
Abstract
Study design: Determination of fat oxidation at three different intensities in trained wheelchair athletes on the treadmill.
Objective: The aim of the study was to assess the level and highest rate of fat oxidation in endurance-trained wheelchair athletes for recommendation on endurance training.
Setting: Institute of Sports Medicine, Swiss Paraplegic Centre, Nottwil, Switzerland.
Methods: Nine (seven men and two women) endurance-trained wheelchair athletes (VO2peak 40.2±6.7 ml/kg/min) were studied over 20 min at 55, 65 and 75% VO2peak on a treadmill in their own racing wheelchairs in order to find the exercise intensity with the highest absolute fat oxidation.
Results: As presumed, total energy expenditure for wheelchair racing was highest at 75% VO2peak, while absolute fat oxidation was statistically not significantly different at the three tested intensities. Percentage of energy expenditure from fat oxidation decreased with increasing intensity from 31.4% at 55% VO2peak to 20.9% at 75% VO2peak, while percentage from carbohydrate oxidation increased from 68.6% at 55% VO2peak to 79.1% at 75% VO2peak.
Conclusion: For wheelchair athletes, we recommend training of fat metabolism for endurance exercise at an intensity of 55% VO2peak, because absolute fat metabolism is not higher at higher intensities but less carbohydrates are used at lower intensity levels. At lower intensities, exercise can be performed over a longer time before the emptied glycogen stores will limit exercise duration. This may apply especially to paraplegic subjects whose active muscle mass is limited in contrast to able-bodied athletes.
Similar content being viewed by others

Introduction
It is generally recommended to perform endurance training at low to moderate intensities in order to stimulate maximally fat oxidation which in turn improves performance in long-distance exercise. At moderate intensities, lipolysis of subcutaneous fat is enhanced,1 while it is limited at high intensities of approximately 80–85% of maximal oxygen consumption (VO2max).2,3 Recent studies revealed that the optimal intensity for fat oxidation is at rather high intensities of 65 to 75% VO2max in endurance-trained athletes.3,4 In earlier years, Romijn et al1 showed that endurance-trained men have their highest fat oxidation rate at 65% VO2max. They recently performed the same protocol with endurance-trained women and confirmed their prior results showing the highest fat oxidation at 65% VO2max.4 Different results were found by Astorino,3 who showed that endurance-trained women have their highest fat oxidation rate at 75% of peak oxygen consumption (VO2peak). The different results in the studies of Romijn et al4 and Astorino3 may have been a consequence of the chosen type of exercise. Romijn and co-workers performed their studies on a cycling ergometer, while Astorino employed running on a treadmill. In more recent studies, highest fat oxidation rate is presumed to be at even lower intensities of 57% VO2max,5 respectively, 65% V02max.6
Nevertheless, results of able bodied athletes cannot completely be transferred to wheelchair exercise. They have to be tested for the different types of exercise and type of disability.7 In spinal cord-injured (SCI) people, there is evidence that mobilisation of free fatty acids from subcutaneous tissue is lower, and glucose meta-bolism is increased compared to able-bodied people.8 One reason could be the smaller muscle mass involved and the type of exercise. All the same, people with SCI respond to exercise training in essentially the same manner as nonhandicapped persons and can also achieve improvements in exercise performance.9,10 In trained paraplegic athletes, maximal oxygen consumption can reach nearly the same levels as in able-bodied persons.11 Also Gass et al12 reported that paraplegics can exercise at approximately 50% VO2max for 60 min, producing responses similar to those in able-bodied subjects. However, there is no study performed with paraplegics concerning fat metabolism and intensity.
The aim of this study was to assess the level and highest rate of fat oxidation in endurance-trained wheelchair athletes. Knowledge of the intensity with the highest fat oxidation is important for recommendations in endurance training. Owing to the fact that in endurance-trained able-bodied athletes, highest fat oxidation is presumed at rather high intensities from 65 to 75% VO2max, we compared fat oxidation at the three intensities of 55, 65 and 75% VO2peak in wheelchair racing athletes.
Subjects and methods
Subjects
A total of nine endurance-trained wheelchair athletes participated in the study. These athletes consisted of five with paraplegia, one with tetraplegia, two with spina bifida and one with poliomyelitis (Table 1). All athletes completed regular training in wheelchair racing and were active athletes at either national or international level. The study was approved by the local ethics committee and all subjects gave their written informed consent prior to testing.
VO2peak test
At 1 day to 2 weeks prior to the endurance tests, subjects referred to the laboratory for a VO2peak test. Wheelchair athletes were tested on their racing wheelchairs that were fixed on a treadmill (Saturn HP Cosmos, München, Germany) with a mobile lever arm. Exercise protocol started at a speed of 10 km/h and an inclination of 0.7%. Every 3 min, speed increased for 2 km/h, while inclination remained constant. At the end of every step, capillary blood was taken from the earlobe to measure concentration of lactate by an enzymatic method (Super GL ambulance, Ruhrtal Labor Technik, Möhnesee, Germany). Before each measurement of lactate, the analyser was calibrated with a 10 mmol/l lactate standard solution. During exercise, oxygen uptake (VO2) and carbon dioxide production (VCO2) were measured continuously (Oxycon α, Jaeger, Würzburg, Germany). Gas analysers were calibrated prior to each test.
Heart rate was measured continuously and reported at the end of each incremental step (Polar M52, Kempele, Finland).
Endurance tests
Between 1 and 14 days after the VO2peak tests, subjects returned for the endurance tests. The evening before the test, all subjects were told to eat a carbohydrate-rich meal with 70 kJ carbohydrates/kg bodyweight without fat in order to load muscle glycogen. After an overnight fast, they reported to the laboratory at 8 am. They completed an endurance test in their racing wheelchair. The endurance test consisted of three stages of 20 min at 55, 65 and 75% VO2peak, which was calculated for each individual from the results of the VO2peak test. Between each intensity stage, they had a rest of 15 min and were allowed to drink tap-water ad libitum. Immediately before the beginning of each intensity stage and every following 10 min during the test, heart rate and concentration of lactate were measured. A 20 μl capillary of glass was filled with blood from the earlobe to assess the concentration of lactate. During the 20 min, VO2 and VCO2 were continuously calculated from inspiratory oxygen concentration (FIO2), expiratory oxygen concentration (FEO2) and ventilation (VE). Workload was adjusted in the first 5 min to reach the preset percentage of VO2peak.
Indirect calorimetry and calculations
VO2 and VCO2 from the last 10 min of each step were used to calculate the rate of the oxidised substrate. Oxidation rate of fat and carbohydrate were calculated using the stochiometric equations of Frayn,13 where oxidation of carbohydrates is 4.55 × VCO2−3.21 × VO2−2.87n and oxidation of fat is 1.67 × VO2−1.67 × VCO2−1.92n. According to the study of Romijn et al,4 nitrogen excretion rate (n) was assumed to be 135 μg/kg/min. Energy expenditure from fat and carbohydrate were converted to kcal/min by multiplying the oxidation rate of fat with 9.1 and the oxidation rate of carbohydrate with 4.2 using the Atwater general conversion factor.14
Statistical analysis
ANOVAs were performed to detect statistically signi-ficant differences between 55, 65, and 75% of VO2peak for the following parameters: carbohydrate oxidation, fat oxidation and total energy expenditure as well as lactate concentrations. Probability level for statistical significance was set at 0.05. A paired t-test (Bonferroni) between the intensity levels of 55 and 65% as well as between 65 and 75% was performed for significant ANOVAs to localise the significant differences.
Results
Subjects and VO2peak tests
Anthropometric data and handicap specifications of the subjects are shown in Table 1. Results of the VO2peak test are listed in Table 2.
Endurance tests
Mean values with standard deviations for oxygen uptake, heart rate, fat and carbohydrate oxidation as well as lactate concentrations for the three tested intensities are presented in Table 3.
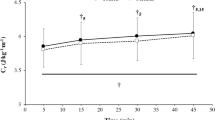
Total energy expenditure as well as energy expenditure separated into carbohydrate and fat oxidation for the three tested intensities are shown in Figure 1. Percentage of energy expenditure from fat oxidation decreased with increasing intensity from 31.4±14.4% at 55% VO2peak to 25.0±12.9% at 65% VO2peak and 20.9±15.4% at 75% VO2peak. However, percentage from carbohydrate oxidation increased from 68.6± 14.4% at 55% VO2peak to 75±12.9% at 65% VO2peak and 79.1±15.4% at 75% VO2peak.

Total energy expenditure as well as energy expenditure from fat and carbohydrate oxidation at the three different exercise intensities expressed as percent of VO2peak. Results are shown as means±SD
At the lowest intensity, oxygen uptake was 1270±290 ml/min, which corresponded to 54.2±4.2% VO2peak. At the medium intensity of 64.9±3.4% VO2peak, mean oxygen uptake was 1511±309 ml/min and at the highest intensity of 74.4±6.5% VO2peak, mean oxygen uptake was 1730±337 ml/min.
Mean heart rate was at 55% VO2peak 132±14 bpm. This corresponded to 73±5% of maximal heart rate in the VO2peak test. At 65% VO2peak, mean heart rate was 146±13 bpm and 81±5% of the maximal heart rate in the VO2peak test. At the highest tested intensity of 75% VO2peak mean heart rate rose to 156±12 bpm, which corresponded to 87±4% of the mean maximal heart rate.
Discussion
The main finding of this study was that fat oxidation in wheelchair cycling does, in contrast to running or cycling,3,4 not differ between the exercise intensities of 55 and 75% VO2peak, but carbohydrate and thus also energy expenditure are significantly higher at higher intensity levels.
These are important findings for training or dietary recommendations for endurance-trained wheelchair athletes. In able-bodied athletes, fat metabolism is important in endurance competitions on one hand due to a glycogen sparing effect and on the other hand because they have to accelerate their own body weight and fat is much lighter. These two aspects are important exercise limiting factors. Especially paraplegic athletes with high lesion levels have very small stores of muscle glycogen due to the reduced active muscle mass involved in exercise. Therefore, exercise time on high intensities, where much glycogen is needed, is shortened compared to able-bodied athletes. The better the fat metabolism of such athletes is, the longer they can maintain a higher power output. Even in able-bodied athletes, glycogen stores will be emptied at an intensity of 80% VO2max in about 90–180 min.15 At this intensity, 80% of the energy derives from carbohydrate oxidation16 of the muscle glycogen, and the oxidation of intramuscular trigly-cerides is inhibited.17
One possible reason that fat oxidation rates remain constant between 55 and 75% VO2peak could be the production of lactic acid.
This seems to play an important role in the inhibition of oxidation of circulating fatty acids in plasma, even though the antilipolytic influence of lactate on lipolysis of subcutaneous tissue has not been shown in trained athletes.18
A further reason for the inhibition of fat oxidation is the inhibition of mobilisation of long-chain fatty acids of the subcutaneous tissue,19 the limited entry of long-chain fatty acids into the mitochondria for oxidation2 and the inhibition of the oxidation of intramuscular triglycerides17 at high intensities.
Another fact to be considered is the composition of the working muscle mass based on fractions of type I and II fibres. Extensive endurance training may enhance the glycolytic capacity in both type I and II fibres, although the glycolytic capacity of the muscle as a whole generally is low in endurance-trained subjects owing to a predominance of type I fibres.20 Endurance performance is impaired by large type II fibres with greater production and reduced removal of lactate.21 In the anterior portion of the deltoid muscle, which is active in the propulsion of the wheelchair, there are more type I fibres in persons with SCI. The ratios have been found to be 42% type I fibres in able-bodied subjects, 57% in persons with paraplegia and even 74% in persons with tetraplegia.22
It is plausible that also other muscles active in wheelchair propulsion of wheelchair athletes are endurance trained and should therefore have a higher percentage of type I fibres than the corresponding muscles in able-bodied athletes and fat metabolism consequently should be enhanced compared with sedentary SCI.
The calculations of energy expenditure shown in Figure 1 give some indication on energy needed during training or competitions in wheelchair cycling. This can be helpful for recommendations of specific nutrition so that wheelchair athletes can assure a sufficient carbo-hydrate intake before long-racing distances. However, due to the fact that interindividual differences are rather large (see standard deviations) for high-level athletes, we recommend to make calculations based on their own values and to use our findings only to make a rough estimate.
Conclusion
For wheelchair athletes, we recommend training of fat metabolism and long-distance exercise around 55% of VO2peak, because fat metabolism is not higher at higher intensities of 65 to 75% VO2peak but less glycogen is needed at lower intensity levels. This allows a longer training duration since exercise duration, especially in paraplegic subjects, is impaired by limited glycogen stores.
References
Romijn JA et al. Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am J Physiol 1993; 265: E380–E391.
Sidossis LS, Gastaldelli A, Klein S, Wolfe RR . Regulation of plasma fatty acid oxidation during low- and high-intensity exercise. Am J Physiol 1997; 272: E1065–E1070.
Astorino TA . Is the ventilatory threshold coincident with maximal fat oxidation during submaximal exercise in women? J Sports Med Phys Fitness 2000; 40: 209–216.
Romijn JA, Coyle EF, Sidossis LS, Rosenblatt J, Wolfe RR . Substrate metabolism during different exercise intensities in endurance-trained women. J Appl Physiol 2000; 88: 1707–1714.
Van Loon JJC, Greenhaff PL, Constantin-Teodosiu D, Saris WHM, Wagenmakers AJM . The effects of increasing exercise intensity on muscle fuel utilisation in humans. J Physiol 2001; 536: 295–304.
Achten J, Gleeson M, Jeukendrup AE . Determination of the exercise intensity that elicits maximal fat oxidation. Med Sci Sports Exerc 2002; 34: 92–97.
Schmid A . Rollstuhlergometrie. Dtsch Z Sportmed 2002; 53: 153–154.
Kjaer M et al. Fatty acid kinetics and carbohydrate metabolism during electrical exercise in spinal cord-injured humans. Am J Physiol 2001; 281: R1492–R1498.
Cowell LL, Squires WG, Raven PB . Benefits of aerobic exercise for the paraplegic: a brief review. Med Sci Sports Exerc 1986; 18: 501–508.
Hoffmann MD . Cardiorespiratory fitness and training in quadriplegics and paraplegics. Sports Med 1986; 3: 312–330.
Huonker M, Schmid A, König D, Mrosek P, Keul J . Trainingsinduzierte Adaptation des Herz-Kreislauf-Systems bei querschnittgelähmten Rollstuhlfahrern. Schweiz Z Sportmed Sporttrauma 1996; 44: 19–23.
Gass GC, Camp EM, Davis HA, Eager D, Grout L . The effects of prolonged exercise on spinally injured subjects. Med Sci Sports Exerc 1981; 13: 277–283.
Frayn KN . Calculation of substrate oxidation rates in vivo from gaseous exchange. J Appl Physiol 1983; 55: 628–634.
Atwater WO . Coefficients of digestibility and availability of the nutrients of food. Proc Am Physiol Soc 1909; 30: 14–19.
Coyle EF . Substrate utilisation during exercise in active people. Am J Clin Nutr 1995; 61(Suppl) S968–S979.
Pirnay F, Scheen AJ, Gautier JF, Lacroix M, Mosora F, Lefebvre P . Exogenous glucose oxidation during exercise in relation to the power output. Int J Sports Med 1995; 16: 456–460.
Brechtel K et al. Utilisation of intramyocellular lipids (IMCLs) during exercise as assessed by proton magnetic resonance spectroscopy (1H-MRS). Horm Metab Res 2001; 33: 63–66.
Trudeau F, Bernier I, De Glisezinsky F, Crampes F, Dulac F, Riviere D . Lack of antilipolytic effect of lactate in subcutaneous abdominal adipose tissue during exercise. J Appl Physiol 1999; 86: 1800–1804.
Kanaley JA, Mottram CD, Scanlon PD, Jensen MD . Fatty acid kinetic responses to running above or below lactate threshold. J Appl Physiol 1995; 79: 439–447.
Essen-Gustavsson B, Henriksson J . Enzyme levels in pools of microdissected human muscle fibres of identified type. Adaptive response to exercise. Acta Physiol Scand 1984; 120: 505–515.
Bishop D, Jenkins DG, McEniery M, Carey MF . Relationship between plasma lactate parameters and muscle characteristics in female cyclists. Med Sci Sports Exerc 2000; 32: 1088–1093.
Schantz P, Sjoberg B, Wideck AM, Ekblom B . Skeletal muscle of trained and untrained paraplegics and tetraplegics. Acta Physiol Scand 1997; 161: 31–39.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Knechtle, B., Müller, G., Willmann, F. et al. Fat oxidation at different intensities in wheelchair racing. Spinal Cord 42, 24–28 (2004). https://doi.org/10.1038/sj.sc.3101548
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101548
Keywords
This article is cited by
-
Physiological responses during a 25-km time trial in elite wheelchair racing athletes
Spinal Cord Series and Cases (2018)
-
Effect of pre-exercise carbohydrate ingestion on substrate consumption in persons with spinal cord injury
Spinal Cord (2009)
-
Substrate metabolism during exercise in the spinal cord injured
European Journal of Applied Physiology (2009)
-
Optimal exercise intensities for fat metabolism in handbike cycling and cycling
Spinal Cord (2004)
