictors of addictive behaviors (as opposed to non-addictive behaviors)? | Are SCT constructs better at predicting addictive behaviors, while TPB constructs are better at predicting non-addictive behaviors? |
| 5. Are certain theories or elements of theories better predictors of one-time behaviors (e.g. vaccinations) as opposed to behaviors that must be maintained over time (e.g. exercise)? | Are HBM constructs better at predicting one-time behaviors, while constructs from the TTM better at predicting behaviors that must be maintained? |
| 6. Are certain theories or elements of theories better predictors of cessation behaviors (e.g. smoking cessation) as opposed to behaviors that must be adopted (e.g. exercise)? | Do theories such as the TRA/TPB predict adoption behaviors better than cessation behaviors, or vice versa? |
| 7. Are certain theories or elements of theories better predictors in different cultures? | Is self-efficacy a better predictor in cultures with more of a focus on individualism, and beliefs and norms better predictors in cultures with more of a focus on collectivism? |
| 8. Is there one set of behavior change principles that can account for all health behaviors, or are they different according to different behaviors, cultures and contexts? | Questions 4–7 address this |
Suggested important theory comparison questions for the field
Research questions | Examples of application |
|---|---|
| 1. What is the extent of similarity or difference regarding constructs from differing theories that appear to be similar or the same in nature? | Is there any difference among behavioral beliefs (TRA), benefits and barriers (HMB), outcome expectancies (SCT), and decisional balance (TTM)? Are there substantive conceptual differences between perceived behavioral control (TPB) and self-efficacy (SCT) or are they essentially the same? |
| 2. Are certain theories or elements of theories more useful in terms of predicting behavior or behavior change as compared to others? | Does the stage-based TTM or continuum-based TRA provide better prediction of behavior? |
| 3. Are the combinatorial rules for one theory better supported empirically than for other theories? | Are health behaviors mediated by intention formation (as TRA/TPB suggest) or not (as the HBM suggests)? |
| 4. Are certain theories or elements of theories better predictors of addictive behaviors (as opposed to non-addictive behaviors)? | Are SCT constructs better at predicting addictive behaviors, while TPB constructs are better at predicting non-addictive behaviors? |
| 5. Are certain theories or elements of theories better predictors of one-time behaviors (e.g. vaccinations) as opposed to behaviors that must be maintained over time (e.g. exercise)? | Are HBM constructs better at predicting one-time behaviors, while constructs from the TTM better at predicting behaviors that must be maintained? |
| 6. Are certain theories or elements of theories better predictors of cessation behaviors (e.g. smoking cessation) as opposed to behaviors that must be adopted (e.g. exercise)? | Do theories such as the TRA/TPB predict adoption behaviors better than cessation behaviors, or vice versa? |
| 7. Are certain theories or elements of theories better predictors in different cultures? | Is self-efficacy a better predictor in cultures with more of a focus on individualism, and beliefs and norms better predictors in cultures with more of a focus on collectivism? |
| 8. Is there one set of behavior change principles that can account for all health behaviors, or are they different according to different behaviors, cultures and contexts? | Questions 4–7 address this |
Research questions | Examples of application |
|---|---|
| 1. What is the extent of similarity or difference regarding constructs from differing theories that appear to be similar or the same in nature? | Is there any difference among behavioral beliefs (TRA), benefits and barriers (HMB), outcome expectancies (SCT), and decisional balance (TTM)? Are there substantive conceptual differences between perceived behavioral control (TPB) and self-efficacy (SCT) or are they essentially the same? |
| 2. Are certain theories or elements of theories more useful in terms of predicting behavior or behavior change as compared to others? | Does the stage-based TTM or continuum-based TRA provide better prediction of behavior? |
| 3. Are the combinatorial rules for one theory better supported empirically than for other theories? | Are health behaviors mediated by intention formation (as TRA/TPB suggest) or not (as the HBM suggests)? |
| 4. Are certain theories or elements of theories better predictors of addictive behaviors (as opposed to non-addictive behaviors)? | Are SCT constructs better at predicting addictive behaviors, while TPB constructs are better at predicting non-addictive behaviors? |
| 5. Are certain theories or elements of theories better predictors of one-time behaviors (e.g. vaccinations) as opposed to behaviors that must be maintained over time (e.g. exercise)? | Are HBM constructs better at predicting one-time behaviors, while constructs from the TTM better at predicting behaviors that must be maintained? |
| 6. Are certain theories or elements of theories better predictors of cessation behaviors (e.g. smoking cessation) as opposed to behaviors that must be adopted (e.g. exercise)? | Do theories such as the TRA/TPB predict adoption behaviors better than cessation behaviors, or vice versa? |
| 7. Are certain theories or elements of theories better predictors in different cultures? | Is self-efficacy a better predictor in cultures with more of a focus on individualism, and beliefs and norms better predictors in cultures with more of a focus on collectivism? |
| 8. Is there one set of behavior change principles that can account for all health behaviors, or are they different according to different behaviors, cultures and contexts? | Questions 4–7 address this |
We gratefully acknowledge the thoughtful suggestions of the three anonymous reviewers.
References
Adih, W.K. and Alexander, C.S. (
Ajzen, I. and Fishbein, M. (
Ajzen, I. and Madden, T.J. (
Albarracin, D., Johnson, B.T., Fishbein, M. and Muellerleile, P.A. (
Bandura, A. (
Bandura, A. (
Becker, M.H. (ed.) (
Biddle, S.J.H. and Nigg, C.R. (
Bish, A., Sutton, S. and Golombok, S. (
Boyd, B. and Wandersman, A. (
Burkholder, G.J. and Evers, K.E. (
Catania, J.A., Kegeles, S.M. and Coates, T.J. (
Connelly, J. (
Conner, M. and Graham, S. (
Conner, M. and Norman, P. (
Crosby, R.A., Kegler, M.C. and DiClemente, R.J. (
Cummings, K.M., Becker, M.H. and Maile, M.C. (
DiClemente, R.J., Crosby, R.A. and Kegler, M.C. (eds) (
Fishbein, M., Triandis, H.C., Kanfer, F.H., Becker, M., Middlestadt, S.E. and Eichler, A. (
Fisher, J.D. and Fisher, W.A. (
Fisher, J.D. and Fisher, W.A. (
Garcia, K. and Mann, T. (
Gerrard, M., Gibbons, F.X. and Bushman, B.J. (
Glanz, K. and Maddock, J. (
Glanz, K., Lewis, F.M. and Rimer, B.K. (
Glanz, K., Lewis, F.M. and Rimer, B.K. (eds) (
Glanz, K., Rimer, B.K. and Lewis, F.M. (eds) (
Glasgow, R.E., Dzewaltowski, D.A., Estabrooks, P.A., Klesges, L.M. and Bull, S.S. (
Godin, G. and Kok, G. (
Greenwald, A.G., Pratkanis, A.R., Leippe, M.R. and Baumgardner, M.H. (
Hagger, M.S., Chatzisarantis, N.L.D. and Biddle, S.J.H. (
Hardeman, W., Johnston, M., Johnston, D.W., Bonetti, D., Wareham, N.J. and Kinmonth, A.L. (
Harrison, J.A., Mullen, P.D. and Green, L.W. (
Hausenblaus, H., Carron, A.V. and Mack, D.E. (
Hennig, P. and Knowles, A. (
Hill, D., Gardner, G. and Rassaby, J. (
Institute of Medicine (
Janz, N.K. and Becker, M.H. (
Jones, B.T., Corbin, W. and Fromme, K. (
Jordan, P.J., Nigg, C.R., Norman, G.J., Rossi, J.S. and Benisovich, S.V. (
Kegler, M.C., Crosby, R.A. and DiClemente, R.J. (
Kloeblen, A.S., Thompson, N.J. and Miner, K.R. (
Levy, R.I. and Bavendam, T.G. (
Madden, T.J., Ellen, P.S. and Ajzen, I. (
Manfredi, C., Lacey, L., P., Warnecke, R. and Petraitis, J. (
Mullen, P.D., Hersey, J.C. and Iverson, D.C. (
Murray-Johnson, L., Witte, K., Boulay, M., Figueroa, M.E., Storey, D. and Tweedie, I. (
Nigg, C.R., Allegrante, J.P. and Ory, M. (
Nigg, C. R., Allegrante, J. P. and Ory, M. (eds) (
Noar, S.M., Laforge, R.G., Maddock, J.E. and Wood, M.D. (
Noar, S.M., Anderman, E.M., Zimmerman, R.S. and Cupp, P.K. (
Norman, P. and Conner, M. (
Ogden, J. (
Oliver, R.L. and Berger, P.K. (
Pinto, B., Friedman, R., Marcus, B.H., Kelley, H., Tennstedt, S. and Gillman, M.W. (
Prochaska, J.O. and DiClemente, C.C. (
Prochaska, J.O., DiClemente, C.C. and Norcross, J.C. (
Prochaska, J.O., Velicer, W.F., Rossi, J.S., Goldstein, M.G., Marcus, B.H., Rakowski, W., Fiore, C., Harlow, L.L., Redding, C.A., Rosenbloom, D. and Rossi, S. (
Quine, L., Rutter, D.R. and Arnold, L. (
Reed, L.D. and Christensen, D.B. (
Rimer, B.K. (
Rosen, C.S. (
Rosenstock, I.M., Strecher, V.J. and Becker, M.H. (
Seibold, D.R. and Roper, R.E. (
Seydel, E., Taal, E. and Wiegman, O. (
Sheeran, P., Abraham, C. and Orbell, S. (
Smedslund, G. (
Smedslund, G. (
Spencer, L., Pagell, F., Hallion, M.E. and Adams, T.B. (
Strecher, V.J., DeVellis, B.M., Becker, M.H. and Rosenstock, I.M. (
Sutton, S. (
Vanlandingham, M.J., Suprasert, S., Grandjean, N. and Sittitrai, W. (
Warwick, P., Terry, D. and Gallois, C. (
Weinstein, N.D. (
Werch, C.E., Pappas, D.M., Carlson, J.M., Edgemon, P., Sinder, J.A. and DiClemente, C.C. (
Wing, R.R., Voorhees, C.C. and Hill, D.R. (eds) (
Wulfert, E. and Wan, C.K. (
Wulfert, E., Wan, C.K. and Backus, C.A. (
Author notes
1Department of Communication, University of Kentucky, Lexington, KY 40506-0042, USA