
Abstract
The aim of this study was to determine the feasibility of the Z0011 criteria to Chinese breast cancer patients. An survey about the Z0011 trial was distributed and we collected 658 consecutive patients with axillary lymph node dissection (ALND) after positive sentinel lymph node (SLN) biopsy from five centers’ databases and grouped them as eligible or ineligible for omitting ALND according to the Z0011 criteria. The eligible group was compared with the cohort included in the Z0011 trial and with the ineligible group. Of the 427 respondants, 106 (24.8%) and 130 (30.4%)would not routinely perform ALND in patients meeting Z0011 criteria before and after learning of the trial results, respectively. Among the 658 patients, 151 (22.9%) were eligible and 507 were ineligible for omitting ALND. The clinicopathologic factors were not statistically different between the eligible group and the Z0011 cohort. Compared with the eligible Group, the ineligible group had significantly more T2 and T3 stage tumors, positive lymph nodes(LNs) and positive non-sentinel lymph nodes (NSLNs) (P < 0.01). The findings suggest good exportability of the Z0011 criteria to Chinese patients omitting ALND, but application of Z0011 as national treatment guideline still needs additional time and effort.
Similar content being viewed by others

Introduction
Sentinel lymph node (SLN) biopsy is currently the standard of care for staging clinically negative axilla in breast cancer patients, with axillary lymph node dissection(ALND) reserved for patients with metastases found by SLN biopsy1,2,3. The American College of Surgeons (ACOSOG) Z0011 trial demonstrated that in clinically node -negative women undergoing breast-conserving therapy (BCT) and found to have metastases to 1 or 2 SLNs, sentinel lymph node biopsy (SLNB) alone resulted in rates of local control, disease-free survival (DFS) and overall survival (OS) equivalent to those seen after ALND but with significantly lower morbidity4,5. Based on their findings, current guidelines from the American Society of Clinical Oncology and the National Comprehensive Cancer Network recommend considering no further surgery for patients who meet ACOSOG Z0011 eligibility criteria6.
Several surveys conducted by researchers in the United States revealed that many surgeons were likely to incorporate Z0011 into their practice7,8 and several centers have already modified their practice based on the Z0011 criteria9,10. Practice in China has been slower to incorporate the Z0011 criteria into its standard of care for some reasons. It is well known that there are some differences in the clinical characteristics between Chinese breast cancers patients and westerners. One of our previous studies has shown that western non-sentinel lymph node (NSLN) metastasis predicting nomogram dose not perform as well as in their original studies when used in Chinese patients11. This is a strong evidence to support that Chinese breast cancer patients are different from western populations. Therefore questions have been raised about whether data analyzing a US cohort in Z0011 are applicable to Chinese patients. Moreover there is no current information regarding how Z0011 has affected Chinese surgeons’ practice patterns across the nation.
So the purpose of this study is to assess the impact of Z0011 on surgeons’ practices across China, analyse the clinical relevance of the Z0011 findings for Chinese breast cancer patients and eventually evaluate the feasibility of using the Z0011 criteria to omit axillary lymph node dissection after positive sentinel lymph node biopsy in Chinese breast cancer patients.
Methods
Survey
The survey designed as detailed below was reviewed by the Chinese Preventive Medicine Association Research Committee and approved by the Board of Directors.
A seven-question survey was sent to every member of Surgical Group of Breast Cancer affiliated with Chinese Preventive Medicine Association by electronic mail. Five questions assessed the grade of the hospital in which each surgeon practices; the location of each surgeon’s affiliation; and each surgeon’s degree, practice duration and familiarity with Z0011. The sixth question assessed preferences for treatment of patients who meet the inclusion criteria and the treatment protocol of the Z0011 trial: T1 or T2, clinically node-negative invasive breast cancer ; one or two positive SLNs by routine haematoxylin and eosin (H&E) staining or frozen section; and treatment with breast-conserving therapy(BCT), whole breast irradiation(WBI) and adjuvant systemic therapy (chemotherapyand/or endocrine therapy) before learning of Z0011. After a simple explanation of Z0011’s results, the last question assessed the impact of Z0011 on the management of the same patients as the sixth question after the surgeon had learned of Z0011.
The first e-mail with request to complete the survey was sent on August 1, 2014 and the survey was closed on October 1, 2014.
Study patients
We reviewed the medical records of 658 breast cancer patients admitted to five different hospitals from December 2008 through October 2014. 194 patients from the Breast Center of Peking University People’s Hospital(PKUPH )(Beijing, China), 206 patients from Breast Surgery Service of Cancer Center of Henan Province(Zhengzhou, Beijing), 161 patients from Breast Disease Center of First Hospital of Peking University (Beijing, China), 66 patients from Breast Surgery Service of First Hospital of Jilin University(Changchun, China) and 31 patients from Breast Surgery Service of Second Hospital of Shandong University(Jinan, China). Patients were selected if they had pathologically confirmed breast cancer with clinically negative lymph nodes before surgery, had positive SLNs on routine H&E staining or frozen section, had not received any neoadjuvant systemic therapy and had ALND after positive sentinel lymph node biopsy(SLNB). Approval from Peking University People’s Hospital’s review board was obtained before data collection. The patient data collection methods were carried out in accordance with the approved guidelines. Written consent was obtained from all the patients.
Surgery and SLN pathological evaluation
SLNs were identified using fluorescence and/or blue dye according to surgeon preference. Intraoperative frozen section was performed on all SLNs. The SLN was cut longitudinally into 2 halves. Half of the node was frozen for immediate examination and up to 2 sections were stained with H&E. The other half node was fixed in formalin and embedded in paraffin and up to 2 sections were stained with H&E. Immunohistochemical stain was not routinely used in the diagnosis of SLN metastasis.
Axillary dissection was performed if SLN was positive by frozen section analysis. Patients with SLN metastases that were not detected during surgery generally underwent completion ALND at a later date. For all additional nodes identified by completion ALND, routine H&E analysis was conducted on a single section of each node.
Clinical and pathological characters
The clinical and pathological data collected for each case included age, clinical tumor size, nuclear grade, estrogen receptor (ER) expression, progesterone receptor (PR) expression, number of positive SLN, number of positive LN, number of positive non-sentinel lymph node (NSLN), surgical treatment (breast conserving therapy (BCT) or mastectomy), adjuvant systemic chemotherapy and/or endocrine therapy after surgery (yes or no) and whole breast irradiation after surgery(yes or no).
Comparison and Statistical Analysis
The survey results were analysed with descriptive statistics.
Factors associated with surgeons’ surgical practice pattern were analysed using Chi-squared test and Fisher’s exact test.
All the 658 patients were divided into an eligible group comprising patients who met the Z0011 criteria for omitting ALND and an ineligible group comprising patients who did not meet these criteria. The eligible group was compared with the cohort included in the “ALND” arm of the Z0011 trial (n = 420, in intention to treat) and the eligible group was also compared to the ineligible group. Chi-squared test and Fisher’s exact test were used for categorical variables.
SPSS19.0 software was used for statistical analyses. A P value of <0.05 was considered significant.
Results
427 surgeons completed the online questionnaire. The information in the survey is listed in Table 1. The majority (75.9%) of surgeons practiced in a third-grade class-A hospital, which is the highest level granted to a hospital according to Chinese health administrative department provision. 283(66.3%) surgeons practiced in municipalities directly under central government. A total of 185(43.3%) had medical master degrees and 122(28.6%) had acquired doctor degrees. Practice duration varied among the respondents : 120(28.1%) had been in practice for 0–5 years, 168(39.3%) for 5–10 years, 101(23.7%) for 10–15 years and 38(8.9%) for over 20 years. Only 116(27.2%) of respondents indicated familiarity with Z0011. Before learning of the trial results, 144(33.7%) would perform completion ALND all of the time on a woman eligible by the Z0011 criteria, 177(41.5%) would perform completion ALND most of the time and 106(24.8%) would not routinely perform ALND. Whether or not the surgeon was aware of Z0011, we explained the Z0011 trial results in our survey. After learning of them, 119 (27.9%) would perform completion ALND all of the time, 178(41.7%) would perform completion ALND most of the time and 130(30.4%) would not routinely perform ALND in such patients.
According to the respondents’ opinions of surgical treatment for patients fulfilling the criteria of Z0011 after learning of the trial results, we divided them into one group of ALND preference including surgeons who would perform completion ALND all of the time or most of the time and another group of ALND non-preference, including those who would not routinely perform ALND. The statistical result indicated there were no correlations between grade of hospital, location of hospital, surgeon’s degree, surgeon’s practice duration and surgeon’s preference for ALND after they learned of the Z0011 results (p < 0.05) (Table 2).
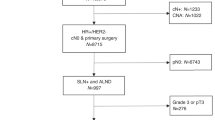
Among the 658 patients enrolled in the current study, 151(22.9%) fulfilled the Z0011 criteria: clinical stage T1 or T2 breast cancer; one or two positive SLNs; and treatment with breast-conserving therapy, whole breast irradiation and adjuvant systemic therapy (chemotherapy and/or endocrine therapy) and were assigned to the eligible group. The rest of the patients (507, 77.1%) were assigned to the ineligible group. In the ineligible group, 490 patients had a mastectomy, 65 patients had more than 2 positive SLNs and 20 patients had tumors with diameter more than 5 cm (Fig. 1).

Diagram of patient groups.
The ER status, clinical stage, number of positive lymph nodes (LNs) and positive NSLNs were not significantly different between the eligible group and the Z0011 cohort. The patients in the eligible group had more grade II tumors than the Z0011 cohort (p = 0.001) (Table 3).
Compared with the eligible group in this study, the ineligible group had significantly more T2 and T3 stage tumors, positive LNs and positive NSLNs (P < 0.01). However there was no significant difference in ER status, clinical stage and nuclear grade between these two groups (Table 4).
Discussion
Prior to publication of Z0011, it had been questioned whether ALND could be omitted in selected patients with a positive SLNB. Several retrospective studies12,13,14,15,16 have shown no significant difference in locoregional recurrence rates in patients with positive SLNs who had SLNB only compared with those who underwent ALND. There have also been prospective non-randomized studies17,18 showing similar results; however these patient cohorts were small and follow-up was less than five years.
The ACOSOG Z0011 trial is the largest prospective randomized trial thus far and it compares locoregional recurrence rates and survival in women with positive sentinel nodes treated with SLNB or ALND. This trial defined a select cohort of patients in whom completion ALND may be safely omitted as long as the patients fulfill the criteria of clinical stage T1 or T2, N0, M0 breast cancer; one or two positive SLNs; treatment with breast-conserving therapy, whole breast irradiation and adjuvant systemic therapy (chemotherapy and/or endocrine therapy).
During the past five years since the publication of Z0011, the study has been described as a practice-changing trial19. Some centers in the United States, Europe and Australia have applied Z0011 criteria to their own population and found the criteria is eligible10,20,21,22. However, in China ALND is still recommended for patients with positive SLNs according to the guideline of Breast Cancer Committee affiliated with Chinese Anti-Cancer Association23. The current study aimed to investigate the feasibility of applying the Z0011 criteria in China. To our knowledge, no other studies have addressed this question before.
It is well known that the feasibility of new practice protocol in China depends on two aspects: the subjective opinions from clinicians regarding the protocol and the clinical applicability of the protocol to Chinese patients. Therefore, our study included two parts: a survey assessing the impact of Z0011 on surgeons’ practices across China and a multi-center study analysing the clinical relevance of the Z0011 findings to Chinese breast cancer patients.
Among the 427 respondents to the survey, most surgeons came from third-grade class-A hospital (75.9%) and municipalities or provincial capitals (87.4%). In China, the training system after graduation is for clinicians from community hospitals to receive training in hospitals of high grade. We believe the answers of the 427 surgeons could represent the current pattern of breast surgery practice in our country.
Although 71.9% of the respondents had a postgraduate education background, it was disappointing that only 27.2% indicated familiarity with Z0011 trial. In a survey given to members of the American Society of Breast Surgeons (ASBrS), 97% of 849 respondents were familiar with Z00118. Another questionnaire survey distributed to members of the North Pacific Surgical Association and the Oregon and Washington chapters of the American College of Surgeons found a similar result, with 94% of surgeons being aware of Z001124.
Our survey data still indicated before Z0011’s publication, 75.2% of the respondents would perform ALND most or all of the time on patients meeting the Z0011 criteria. In western countries, some surgeons had elected to omit ALND in some patients with a positive SLN or favorable clinicopathologic characteristics prior to publication of Z001115,18,25,26. Yi et al. published data from the Surveillance, Epidemiology and End Results (SEER) database on 26,986 breast cancer patients with nodal disease treated from 1998 to 2004. Completion ALND was omitted in 16.4%13. After Z0011’s publication, many studies indicated the majority of surgeons incorporated Z0011 into practice by omitting completion ALND in patients with one or two positive SLNs undergoing BCT who were targeted for WBI7,8,10,13. Gainer et al.’s survey results showed that 468 (56.9%) respondents would infrequently or never perform completion ALND on a woman fulfilling Z0011 criteria, while 186 (22.6%) would sometimes perform completion ALND and 168 (20.4%) would perform completion ALND most or all of the time8. By contrast, our current survey data demonstrated after learning of Z0011 results from our explanation shown in the questionnaire, 69.6% of the respondnts would still perform ALND most or all of the time on patients meeting the Z0011 criteria.
It was interesting that the result of our survey demonstrated that there was no difference in the physicians’ preference for ALND after learning of Z0011, regardless of whether the physician practiced in a high-level hospital or a lower one, came from a metropolis or a small town, had a doctoral degree or only a bachelor degree, or had practiced for a longer time or a shorter time.
It seemed that the Z0011 trial did not have the same impact on Chinese surgeons’ practice as on western surgeons’8,24. Even having learned of the Z0011 results, most Chinese surgeons would much more frequently choose radical surgery for patients with positive SLNs. Although lack of detailed knowledge regarding Z0011 might affect respondents’ acceptance of Z0011 to some extent in the current study, we thought that the survey was consistent with the current management pattern for breast cancer patients with positive SLNs in China.
Although we did not survey in detail the reasons why Chinese physicians would not alter their practice mode according to Z0011 results, we could presume the main cause is because Z0011 was recently the hot topic of discussion at many breast cancer meetings in China . First, most Chinese surgeons worry about the recurrence of breast cancer if positive lymphnodes are left in the axilla. The completeness of tumour resection has been the standard for evaluating the success of surgery in our practice and recurrence at local or regional nodes would be attributed to incomplete excision. Second, in many areas of China, especially suburban areas, many patients could not undergo standard adjuvant treatment after surgery due to many reasons, including medical conditions, patient intention, economic ability, etc. Thus, many Chinese physicians would argue that the Z0011 trial does not fit China’s basic conditions. Third, there are differences in clinical characteristics between Chinese breast cancer patients and Westerners and no data about the relevance of the Z0011 criteria to Chinese patients have been reported until now. It is reasonable that Chinese physicians are uncertain as to whether western trial results are applicable to the Chinese population.
To address the third point above, we collected 658 consecutive breast cancer patients from five hospitals’ databases to examine whether following the Z0011 criteria would select patients with the same characteristics as those of the cohort included in the Z0011 trial.
At these five hospitals ALND was the standard treatment for patients with positive SLN regardless of the size of metastasis or number of positive SLNs. After applying Z0011 criteria to the 658 patients with ALND after positive SLNB, we found 151(22.9%) patients were eligible for omitting ALND. Yi et al. found 36.6% of patients with positive SLNs could have SLNB only using Z0011 criteria27. Delpech et al. found 69.6% of patients with positive SLNs met Z0011 criteria20. Authors from Memorial Sloan-Kettering Cancer Center found that 48% of patients with positive SLNB would be spared ALND if they incorporate Z0011 results into their cancer care28. The difference between our study and western ones might be mainly due to the lower rate of BCT20,27,29. In our study, 490(74.5%) patients had mastectomies and 445(67.6%) patients could not be spared ALND only because they underwent mastectomy, according to the Z0011 results.
The rate of BCT in China varies greatly among different areas and hospitals. After more than twenty years’ practice, BCT has been widly accepted across China and has become the most common surgery for breast cancer. The five hospitals attending this study could represent the highest level for breast surgery in China, but the rate of BCT in this study is lower than in other studies in western countries. The difference of BCT may mainly because of the difference of medical conditions and economic ability in China and western countries. On the other hand, Chinese patients usually having smaller size breasts than westerners may be another cause. But since the development of medical technique and economy in China, the rate of BCT would be higher in the future. Therefore, discussing the Z0011 trial’s applicability to Chinese patients will be more meaningful.
Compared with axillary clearance, SLNB is associated with significantly less morbidity, such as seroma formation, wound infection, arm dysfunction, sensory loss and lymphoedema30,31,32,33,34. So if using Z0011 findings to Chinese breast cancer patients with metastatic SLNs could make nearly one quarter of them avoiding ALND safely. This result suggests that applying Z0011 criteria to Chinese patients has great clinical meaning.
We found no significant difference in clinical characteristics including ER status, clinical stage, or number of positive LNs or positive NSLNs between our group of patients who were potentially eligible for omitting ALND according to the Z0011 criteria and the population reported in the Z0011 trial. The patients in the eligible group had more gradeII tumors than the Z0011 cohort (p = 0.001), perhaps because we classified all gradeI and gradeII mixed tumors as gradeII tumors all. This finding indicated using Z0011 results in Chinese patients could select ones with similar characteristics as the Z0011 cohort, which supports the safe exportability of the Z0011 criteria. In our comparison of the patients who were ineligible for omitting ALND with those who were eligible, the ineligible group had a significantly higher percentage of patients with later stage tumors and advanced disease in the axilla. This result demonstrated that the Z0011 criteria might discriminate patients with a high risk of recurrence and metastasis from those with a low risk and it confirms the importance of the strict adherence to the Z0011criteria in China.
However, there has been some criticism on Z001135,36. The trial had a potential bias related to the enrolment of only patients with a good prognosis and it was closed early with less than 50% target accrual. There were also high survival and low event rates (only 92 events for the trial) and a large number of women in both groups were lost to follow up—21% in the axillary dissection group and 17% in the SLNB group. Lastly, the radiation techniques were not described, including dosing, frequency and field definitions. While many centers have changed their treatment pattern according to Z0011 results and acquired similar survival rate as Z0011 trial10,20,27. It is important that future trials should focus on groups excluded from Z0011, such as patients undergoing neoadjuvant chemotherapy or neoadjuvant hormonal therapy, mastectomy, or radiation modalities other than WBI37.
The major limitation of our study is that we could only collect retrospective data because ALND is the standard treatment for patients with positive SLNs. The results of our study indicat good applicability of Z0011criteria in Chinese Patients and we need further data on the application of the Z0011 criteria in China.
From the results of our survey, we conclude that time is to be needed before the Z0011 criteria becomes the standard guideline in China. The same as the acceptance of BCT and SLNB in China, it will require a process of development. We should first begin to incorporate Z0011 into our practice in hospitals with suitable medical conditions, such as the five hospitals participating in this study. The five hospitals have played a leading role in the breast surgery field in China and we believe that changes in practice at these five hospitals would have a strong impact on others. In addition, more introduction and explanation of Z0011 trial to more Chinese physicians through meeting, press and the Internet would help to make it more acceptable in China.
We think the results of our current multicenter study offer data regarding our own population and may influence Chinese surgeons to incorporate the Z0011 criteria into their practice.
Additional Information
How to cite this article: Liu, M. et al. The feasibility of the ACOSOG Z0011 Criteria to Chinese Breast Cancer Patients: A Multicenter Study. Sci. Rep. 5, 15241; doi: 10.1038/srep15241 (2015).
References
Krag, D. N. et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 11, 927–933 (2010).
Veronesi, U. et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med. 349, 546–553 (2003).
Posther, K. E. et al. Sentinel node skills verification and surgeon performance: data from a multicenter clinical trial for early-stage breast cancer. Ann Surg. 242, 593–599 (2005).
Giuliano, A. E. et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA . 305, 569–575 (2011).
Giuliano, A. E. et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 252, 426–432 (2010).
National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Breast, version 1.2012. Available at: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. (Accessed: 18th September 2012).
Caudle, A. S. et al. Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: A practice changing trial. Ann Surg Oncol. 18, 2407–2412 (2011).
Gainer, S. M. et al. Changing behavior in clinical practice in response to the ACOSOG Z0011 trial: A Survey of the American Society of Breast Surgeons. Ann Surg Oncol . 19, 3152–3158 (2012).
Caudle, A. S. et al. American College of Surgeons Oncology Group (ACOSOG) Z0011: Impact on surgeon practice patterns. Ann Surg Oncol. 19, 3144–3151 (2012).
Dengel, L. T. et al. Axillary dissection can be avoided in the majority of clinically node-negative patients under going breast-conserving therapy. Ann Surg Oncol. 21, 22–27 (2014).
Liu, M. et al. A new model for predicting non-sentinel lymph node status in Chinese sentinel lymph node positive breast cancer patients. PLoS One. 9, e104117 (2014).
Fant, J. S. et al. Preliminary outcome analysis in patients with breast cancer and a positive sentinel lymph node who declined axillary dissection. Ann Surg Oncol. 10, 126–130 (2003).
Yi, M. et al. Trends in and outcomes from lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database. Ann Surg Oncol. 17, S343–351 (2010).
Bilimoria, K. Y. et al. Comparison of sentinel lymph node biopsy alone and completion axillary lymph node dissection for node-positive breast cancer. J Clin Oncol. 27, 2946–2953 (2009).
Hwang, R. F. et al. Low locoregional failure rates in selected breast cancer patients with tumor-positive sentinel lymph nodes who do not undergo completion axillary dissection. Cancer. 110, 723–730 (2003).
Francissen, C. M. et al. Axillary recurrence after a tumorpositive sentinel lymph node biopsy without axillary treatment: a review of the literature. Ann Surg Oncol. 19, 4140–4149 (2012).
Guenther, J. M. et al. Axillary dissection is not required for all patients with breast cancer and positive sentinel nodes. Arch Surg. 138, 52–56 (2003).
Jeruss, J. S. et al. Axillary recurrence after sentinel node biopsy. Ann Surg Oncol. 12, 34–40 (2005).
Caudle, A. S. et al. Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: a practice changing trial. Ann Surg Oncol. 18, 2407–2412 (2011).
Delpech, Y. et al. The exportability of the ACOSOG Z0011 criteria for omitting axillary lymph node dissection after positive sentinel lymph node biopsy findings: a multicenter study. Ann Surg Oncol. 20, 2556–2561 (2013).
Aigner, J. et al. Omission of axillary dissection according to ACOSOG Z0011: impact on adjuvant treatment recommendations. Ann Surg. 20, 1538–1544 (2013).
Ngui, N. K., Elder, E. E., Jayasinghe, U. W. & French, J. Relevance of the American College of Surgeons Oncology Group Z0011 Trial to breast cancer in the Australian setting. ANZ J Surg . 83, 924–928 (2013).
Breast Cancer Committee of China Anti-Cancer Association. Guidelines in breast caner diagnosis and treatment of China Anti-Cancer Association (version 2013). Zhongguo Ai Zheng Za Zhi. 23, 639-696 (2013).
Massimino, K. P., Hessman, C. J., Ellis, M. C., Naik, A. M. & Vetto, J. T. Impact of American College of Surgeons Oncology Group Z0011 and National Surgical Adjuvant Breast and Bowel Project B-32 trial results on surgeon practice in the Pacific Northwest. Am J Surg. 203, 618–622 (2012).
Barkley, C. et al. Can axillary node dissection be omitted in a subset of patients with low local and regional failure rates? Breast J. 18, 23–27 (2012).
Galimberti, V. et al. Can we avoid axillary dissection in the micrometastatic sentinel node in breast cancer? Breast Cancer Res Treat. 131, 819–825 (2012).
Yi, M. et al. Impact of the american college of surgeons oncology group Z0011 criteria applied to a contemporary patient population. J Am Coll Surg. 216, 105–113 (2013).
Weber, W. P. et al. A 10-year trend analysis of sentinel lymph node frozen section and: are these procedures becoming obsolete? Ann Surg Oncol. 19, 225–232 (2012).
Hiotis, K. et al. The importance of location in determining breast conservation rates. Am J Surg. 190, 18–22 (2005).
Gill, G. SNAC Trial Group of the Royal Australasian College of Surgeons (RACS) and NHMRC Clinical Trials Centre.Sentinel-lymph-node-based management or routine axillary clearance? One-year outcomes of sentinel node biopsy versus axillary clearance (SNAC): a randomized controlled surgical trial. Ann Surg Oncol. 16, 266–275 (2009).
Mansel. R. E. et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst. 98, 599–609 (2006).
Feldman, S. M. & Sweatman, C. A. Jr. Sentinel node biopsy for breast cancer: past, present and future (editorial). Ann Surg Oncol . 19, 3123–3124 (2012).
Haffty, B. G., Hunt, K. K., Harris, J. R. & Buchholz, T. A. Positive sentinel nodes without axillary dissection: implications for the radiation oncologist. J Clin Oncol. 29, 4479–81 (2011).
Lucci, A. et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 25, 3657–3663 (2007).
Latosinsky, S. et al. Axillary dissection versus no axillary dissection in women with invasive breast cancer and sentinel node metastases. Can J Surg. 55, 66–69 (2012).
Jatoi, I. Axillary vs sentinel lymph node dissection for invasive breast cancer. JAMA . 305, 2288 (2011).
Morrow, M. & Giuliano, A. E. To cut is to cure: can we really apply Z0011 in practice? Ann Surg Oncol. 18, 2413–2415 (2011).
Acknowledgements
The authors thank Dr. Dingbao Chen for his technical assiatance from the Department of Pathology, People’s Hospital, Peking University.
Author information
Authors and Affiliations
Contributions
M.L. and S.W. conceived and designed the study. S.D.C., X.N.D., Z.M.F. and Z.G.Y. contributed the materials and analyzed the data. M.L. wrote the main manuscript text. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Liu, M., Wang, S., Cui, S. et al. The feasibility of the ACOSOG Z0011 Criteria to Chinese Breast Cancer Patients: A Multicenter Study. Sci Rep 5, 15241 (2015). https://doi.org/10.1038/srep15241
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep15241
This article is cited by
-
Impact of the ACOSOG Z0011 trial on surgical practice in Asian patients: trends in axillary surgery for breast cancer from a Korean Breast Cancer Registry analysis
World Journal of Surgical Oncology (2022)
-
Comparing single or dual tracing modality on sentinel lymph node biopsy from patients who plan to omitting axillary lymph node dissection referring to the criteria of Z0011 trial: a retrospective study
Updates in Surgery (2022)
-
Application of the ACOSOG Z0011 criteria to Chinese patients with breast cancer: a prospective study
World Journal of Surgical Oncology (2021)
-
Trends in Axillary Management of Early Breast Cancer: a Questionnaire-Based Pattern of Practice Survey for India
Indian Journal of Surgical Oncology (2021)
-
Using the axillary reverse mapping technique to screen breast cancer patients with a high risk of lymphedema
World Journal of Surgical Oncology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
