
Abstract
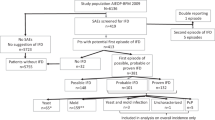
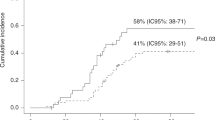
Transplanted patients with a history of invasive fungal infection (IFI) are at high risk of developing relapse and fatal complications. Eighteen patients affected by hematological malignancies and a previous IFI were submitted to allogeneic stem cell transplantation, using Caspofungin as a secondary prophylaxis. Patients had a probable or proven fungal infection and 16 had a pulmonary localization. No side effects were recorded during treatment with Caspofungin. Compared to pre-transplant evaluation, stability or improvement of the previous IFI was observed in 16 of the 18 patients at day 30, in 13 of the 15 evaluable patients at day 180 and in 11 of the 11 evaluable patients at day 360 post transplant. In particular, all the six patients with a proven fungal infection were alive, with a stable or improved IFI after 1 year from transplant. At a maximum follow-up of 31 months, eight patients died for disease progression or transplant-related complications, but only two had evidence of fungal progression. Secondary prophylaxis with Caspofungin may represent a suitable approach to limit IFI relapse or progression, allowing patients with hematological malignancies to adhere to the planned therapeutic program.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others
References
Lin SJ, Schranz J, Teutsch SM . Aspergillosis case-fatality rate: systematic review of the literature. Clin Infect Dis 2001; 32: 358–364.
Marr K, Carter R, Crippa F, Wald A, Corey L . Epidemiology and outcome of mould infections in hematopoietic stem cell transplant recipients. Clin Infect Dis 2002; 34: 909–917.
Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002; 347: 408–415.
Sipsas NV, Kontoyiannis DP . Clinical issues regarding relapsing aspergillosis and the efficacy of secondary antifungal prophylaxis in patients with haematological malignancies. Clin Infect Dis 2006; 42: 1584–1591.
Offner F, Cordonnier C, Ljungman P, Prentice HG, Engelhard D, De Bacquer D et al. Impact of previous aspergillosis on the outcome of bone marrow transplantation. Clin Infect Dis 1998; 26: 1098–1103.
Cordonnier C, Beaune J, Offner F, Marinus A, Ljungman P, Meunier F . Aspergillosis prior to bone marrow transplantation. Infectious disease working party of the EBMT and the EORTC Invasive Fungal Infections Cooperative Group. Bone Marrow Transplant 1995; 16: 323–324.
Bjerke JW, Meyers JD, Bowden RA . Hepatosplenic candidiasis: a contraindications to marrow transplantation? Blood 1994; 15: 2811–2814.
Cordonnier C, Maury S, Pautas C, Bastiè JN, Chehata S, Castaigne S et al. Secondary antifungal prophylaxis with voriconazole to adhere to scheduled treatment in leukemic patients and stem cell transplant recipients. Bone Marrow Transplant 2004; 33: 943–948.
Stute N, Kratochwille A, Zabelina T, Fehse N, Hassenpflug W, Panse J et al. Caspofungin is highly effective as secondary prophylaxis in allogeneic stem cell transplantation in patients with prior systemic or invasive fungal infections. Blood 2003; 102 (abstract 3636).
Onishi J, Meinz M, Thompson J, Curotto J, Dreikorn S, Rosenbach M et al. Discovery of novel antifungal (1,3)-beta-d-glucan synthase inhibitors. Antimicrob Chemother 1999; 44: 368–377.
Sanz-Rodriguez C, Lopez-Duarte M, Jurado M, Lopez J, Arranz R, Cisneros JM et al. Safety of the concomitant use of Caspofungin and cyclosporin-A in patients with invasive fungal infections. Bone Marrow Transplant 2004; 34: 13–20.
Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J, Crokaert F et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplant: an international consensus. Clin Infect Dis 2002; 34: 7–14.
Gooley TA, Leisenring W, Crowley J, Storer BE . Estimation of failure probabilities in the presence of competing risks: new representation of old estimators. Stat Med 1999; 18: 695–706.
Sable CA, Nguyen B-YT, Chodakewitz JA, DiNubile MJ . Safety and tolerability of Caspofungin in the treatment of fungal infections. Transplant Infect Dis 2002; 4: 25–30.
Walsh TJ, Teppler H, Donowitz GR, Maertens JA, Baden LR, Dmoszynska A et al. Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia. N Engl J Med 2004; 351: 1391–1402.
Dominietto A, Lamparelli T, Raiola AM, Van Lint MT, Gualandi F, Berisso G et al. Transplant-related mortality and long-term graft function are significantly influenced by cell dose in patients undergoing allogeneic marrow transplantation. Blood 2002; 100: 3930–3934.
Girgis M, Hallemeier C, Blum W, Brown R, Lin HS, Khoury H et al. Chimerism and clinical outcome of 110 recipients of unrelated donor bone marrow transplant who underwent conditioning with low-dose, single exposure total body irradiation and cyclophosphamide. Blood 2005; 105: 3035–3041.
Yeghen T, Kibbler CC, Prentice HG, Berger LA, Wallesby RK, McWhinney PH et al. Management of invasive pulmonary aspergillosis in hematology patients: a review of 87 consecutive cases at a single institution. Clin Infect Dis 2000; 31: 859–868.
Massard G . Role of surgery in the treatment of pulmonary aspergillosis. Rev Mal Respir 2005; 22: 466–472.
Martino R, Parody R, Fukuda T, Maertens J, Theunissen K, Ho A et al. Impact of the intensity of the pretransplantation conditioning regimen in patients with prior invasive aspergillosis undergoing allogeneic hematopoietic stem cell transplantation: a retrospective survey of the Infectious Disease Working Party of the European Group for Blood and Marrow Transplantation. Blood 2006; 108: 2928–2936.
Junghanss C, Marr KA, Carter RA, Sandmaier BM, Maris MB, Maloney DG et al. Incidence and outcome of bacterial and fungal infections following non-myeloablative compared to myeloablative allogeneic hematolopietic stem cell transplantation: a matched control study. Biol Blood Marrow Transplant 2002; 8: 512–520.
Fukuda T, Boeckh M, Carter RA, Sandmaier BM, Maris MB, Maloney DG et al. Risks and outcomes of invasive fungal infections in recipients of allogeneic hematoloietic stem cell transplants after non-myeloablative conditioning. Blood 2003; 102: 827–833.
Safdar A . Strategies to enhance immune function in hematopoietic transplantation recipients who have fungal infections. Bone Marrow Transplant 2006; 38: 327–337.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
de Fabritiis, P., Spagnoli, A., Di Bartolomeo, P. et al. Efficacy of caspofungin as secondary prophylaxis in patients undergoing allogeneic stem cell transplantation with prior pulmonary and/or systemic fungal infection. Bone Marrow Transplant 40, 245–249 (2007). https://doi.org/10.1038/sj.bmt.1705720
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705720
Keywords
This article is cited by
-
Analysis of the efficiency and costs of antifungal prophylaxis and mycological diagnostics in patients undergoing allogeneic haematopoietic cell transplantation: “real life” evaluation
Annals of Hematology (2016)
-
Infectious diseases in allogeneic haematopoietic stem cell transplantation: prevention and prophylaxis strategy guidelines 2016
Annals of Hematology (2016)
-
The impact of prior invasive mold infections in leukemia patients who undergo allo-SCT in the era of triazole-based secondary prophylaxis
Bone Marrow Transplantation (2013)
-
Current Role of Echinocandins in the Management of Invasive Aspergillosis
Current Infectious Disease Reports (2011)
-
Secondary Antifungal Prophylaxis in Hematopoietic Stem Cell Transplantation (HSCT)/Acute Leukemia Patients
Current Infectious Disease Reports (2011)
