
Abstract
Study design:
Case report of a severe upper cervical cord compression and tetraparesis by a massive cervical exostotic osteochondroma in a patient with multiple exostoses–mental retardation syndrome (Langer–Giedion syndrome; LGS).
Objective:
To describe this very rare pathological condition and the results of surgical intervention.
Setting:
Gifu, Japan.
Methods:
A 23-year-old man was referred to our clinic because of progressing tetraparesis. He had previously been diagnosed with hereditary multiple exostoses and mental retardation. As he had not complained of any symptoms, his family only noticed the tetraparesis after advanced deterioration. His face possessed the pathognomic features of LGS. A postmyelogram CT scan demonstrated an exostotic mass arising from the left-side C2 pedicle with associated severe spinal cord compression. He was diagnosed with LGS. Hemilaminectomy on the left side and resection of the osteochondroma were performed.
Results:
At 5 years postoperatively, a neurological examination showed the full return of all motor functions. The CT scan revealed no intracanalar recurrence of the tumor.
Conclusion:
In this case of severe tetraparesis due to cervical osteochondroma, decompression by hemilaminectomy provided excellent results. In patients with LGS and intracanalar osteochondroma, the neurological deficit may be masked by mental retardation. Hence, awareness of this pathological condition will help clinicians diagnose it at an early stage.
Similar content being viewed by others


Introduction
Hereditary multiple exostoses1 is a condition characterized by anomalous skeletal development with multiple exostotic osteochondromas frequently occurring from the metaphyseal regions of long bones, iliac crests, and scapulas. The vertebral column is involved in approximately 7% of patients with hereditary multiple exostoses.2 Several cases with the development of an osteochondroma in the spinal canal, hereafter referred to as intracanalar osteochondroma, and spinal cord compression have been reported as relatively rare pathological conditions.3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13
Multiple exostoses are also a cardinal feature of trichorhinophalangeal syndrome (TRP) type II (Langer–Giedion syndrome),14 which includes mental retardation and peculiar facial features.14, 15, 16, 17, 18, 19, 20 We report a very rare case of tetraparesis, due to an intracanalar osteochondroma at the upper cervical spine in a patient with Langer–Giedion syndrome (LGS), which was successfully treated by surgery. This is the first case report of spinal exostotic osteochondroma and spinal cord compression associated with LGS in the literature.
Case report
A 23-year-old man was admitted to our department in January 1998 for tetraparesis. Two months before, he became unable to walk after a gradual decline. During his childhood, he had absence epilepsy. Multiple bony deformities were noted since he was 9 years old. He was mentally retarded. His father had bony prominences in his ankles, although the details were not known. As he had not complained of the motor disturbances, his family only noticed his condition after it had deteriorated.
On admission, his height was 158 cm and his head was relatively small. His face (Figure 1) was unusual with large, laterally protruded ears, an elongated philtrum, thin upper lip, teeth malformations, and heavy eyebrows. Bony tumors were palpated at the occipital lesion and in the peri-articular areas of the upper and lower extremities. There was percussion pain at the midline of the upper cervical spine. Hyperelasticity of the skin and joint laxity was not observed. His IQ measured 42 and he had a marked disturbance in his speech.

The patient's face was unique with large, laterally protruded ears (black arrows), elongated philtrum, thin upper lip, teeth malformations, and heavy eyebrows
The neurological examination disclosed spastic tetraparesis, with his manual muscle test at grade two to three below the bilateral C4 level. Sensory disturbances were present in the right hand. In addition, hyper-reflexia and pathological reflexes of the lower extremities and urinary incontinence were noted. Since his fine motor abilities in his fingers were remarkably deteriorated, he could not use chopsticks or other eating utensils with his hands.
Radiological studies disclosed numerous exostoses at the distal ends of the bilateral humeri, radii, ulnae, femurs, tibiae, fibulae, and metatarsal bones, as well as the occiput and the right-side sacroiliac joint. On plain X-ray film of the hands (Figure 2), cone-shaped epiphyses were demonstrated at the proximal phalanges of the fingers. Plain X-ray film of the cervical spine (Figure 3) showed irregular sclerotic changes at C2–C3. Myelography demonstrated a complete block of cerebrospinal fluid at the second cervical level. A postmyelogram CT scan (Figure 4) demonstrated an exostotic mass arising from the left-side C2 pedicle that severely compressed the spinal cord. The diagnosis was upper cervical cord compression due to exostotic osteochondroma at C2 with associated LGS. Because the tetraparesis was progressing, we indicated a surgical treatment for him.

On plain X-ray film of the hands, cone-shaped epiphyses are demonstrated at metacarpals and phalanges. Exostoses at the distal portions of the bilateral radii are noted (black arrow)

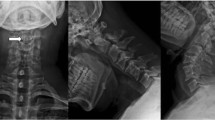
Plain cervical spine radiograph showed irregular sclerotic changes at C2-C3 (white arrow)

Postmyelogram CT scan demonstrated an exostotic mass arising from the left-side C2 pedicle with associated severe spinal cord compression
Surgical treatment
At 1 month after his admission, a hemilaminectomy was performed, using an air-drill, on the left side from the inferior half of C1 to the superior half of C3. The muscles attaching to the spinosus processus of the C2, such as semispinalis cervicis, were preserved. The intracanalar portion of the tumor compressing the spinal cord was then resected. We did not resect the anterior part of the tumor, which would have required an anterior or lateral approach.
The histological examination of the tumor specimen revealed the typical characteristics of osteochondroma with a thick cartilage cap. The postoperative CT scan (Figure 5) showed sufficient decompression. Spastic tetraparesis improved gradually and the patient regained the ability to walk without a cane 2 months after the operation. At 5 years postoperatively, plain X-ray film of the cervical spine showed no sign of subsequent kyphosis or instability. The CT scan (Figure 6) did not reveal intracanalar recurrence of the tumor, but there was further growth of the anterior residual mass. An approval for reporting this illness including the features of appearance to the scientific literature was obtained from the patient.

A postoperative CT demonstrated sufficient decompression by the excision of the intracanalar portion of the tumor

A CT scan at the 5-year follow-up demonstrated no intracanalar recurrence of the tumor but a further growth of the extracanalar portion of the tumor (white arrows)
Discussion
LGS,14 characterized by the combination of multiple exostoses and mental retardation,14, 15, 16, 17, 18, 19, 20 is a very rare contiguous gene-deletion syndrome21 caused by the simultaneous deletion of the EXT1 and TRPS1 genes on choromosome 8q24.22 The characteristics of the present patient, including multiple exostoses, mental retardation, short stature, small head, unusual facial appearance, and cone-shaped epiphyses of the hands, sufficiently fulfilled all the major criteria of this disease,14, 19, 20 except for a bulbous nose. Recently, patients with clinical features very similar to LGS, but with epilepsy, were reported by two authors23, 24 as a different criteria from LGS. The lack of a chromosome analysis and the past history of epilepsy in this patient make a definite diagnosis difficult. In any case, the combination of multiple exostoses, mental retardation, and tetraparesis due to intracanalar osteochondroma has not been previously reported in the literature.
Surgical treatments have been indicated for intracanalar osteochondroma, which is associated with myelopathy,2, 3, 4, 5, 6, 7, 12, 13 radiculopathy,8 insufficiency of the vertebral artery,25 and neck pain.2 From various other possible surgical procedures, laminectomy was chosen by a majority of authors.2, 3, 4, 5, 6 Then, to avoid the risk of postlaminectomy kyphosis26, 27 and subsequent instability26 as complications of laminectomy for the cervical spine, the use of posterior stabilization and posterolateral fusion,7 anterior stabilization and fusion,9 and laminoplasty12 were reported. As a less invasive procedure, we chose hemilaminectomy28 for this patient. The excision of the intracanalar portion of the tumor was successfully performed and neurological recovery at the 5-year follow-up was excellent without subsequent problems. However, as we did not resect the anterior part of the tumor, it manifested growth at the 5-year follow-up. Taking into account the incidence of malignant transformation of the exostoses in hereditary multiple exostosis,29 this patient requires careful monitoring and further therapeutic treatments should be considered.
The clinically important lesson from this patient with LGS is that his tetraparesis was not recognized, presumably because of his mental retardation, until it became severe. Indeed, his intracanalar tumor is among the largest described in the literature. Awareness of this pathological condition would help clinicians make an early and correct diagnosis.
Conclusion
We reported a case of severe upper cervical cord compression and tetraparesis by a massive cervical exostotic osteochondroma in a patient with multiple exostoses–mental retardation syndrome (LGS). For this case of severe tetraparesis, decompression by hemilaminectomy provided an excellent result.
References
Jaffe HL . Hereditary multiple exostoses. Arch Pathol 1943; 36: 335–357.
Carmel PW, Cramer FJ . Cervical cord compression due to exostosis in a patient with hereditary multiple exostoses. Case report. J Neurosurg 1968; 28: 500–503.
Ochsner EH, Rothstein T . Multiple exostosis including an exostosis within spinal canal with surgical and neurological observation. Ann Surg 1907; 46: 608–616.
Roman G . Hereditary multiple exostoses. A rare cause of spinal cord compression. Spine 1978; 3: 230–233.
O'Connor GA, Roberts TS . Spinal cord compression by an osteochondroma in a patient with multiple osteochondromatosis. Case report. J Neurosurg 1984; 60: 420–423.
Shapiro SA, Javid T, Putty T . Osteochondroma with cervical cord compression in hereditary multiple exostoses. Spine 1990; 15: 600–602.
Bhojraj SY, Panjwani JS . A new management approach to decompression, posterior stabilization, and fusion for cervical laminar exostosis with cord compression in a case of diaphyseal aclasis. Case report and review of the literature. Spine 1993; 18: 1376–1379.
Arasil E, Erdem A, Yuceer N . Osteochondroma of the upper cervical spine. A case report. Spine 1996; 21: 516–518.
Ergun R et al. Cervical laminar exostosis in multiple hereditary osteochondromatosis: anterior stabilization and fusion technique for preventing instability. Eur Spine J 1997; 6: 267–269.
Tang WM, Luk KD, Leong JC . Costal osteochondroma. A rare cause of spinal cord compression. Spine 1998; 23: 1900–1903.
Govender S, Parbhoo AH . Osteochondroma with compression of the spinal cord. A report of two cases. J Bone Joint Surg Br 1999; 81: 667–669.
Oga M et al. Treatment of cervical cord compression, caused by hereditary multiple exostosis, with laminoplasty: a case report. Spine 2000; 25: 1290–1292.
Mermer MJ et al. Thoracic vertebral body exostosis as a cause of myelopathy in a patient with hereditary multiple exostoses. J Spinal Disord Tech 2002; 15: 144–148.
Hall BD et al. Langer–Giedion syndrome. Birth Defects Orig Artic Ser 1974; 10: 147–164.
Ale G, Calo S . Su di un caso di disostosi periferia associate con estosi osteogeniche multiple ed ipsomia disuniforme e disarmonica. Ann Radiol 1961; 34: 376–385.
Kozlowski K et al. Multiple exostoses–mental retardation syndrome (Ale-Calo or M.E.M.R. syndrome). Clin Pediatr (Phila) 1977; 16: 219–224.
Stoltzfus E, Ladda RL, Lloyd-Still J . Langer–Giedion syndrome: type II tricho-rhino-phalangeal dysplasia. J Pediatr 1977; 91: 277–280.
Wilson WG, Herrington RT, Aylsworth AS . The Langer–Giedion syndrome: report of a 22-year old woman. Pediatrics 1979; 64: 542–545.
Miki T et al. Multiple exostoses–mental retardation (MEMR) syndrome: report of a case. Clin Orthop 1980; 207–210.
Mirovsky Y et al. Multiple exostoses–mental retardation syndrome. A case report and review of the literature. Clin Orthop 1984; 72–76.
Ludecke HJ et al. Molecular dissection of a contiguous gene syndrome: localization of the genes involved in the Langer–Giedion syndrome. Hum Mol Genet 1995; 4: 31–36.
Momeni P et al. Mutations in a new gene, encoding a zinc-finger protein, cause tricho-rhino-phalangeal syndrome type I. Nat Genet 2000; 24: 71–74.
Volpi N et al. Familial multiple exostoses syndrome: a phacomatosis of bone tissue. Acta Neurol (Napoli) 1986; 8: 516.
Wuyts W et al. Multiple exostoses, mental retardation, hypertrichosis, and brain abnormalities in a boy with a de novo 8q24 submicroscopic interstitial deletion. Am J Med Genet 2002; 113: 326–332.
George B, Atallah A, Laurian C, Tayon B, Mikol J . Cervical osteochondroma (C2 level) with vertebral artery occlusion and second cervical nerve root irritation. Surg Neurol 1989; 31: 459–464.
McLaughlin MR, Wahlig JB, Pollack IF . Incidence of postlaminectomy kyphosis after Chiari decompression. Spine 1997; 22: 613–617.
Matsunaga S, Sakou T, Nakanisi K . Analysis of the cervical spine alignment following laminoplasty and laminectomy. Spinal Cord 1999; 37: 20–24.
Khosla A, Martin DS, Awwad EE . The solitary intraspinal vertebral osteochondroma. An unusual cause of compressive myelopathy: features and literature review. Spine 1999; 24: 77–81.
Schmale GA, Conrad III EU, Raskind WH . The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994; 76: 986–992.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Miyamoto, K., Sakaguchi, Y., Hosoe, H. et al. Tetraparesis due to exostotic osteochondroma at upper cervical cord in a patient with multiple exostoses–mental retardation syndrome (Langer–Giedion syndrome). Spinal Cord 43, 190–194 (2005). https://doi.org/10.1038/sj.sc.3101690
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101690
Keywords
This article is cited by
-
Spinal stenosis frequent in children with multiple hereditary exostoses
Journal of Children's Orthopaedics (2013)
-
Cervical osteochondroma with postoperative recurrence: case report and review of the literature
Child's Nervous System (2010)
