
Abstract
The proteasome system is a proteolytic pathway that regulates the expression of genes involved in inflammation. Polymorphisms in the gene encoding subunit α type 6 (PSMA6) – in particular the rs1048990 exon 1–8C/G SNP – have been implicated with susceptibility to myocardial infarction (MI) in a Japanese study. We examined whether several polymorphisms in the PSMA6 gene were related to MI risk in 6946 nonfatal MI cases and 2720 unrelated controls in a UK population. The homozygous GG genotype for rs1048990 was much less frequent in this UK population than in the Japanese population (2.1 vs 8.9%), and was associated with an odds ratio (OR) for MI of 1.09 (95% confidence interval (CI): 0.98–1.21) per G allele in a co-dominant genetic model and 1.32 (95% CI: 0.90–1.93) in a recessive genetic model. Although not statistically significant, these results for this variant are still consistent with the Japanese hypothesis-generating study. Our findings, when taken together with four other studies (including the hypothesis-generating one), yielded a combined OR for MI of 1.15 (95% CI: 1.08–1.21) per G allele in a co-dominant model and 1.38 (95% CI: 1.22–1.57) for the GG genotype in a recessive model. Larger studies involving more than 10 000 disease cases would be required to further elucidate the role of this variant for susceptibility to MI. However, given the rarity of this variant in Caucasians, the attributable risk of rs1048990 for MI is unlikely to be great in western populations.
Similar content being viewed by others

Introduction
The ubiquitin–proteasome pathway plays an important role in the initiation and progression of atherosclerosis by controlling the activation of nuclear factor kappa B (NFκB) proteins, which control expression of genes encoding cytokines involved in inflammation.1, 2 Inflammation has been implicated in the initiation, progression, and complication stages of atherosclerosis. Drugs that inhibit the ubiquitin–proteasome pathway through their effect on NFκB have been shown to reduce the occurrence of stroke and atherosclerosis in animal models.3, 4
Recently, a Japanese case–control study reported that susceptibility to myocardial infarction (MI) was associated with the exon 1–8C/G SNP at rs1048990 in the proteasome subunit α type 6 (PSMA6) gene, which enhances transcription of PSMA6 on chromosome 14q13-q13.2.5 The association of MI with rs1048990, and with a further SNP (intron 1 1233A/T) in near-perfect linkage disequilibrium (LD) with it, was originally found in a sample of 2592 MI cases and 2851 controls, and then replicated in a further 867 MI cases and 1104 controls. The rs1048990 SNP appeared to be functional because of its effects on the NFκB protein concentration in this population.5 If genetic markers associated with the control of pro-inflammatory cytokines are implicated in susceptibility to MI risk, this could provide additional targets for the prevention of atherosclerosis. Consequently, we examined the association of six SNPs in the PSMA6 gene with biochemical markers of inflammation and with risk of MI in the large ISIS case–control study (6946 MI cases and 2720 controls) conducted in a UK population.
Materials and methods
DNA samples
The design of the ISIS case–control study has been described in detail in previous publications.6, 7 DNA was extracted from frozen buffy coat samples using a Taqman and amplifluor technique, as described previously.7, 8 Cases genotyped for this study were men and women aged 30–64 years, with nonfatal MI confirmed by cardiac enzyme or electrocardiographic criteria (or both). Controls genotyped in the present study were spouses of the siblings or children of cases (ie, unrelated to the MI cases except by marriage) aged 30–64 years, and with no history of MI, angina or other definite heart disease. Ethnicity was not recorded, but based on previous studies conducted by our research group in a similar setting, more than 95% would be expected to be Caucasian.9 Participants provided consent to participate in the study, which had research ethics committee approval.
SNP analysis
Six SNPs for PSMA6 were selected for analysis in the ISIS study. The rs1048990 and PSMA6_1233 (intron 1 1233 A/T) SNPs were, respectively, the SNP originally associated with MI and a SNP in perfect LD with it in the Japanese study. The PSMA6_7693 (intron 1 7693 G/A) SNP had been excluded from further analysis in the Japanese study, because it had a minor allele frequency (MAF) <5%, but it is more frequent in European populations (MAF=18%) (http://www.hapmap.org/Data Release #21a). The three other SNPs (rs17458312, rs2277459, and rs2277461) studied had not been included in the Japanese study. Genotyping using mass-spectrometry was carried out at the Centre Nationale de Genotypage in Paris without the knowledge of disease status, with samples from cases and controls distributed within each 384-well genotyping plate. Quality control procedures included assessment of consistency of genotyping between plates through internal controls and replication of measurements in a random sample of 250 controls, to assess the reproducibility of genotyping.
Intermediate phenotypes
Plasma levels of high-sensitivity C-reactive protein (CRP), fibrinogen, albumin, apolipoprotein A1 and apolipoprotein B were measured using standard methods.8 Previous studies had indicated small changes in plasma levels of such analytes due to delay in plasma separation,10 so levels were adjusted for time from collection to separation, as well as for date of assay, to compensate for extrinsic sources of variation.
Statistical analysis
The distributions of genotypes for each SNP were assessed for departure from Hardy–Weinberg equilibrium (HWE) in cases and controls separately, using an exact χ2 goodness of fit test.11 A P-value <0.05 was used to indicate significant departure from HWE. LD between SNPs was assessed using both the standardised disequilibrium (D′)12 and correlation (r2)13 coefficients. A weighted kappa statistic was computed to assess reproducibility of each of the individual SNPs studied. Posterior probabilities of pairs of haplotypes and maximum likelihood estimates of haplotype frequencies were computed for each individual with an expectation-maximisation (E-M) algorithm under the assumption of HWE using the Haplo.stats suite of functions in R.14, 15 The associations of haplotypes that had an estimated frequency >1% with biochemical markers and with MI risk were analysed separately (while the remaining haplotypes with estimated frequencies <1% were ignored).
Standard one-way ANOVA and haplotype-based one-way ANOVA were used to assess the associations of SNPs and haplotypes with plasma levels of biochemical markers in controls. Standard logistic regression adjusted for age and sex, and haplotype-based logistic regression, were used to estimate odds ratios (ORs) for MI for each SNP and haplotype, respectively. Floated absolute risks and confidence intervals (CIs) were used to share the variance of the log ORs appropriately between the different genotypes, which allows a CI to be computed for the reference category and any group to be compared directly with any other.16, 17 Power calculations to detect the association of MI risk with the rs1048990 SNP for the PSMA6 gene in the ISIS case–control study were estimated using standard methods.18, 19 The results of the ISIS study of MI risk were combined with other similar studies using standard meta-analytic methods. We computed the population attributable risk20, 21 to compare the impact of these gene variants in a Western European population with that in a Japanese population using the combined OR from all studies included in the meta-analysis. All analyses were carried out using SAS version 8.222 and R version 2.4.0.23
Results
Data for all six SNPs were available in 6946 cases and 2720 controls who had sufficient DNA for analysis. Table 1 shows the characteristics of these cases and controls. The mean age was 55.1 years in cases and 46.3 years in controls, and a much higher proportion of cases were men. After adjustment for age and sex differences, cases had a higher mean body mass index and higher prevalence of current smokers, hypertension and diabetes mellitus compared with controls.
PSMA6 SNPs and haplotypes
The reproducibility of the genotyping was high, with a weighted kappa score of 0.96–1.00 for each SNP in the PSMA6 gene, except for the rs2277459 SNP which was 0.75 (Supplementary Table A2). The rs2277459 and rs2277461 SNPs were not in HWE amongst controls (Supplementary Table A2), perhaps due to the very low frequencies of their minor alleles in Caucasians (both in ISIS and HapMap; http://www.hapmap.org/Data Release #21a). We investigated a 9-kb region of PSMA6 in our study that was bounded by PSMA6_1233 (intron 1 1233A/T) and rs2277461. Table 2 shows the minor allele frequencies and LD patterns of the six SNPs in the PSMA6 gene examined in the ISIS study. Ozaki et al5 reported near complete LD in terms of r2 between rs1048990 and PSMA6_1233, and the present study demonstrated similar findings for these two SNPs. Indeed, all six SNPs examined in the ISIS study were in high LD with respect to DI (all >0.95), although most were in very low pair-wise LD with respect to r2 values (only the combinations of rs1048990 and PSMA6_1233, rs17458312 and PSMA6_7693, and rs2277459 and rs2277461 had r2 values >0.80). The four SNPs found to be in HWE were incorporated into a haplotype analysis, which yielded three common haplotypes.
Associations with CRP, fibrinogen and albumin
Table 3 shows the mean (SE) values of cardiovascular risk factors for the rs1048990 SNP in the controls. The relatively few individuals with the GG genotype appeared to have higher levels of fibrinogen and CRP, accompanied by lower levels of albumin, compared with those without this genotype. But, these differences were marginally statistically significant (P=0.03) only for fibrinogen and only in a recessive model. None of the other SNPs were associated with significant differences in mean plasma levels of these biochemical markers (Supplementary Table A3). In addition, there were no differences in the proportions of current smokers, or people with hypertension or diabetes mellitus by genotype for any of the SNPs investigated (Supplementary Table A4).
Considering the estimated haplotypes, slightly raised plasma levels of the inflammatory markers CRP and fibrinogen were observed for carriers of the TGGC haplotype, but these differences were not statistically significant (Supplementary Table A5). In addition, no statistically significant differences were observed between the three estimated haplotypes and plasma levels of albumin, apolipoprotein A1 or apolipoprotein B.
Association with MI risk
Table 4 shows the associations of rs1048990 with MI risk after adjustment for age and sex, when analysed using co-dominant and recessive genetic models. In the co-dominant model, rs1048990 was associated with a nonsignificant OR for MI of 1.09 (95% CI: 0.98–1.21) per G allele (P=0.11). For a recessive model, the OR for MI was 1.32 (95% CI: 0.90–1.93) for the GG genotype, but again this association was not statistically significant (P=0.16). The other SNPs were less strongly associated with MI risk, with the exception of the rs2277459 SNP. However, the rs2277459 SNP had a poor kappa score, evidence of departure from HWE, and an MAF of <5%, so this marginally significant (P=0.01) result should be interpreted with caution (Supplementary Table A6). None of the three estimated individual haplotypes for the PSMA6 gene were significantly associated with MI risk (Global score-statistic χ23=5.65, P=0.13) (Supplementary Table A7).
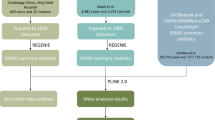
Figure 1 shows the results of a meta-analysis of the ISIS study and four other studies (three Japanese and one European). The overall pooled ORs for MI were 1.15 (95% CI: 1.08–1.21) when estimated using a co-dominant model and 1.38 (95% CI: 1.22–1.57) with a recessive model. There was no evidence of statistical heterogeneity between the results in the different studies for either genetic model (both P>0.10).

Odds ratio (& 95% CI) for MI associated with the rs1048990 polymorphism. The size of the squares are proportional to the variance of the log OR and horizontal lines represent the 95% CI. The diamond represents the pooled estimate with the width being the 95% CI. Panel (a) shows individual study estimates and the overall pooled odds ratios for myocardial infarction (MI) when estimated using a co-dominant genetic model. Panel (b) shows individual study estimates and the overall pooled odds ratios for MI when estimated using a recessive genetic model.
Using the combined OR of 1.38 for a recessive model, we estimated the population attributable risk to be 0.6% in a Western European population (as included in the ISIS study) as compared to 3.5% in the Japanese population. For the co-dominant model, using the combined OR of 1.15, the estimated population attributable risk would be 2.4% in a western population compared to 8.1% in the Japanese population.
Discussion
The ISIS study involving 6946 MI cases and 2720 unrelated controls is the largest genetic association study to date of MI risk in relation to polymorphisms of the PSMA6 gene, and one of the first studies to investigate the associations in a Caucasian population. In the ISIS study, the rs1048990 SNP was associated with an OR for MI of 1.09 (95% CI: 0.98–1.21) per G allele in a co-dominant model. This result is less extreme than the hypothesis-generating study by Ozaki et al,5 which reported an OR for MI of 1.21 (95% CI: 1.11–1.31) per G allele in the Japanese population, but similar to the ORs for MI of 1.06 (95% CI: 0.91–1.24) and 1.06 (95% CI: 0.78–1.44) per G allele reported by Takashima et al24 and Sjakste et al25 in a Japanese and a Caucasian population, respectively (see Figure 1a). A meta-analysis of the results for the rs1048990 SNP in the ISIS study and the four other studies, involving a total of 11 127 cases and 9109 controls, yielded combined ORs of 1.15 (95% CI: 1.08–1.22) per G allele in a co-dominant model and 1.38 (95% CI: 1.22–1.57) in a recessive model, with no evidence of statistical heterogeneity between the results of these studies. The ISIS study had 98% power to detect a 39% increase in risk of MI associated with the rs1048990 SNP in a recessive genetic model, but only 78% power to detect a 15% increase in risk using a co-dominant model.18 These associations are relatively modest, but similar in magnitude to those reported in previous studies involving other inflammatory-related genes.26
There was a substantial difference in the frequency of the homozygous GG genotype for rs1048990 in the two European and the three Japanese studies (2.1 and 3.0% vs 8.9, 10.7, and 9.8% respectively). The observed genotype frequencies of rs1048990 in these two populations are consistent with those reported by HapMap (http://www.hapmap.org/Data Release #21a). Despite the large number of cases in the ISIS study, the lower allele frequency results in a greater variability in the effect size and, hence, a proportionately smaller contribution to the meta-analysis (as depicted by a smaller square and wider CI in Figure 1). Moreover, the low frequency of the GG genotype means that the estimated population attributable risk is only about 1–2% in this Western European population compared with 3–8% in the Japanese population (depending on whether a recessive or codominant genetic model is used).
The four other studies appear to be well conducted; controls were recruited from the same population as the cases, and the control genotype frequencies were in HWE. Even though selection of cases and controls of the same nationality and ethnicity does not rule out a false positive result due to population stratification,27 the researchers in the Ozaki study also used genomic control methods28 to account for this. The procedures used for recruitment of controls in the ISIS case–control study (involving spouses of siblings and their children) should also have minimised the impact of population admixture between controls and cases. There were departures from HWE for two rare SNPs in the ISIS study, but this was not the case for rs1048990, which was the main SNP of interest.
In the Ozaki study, the authors reported that the G allele was associated with 1.7–1.8 higher expression of PSMA6, which they suggested could have an effect on genes in the NFκB pathway. The Suita study conducted by Takashima et al24 found the rs1048990 SNP to be significantly associated with intima-media thickness of the carotid artery and suggested that it may play a role in the pathogenesis of atherosclerosis. PSMA6 concentrations have not been measured in the ISIS study, but measurements were made of plasma concentrations of CRP and fibrinogen (which are established markers of inflammation). Both the p50 and p60 subunits of NFκB play a role in the transcription of CRP,29 which appeared to have proatherogenic properties through upregulation of expression of AT1 receptor30 and activation of vascular smooth muscle cells in some studies.31, 32 Over 30 studies have reported that higher plasma levels of CRP are associated with higher risks of CHD,33 but other studies have not been to able to confirm these associations,34, 35 and there is uncertainty as to whether these associations are causal. Fibrinogen has been observed to regulate to NFκB activation and the expression of chemokines in vascular endothelial cells,36 but for it too there is uncertainty about the nature of the relationship with vascular disease.37, 38 In the ISIS study, CRP and fibrinogen levels were not significantly associated with the number of copies of the G allele for the rs1048990 SNP. In a recessive genetic model, carriers of the GG genotype appeared to have slightly higher levels of fibrinogen and CRP, but the low frequency of this genotype made these differences inconclusive.
Ozaki et al39 investigated the PSMA6 gene, because they had previously observed that SNPs encoding lymphotoxin α (LTA), a cytokine produced in the early stages of inflammation, was associated with an increased susceptibility to MI in a Japanese population. Binding of LTA to its receptor is known to activate NFκB, which has an effect on the ubiquitin–proteasome system. We have previously reported no significant association of the rs1041981 SNP in LTA gene with MI risk in the ISIS study.8 The frequency of the minor A allele for rs1041981 is similar for European and Japanese populations from HapMap (0.36 and 0.43, respectively) (http://www.hapmap.org/Data Release #21a). Thus, the lack of association of LTA with MI risk in the ISIS study was unlikely to be due to differences in the frequency of this allele, although it could be that this particular pathway is less important in Caucasians than in Japanese populations.
In conclusion, although the ISIS case–control study failed to identify statistically significant associations with MI for rs1048990 in the PSMA6 gene, the results remain entirely consistent with the findings of the previous studies. The results of a meta-analysis of these studies were homogenous, but further population-based studies (or meta-analyses of such studies) involving very large sample sizes (in excess of 10 000 cases and 10 000 controls) would help to confirm the relevance of this gene for MI risk. Even if this variant is found to be causal, however, the low prevalence of the GG genotype means that the impact on overall MI risk is likely to be small, especially in western populations.
References
Herrmann J, Ciechanover A, Lerman LO, Lerman A : The ubiquitin–proteasome system in cardiovascular diseases-a hypothesis extended. Cardiovasc Res 2004; 61: 11–21.
Palombella VJ, Rando OJ, Goldberg A, Maniatis T : The ubiquitin-proteasome pathway is required for processing the NF-[kappa]B1 precursor protein and the activation of NF-[kappa]B. Cell 1994; 78: 773–785.
Meiners S, Laule M, Rother W et al: Ubiquitin–proteasome pathway as a new target for the prevention of restenosis. Circulation 2002; 105: 483–489.
Elliott PJ, Zollner TM, Boehncke WH : Proteasome inhibition: a new anti-inflammatory strategy. J Mol Med 2003; 81: 235–245.
Ozaki K, Sato H, Iida A et al: A functional SNP in PSMA6 confers risk of myocardial infarction in the Japanese population. Nat Genet 2006; 38: 921–925.
Keavney B, McKenzie C, Parish S et al: Large-scale test of hypothesised associations between the angiotensin-converting-enzyme insertion/deletion polymorphism and myocardial infarction in about 5000 cases and 6000 controls. International Studies of Infarct Survival (ISIS) Collaborators. Lancet 2000; 355: 434–442.
Keavney B, Palmer A, Parish S et al: Lipid-related genes and myocardial infarction in 4685 cases and 3460 controls: discrepancies between genotype, blood lipid concentrations, and coronary disease risk. Int J Epidemiol 2004; 33: 1002–1013.
Clarke R, Xu P, Bennett D et al: Lymphotoxin-alpha gene and risk of myocardial infarction in 6928 cases and 2712 controls in the ISIS case–control study. PLoS Genet 2006; 2: e107.
MRC/BHF Heart Protection Study Collaborative Group: MRC/BHF Heart Protection Study of cholesterol-lowering therapy and of antioxidant vitamin supplementation in a wide range of patients at increased risk of coronary heart disease death: early safety and efficacy experience. Eur Heart J 1999; 20: 725–741.
Clark S, Youngman LD, Palmer A, Parish S, Peto R, Collins R : Stability of plasma analytes after delayed separation of whole blood: implications for epidemiological studies. Int J Epidemiol 2003; 32: 125–130.
Guo SW, Thompson EA : Performing the exact test of Hardy–Weinberg proportion for multiple alleles. Biometrics 1992; 48: 361–372.
Lewontin RC : On measures of gametic disequilibrium. Genetics 1988; 120: 849–852.
Hill W, Robertson A : Linkage disequilibrium in finite populations. Theor Appl Genet 1968; 38: 226–231.
Schaid DJ, Rowland CM, Tines DE, Jacobson RM, Poland GA : Score tests for association between traits and haplotypes when linkage phase is ambiguous. Am J Hum Genet 2002; 70: 425–434.
Schaid DJ : Evaluating associations of haplotypes with traits. Genet Epidemiol 2004; 27: 348–364.
Easton DF, Peto J, Babiker AG : Floating absolute risk: an alternative to relative risk in survival and case-control analysis avioding an arbritrary reference group. Stat Med 1991; 10: 1025–1035.
Plummer M : Improved estimates of floating absolute risk. Stat Med 2004; 23: 93–104.
Slager SL, Schaid DJ : Case–control studies of genetic markers: power and sample size approximations for Armitage's test for trend. Hum Hered 2001; 52: 149–153.
Freidlin B, Zheng G, Li Z, Gastwirth JL : Trend tests for case–control studies of genetic markers: power, sample size and robustness. Hum Hered 2002; 53: 146–152.
Schlesselman JJ : Case-Control Studies: Design, Conduct, Analysis. London: Oxford University Press, 1982.
Rockhill B, Newman B, Weinberg C : Use and misuse of population attributable fractions. Am J Public Health 1998; 88: 15–19.
SAS Institute: SAS Version 8. Cary, North Carolina: SAS Institute, 1999.
Ihaka R, Gentleman R : R: a language for data analysis and graphics. J Comput Graph Stat 1996; 5: 299–314.
Takashima N, Shioji K, Kokubo Y et al: Validation of the association between the gene encoding proteasome subunit alpha type 6 and myocardial infarction in a Japanese population. Circ J 2007; 71: 495–498.
Sjakste T, Poudziunas I, Ninio E et al: SNPs of PSMA6 gene – investigation of possible association with myocardial infarction and type 2 diabetes mellitus. Genetika 2007; 43: 553–559.
Morgan TM, Krumholz HM, Lifton RP, Spertus JA : Nonvalidation of reported genetic risk factors for acute coronary syndrome in a large-scale replication study. JAMA 2007; 297: 1551–1561.
Helgason A, Yngvadottir B, Hrafnkelsson B, Gulcher J, Stefansson K : An Icelandic example of the impact of population structure on association studies. Nat Genet 2005; 37: 90–95.
Pritchard JK, Stephens M, Rosenberg NA, Donnelly P : Association mapping in structured populations. Am J Hum Genet 2000; 67: 170–181.
Agrawal A, Cha-Molstad H, Samols D, Kushner I : Overexpressed nuclear factor-kappaB can participate in endogenous C-reactive protein induction, and enhances the effects of C/EBPbeta and signal transducer and activator of transcription-3. Immunology 2003; 108: 539–547.
Wang CH, Li SH, Weisel RD et al: C-reactive protein upregulates angiotensin type 1 receptors in vascular smooth muscle. Circulation 2003; 107: 1783–1790.
Hattori Y, Matsumura M, Kasai K : Vascular smooth muscle cell activation by C-reactive protein. Cardiovasc Res 2003; 58: 186–195.
Cirillo P, Golino P, Calabro P et al: C-reactive protein induces tissue factor expression and promotes smooth muscle and endothelial cell proliferation. Cardiovasc Res 2005; 68: 47–55.
Danesh J, Wheeler JG, Hirschfield GM et al: C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004; 350: 1387–1397.
Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P : N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as predictors of mortality and cardiovascular events in older adults. JAMA 2005; 293: 1609–1616.
van der Meer IM, de Maat MP, Kiliaan AJ, van der Kuip DA, Hofman A, Witteman JC : The value of C-reactive protein in cardiovascular risk prediction: the Rotterdam Study. Arch Intern Med 2003; 163: 1323–1328.
Guo M, Sahni SK, Sahni A, Francis CW : Fibrinogen regulates the expression of inflammatory chemokines through NF-kappaB activation of endothelial cells. Thromb Haemost 2004; 92: 858–866.
Danesh J, Lewington S, Thompson SG et al: Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. JAMA 2005; 294: 1799–1809.
Keavney B, Danesh J, Parish S et al: Fibrinogen and coronary heart disease: test of causality by ‘Mendelian randomization’. Int J Epidemiol 2006; 35: 935–943.
Ozaki K, Ohnishi Y, Iida A et al: Functional SNPs in the lymphotoxin-alpha gene that are associated with susceptibility to myocardial infarction. Nat Genet 2002; 32: 650–654.
ISIS-3 (Third International Study of Infarct Survival) Collaborative Group: ISIS-3: a randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41 299 cases of suspected acute myocardial infarction. Lancet 1992; 339: 753–770.
Acknowledgements
The chief acknowledgement for the ISIS study is to the patients and their relatives who collaborated, to their general practitioners, and to the medical and nursing staff from more than 100 hospitals in the UK. A full list of the participating centres and collaborators is given in the ISIS-3 report.40 We also thank Peter Sleight, the Chairman of the ISIS Steering Committee. The ISIS trials and epidemiological studies were supported by the manufacturers of the study drugs, and by the British Heart Foundation, Medical Research Council, Cancer Research UK, Tobacco Products Research Trust of the UK Department of Health Independent Scientific Committee on Smoking and Health, and Oxford NHS Genetic Knowledge Park.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Supplementary information accompanies the paper on European Journal of Human Genetics website (http://www.nature.com/ejhg)
Supplementary information
Rights and permissions
About this article
Cite this article
Bennett, D., Xu, P., Clarke, R. et al. The exon 1–8C/G SNP in the PSMA6 gene contributes only a small amount to the burden of myocardial infarction in 6946 cases and 2720 controls from a United Kingdom population. Eur J Hum Genet 16, 480–486 (2008). https://doi.org/10.1038/sj.ejhg.5201948
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5201948
Keywords
This article is cited by
-
Association of intronic polymorphisms (rs1549339, rs13402242) and mRNA expression variations in PSMD1 gene in arsenic-exposed workers
Environmental Science and Pollution Research (2020)
-
Quantitative assessment of the influence of PSMA6 variant (rs1048990) on coronary artery disease risk
Molecular Biology Reports (2013)
-
Replication studies for the association of PSMA6 polymorphism with coronary artery disease in East Asian populations
Journal of Human Genetics (2009)
