
Abstract
This study compared the effects on weight as well as on metabolic parameters and liver size of a very low-calorie ketogenic diet versus a Mediterranean diet in patients with morbid obesity preparing to undergo bariatric surgery. This prospective comparison study evaluated patients 18–65 years of age who enrolled for bariatric surgery. Study duration was limited to an immediate preoperative period of 15 days. The very low-calorie ketogenic diet incorporated 10–12 kcal/kg/day of energy and 1–1.2 g/kg of protein using Kalibra (Societa Dietetica Medica) (VLCKD-SDM). The Mediterranean diet (MD) included 15–20% protein, 45–50% carbohydrate, and 25–35% fat. Changes in body mass index (BMI), liver size, and anthropometric and metabolic measurements were assessed. Between January 2016 and March 2017, of 45 patients enrolled, 30 completed the study (VLCKD-SDM, n = 15; MD, n = 15). Respective median BMI loss after VLCKD-SDM was 2.7 kg/m2 versus MD 1.4 kg/m2 (p < 0.05); median fat percentage reduction was 3.2 units versus 1.7 units (p < 0.05). Median liver size decreased 5.5% in the VLCKD-SDM group versus 1.7% in the MD group (p < 0.05). Median total cholesterol, and LDL levels decreased in both groups (p < 0.05), with greater relative decreases in the VLCKD-SDM group. Short-term preoperative diet-based weight loss in patients with morbid obesity preparing for bariatric surgery was significantly greater following a very low-calorie ketogenic diet versus a Mediterranean diet. The very low-calorie diet also significantly improved anthropometric and metabolic parameters and reduced preoperative liver size above that of the MD.
Similar content being viewed by others

Introduction
Obesity is a disease that affects approximately 641 million adults worldwide. Of these, 58 million men and 126 million women suffer from morbid obesity, which is typically associated with diseases such as non-alcoholic fatty liver disease (NAFLD), sleep apnea syndrome, hypertension, type 2 diabetes mellitus, and dyslipidemias1. Liver damage increases with increasing body mass index (BMI), and a large liver size is significantly related to increased surgical morbidity and mortality2. Prior to metabolic/bariatric surgery, intentional weight loss can successfully reduce liver size and improve intraoperative management of the anatomy. Short-term, low-energy, low-carbohydrate diets have been shown to be particularly effective in reducing BMI and liver size and in helping patients to anticipate postoperative weight loss3,4,5,6,7,8,9,10.
The efficacy of the Mediterranean diet (MD) in achieving weight loss in patients who are overweight or who suffer from obesity has been much publicized9. A variety of diets have been tested and compared with the MD, both longitudinally following bariatric surgery, and prior to surgery over a brief time period to induce rapid weight loss. Observational studies randomized controlled trials, and systematic reviews have cited the low-calorie ketogenic diet (VLCKD) as the most successful in achieving weight loss2. Ketogenic-based diets may induce greater weight loss by the expenditure of energy in gluconeogenesis due to the low glucose intake, decreased appetite, and increased energy expenditure resulting from ketosis2,3. In the current study, we assessed the effects of the MD versus a VLCKD undertaken by patients with morbid obesity over a 2-week pre-bariatric surgery time course. Weight loss is aimed to be the initial outcome of this study. It is intended to reduce the liver size by losing weight. An overall weight loss goal of 5–10% was thought to be safe and feasible, and has been associated with a reduction in visceral fat and liver size within a few weeks5,11. Preoperative changes in weight, liver size, anthropometric parameters, and metabolic outcomes for patients on each diet were compared.
Methods
Study design and approval
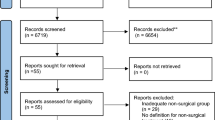
This prospective comparison study was undertaken to assess changes in morbidly obese patients in two groups, each undertaking a 2-week trial of a different diet before undergoing bariatric surgery. These diets are not routinely practiced in the clinic. This is not an interventional study. Patients were randomly assigned to diet types. The standard effect size was determined as 1.05 with 5% margin of error and 80% power for the sample size. It was found sufficient to include n = 14 cases in each group. According to this minimum number, 15 people were included in each group. The primary outcome used to base statistical power was body mass index. Forty-five morbidly obese patients were included in the study. At the beginning of the study before exclusion, 25 of these 45 patients were in the VLCKD-SDM group and 20 were in the MD group. After the excluded patients, the number of patients in each diet group fulfilled the numbers required for the sample size. Nine patients failed to adhere to the diet and were therefore excluded from the study. Of these patients, 7 were in the VLCKD-SDM and 2 were in the MD group. Additionally, 6 patients had early surgery. Three of these belonged to the VLCKD-SDM group, and three to the MD group. Patients who failed to follow the diet and underwent surgery too soon were unable to finish the 14-day diet phase. They were left out of the study to avoid having a negative impact on the findings. The study was conducted with pre-approval of the hospital’s Non-invasive Clinical Research Ethics Committee (Decision No. 161, Approval #10840098-604.01.01-E.12049 and E-10840098-772.02-2490; dated 09.03.2016, 29.07.2016, 01.06.2021) and was performed in accord with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Inclusion and exclusion
Patients seeking bariatric surgery who were 18–65 years of age with a BMI of ≥ 35.0 kg/m2 with up to two comorbidities were included in the study. Patients were excluded if they were females who were pregnant or lactating, or men and women with acute or chronic kidney failure (creatinine, women ≥ 1.2 mg/dL, men ≥ 1.3 mg/dL or glomerular filtration rate < 60–65 mL/min), chronic alcoholism, cancer, liver failure, acid–base balance disorder, severe psychiatric disorders, or active peptic ulcer disease.
Diets
VLCKD-SDM
The very-low calorie ketogenic diet (VLCKD) group’s 2-week course consisted of meal replacements using Societa Dietetica Medica (SDM, Kalibra [VLCKD-SDM]) products. Patients were provided with 1–1.2 g/kg/day of protein based on each patient’s calculated ideal weight, 10–12 kcal/kg/day of energy (containing 30–40% fat) based on ideal weight. One portion of each product contained 16–18 g of protein (31 g, pasta, 20 g, focaccia), 60–224 kcal of energy, 0.1–12 g of fiber, and 0.9–9.6 g of fat. The respective protein content of the above products is composed of whey, egg, wheat, and pea protein. Products also contained important amino acids (i.e., leucine, lysine, isoleucine, valine, methionine, phenylalanine, threonine, and tryptophan) and sucralose approved by the U.S. Food and Drug Administration (FDA) as a sweetener.
In addition, patients were instructed to drink 2–3 L of water a day. Individualized nutritional supplements were given under the supervision of the doctor12,13. These included: 1 tablet Supradyn All Day (Bayer Turkish Chemical Industry Trade Ltd., Turkey); 1 effervescent tablet of Kalinor (Farma-Tek Pharmaceutical Industry, and Trade Co. Ltd., Germany); 2 tablets of calcium, Osteocare (Vitabiotics Ltd., UK); 1 capsule of n-3 polyunsaturated fatty acid (PUFA), Marincap (Kocak Farma Pharmaceutical, and Chemical Industry Trade Co. Ltd., Turkey); and 1 packet/day NBL Probiotic Gold (Cell Biotech Co. Ltd., South Korea).
Mediterranean diet
Based on an updated systematic review of the core compositional elements of a Mediterranean diet14, the study required patients in the MD group to consume 15–20% protein (low-fat dairy, poultry, fish, legumes, nuts, red meat) in their daily food intake, 45–50% carbohydrates (vegetables, fruits, whole grains), and 25–35% fat (especially from olive oil). In this MD, the daily minimum requirements of vitamins and minerals were expected to be included with the food and beverage selections; therefore, supplements were not added.
Diet follow-up
Demographic information, anthropometric and biochemical measurements, liver size, and gastrointestinal issues were assessed carefully before and after the diet. An interview was conducted at the hospital outpatient clinic to evaluate the nutritional status of the patients in detail on the 7th and the 15th days after the start of the study. Dietary compliance, ketones in urine, and any complications were assessed.
Determining food consumption status
The patients' required intake of energy and macronutrients for both diet groups was determined using a formula. Our ketogenic diet group was fed commercial products, therefore daily macronutrients were determined based on the information on the labels of the goods they consumed over the course of 14 days. A 24-h diary was kept by members of our Mediterranean diet group. Patients were instructed to record on a chart the foods and meals they consumed over the course of three days, one of which being a weekend. The amounts of all foods consumed were calculated using the units of g and kg. The portions of the stated contents were chosen based on standardised recipes15. Consumed foods and portion amounts of meals were one by one entered into the Nutrition Information System (BeBiS) database software programme. This software was used to compute the daily intake of energy, carbohydrate, fat, and micronutrients16.
Evaluation of nutritional status
Anthropometric measurements
BMI was calculated using ideal BMI (IBMI) and ideal body weight (IBW) formulas17,18. Weight loss (WL%)19 and basal metabolic rate (BMR) were calculated with the Schofield Equation20. Body fat percentage and lean body mass (LBM) were calculated using standard formulas21. Waist, hip, and middle-upper arm circumference (MUAC) measurements were taken. Waist Circumference was assessed at the midpoint between the 12th rib and the iliac crest, while hip circumference was measured at the level of the greater trochanter. Waist/hip ratio was calculated as WC/HC18,22. Malnutrition status was determined by the nutritional risk index (NRI)23. Nutritional Risk Index (NRI) values were calculated by using plasma albumin levels and body weight alterations and compared with reference data NRI was calculated upon the following formula:
NRI values were considered according to the data given below:
NRI > 100 normal,
NRI > 97.5 borderline malnutrition,
NRI = 83.5–97.5 moderate malnutrition,
NRI = 83.5 severe malnutrition.
Biochemical measurements
Biochemical measurements were performed after an overnight fast. These measurements were repeated two times in each group. Adherence to the protein-rich diet was detected by the presence of ketones in the urine.
Liver size
The liver size of patients was measured by the same radiologist in both study groups by abdominal sonography just before starting the pre-operative diet and 2 weeks after when the diet period ended just before the surgery. Both measurement values were assessed by the surgical team. No liver measurements were made in the postoperative period. The measurement was accomplished according to the method described by Börner et al., by taking the mid-clavicular line in maximum inspiration and supine positions as reference by using a 2–5-MHz convex abdominal sonography probe. Reference value, mean male ≤ 150 ± 15 mm and female ≤ 149 ± 16 mm values were considered normal24.
Statistical evaluation
Analyses were performed using the SPSS statistical package (version 22, IBM, Chicago, IL, USA). Descriptive statistics were calculated for all variables assessed. Quantitative variables were reported as means, standard deviations (SDs), medians, minimums, and maximums. Qualitative variables were reported as frequencies and percentages. Interquartile ranges were used. Data normality was evaluated by visual inspection of histograms/Q–Q plots and cross-validated by the Kolmogorov Smirnov test. As appropriate, independent samples t-tests or Mann–Whitney U-tests were used to assess between-group differences with respect to quantitative baseline and outcome variables; chi-square tests (or Fisher's exact tests) were applied to qualitative data. Paired-samples t-tests or Wilcoxon signed-rank tests (as appropriate) were used to analyze within-group change from baseline along quantitative variables; McNemar’s test was used for qualitative data. Correlations of the independent variables were performed by Spearman's correlation tests. All statistical tests were two-tailed and statistical significance was set at p < 0.05.
Ethical approval
Ethics Committee approval (# 10840098-604.01.01-E.12049, dated 09.03.2016 and 29.07.2016, Decision #161) was obtained to conduct the study from the Istanbul Medipol University Noninvasive Clinical Research Ethics Committee.
Informed consent
Informed consent was obtained from all study participants.
Human and animal rights
The study was performed in accord with the ethical standards of the 1964 Declaration of Helsinki and its subsequent amendments.
Results
Between January 2016 and March 2017, 45 patients (25 in VLCKD-SDM, 20 in MD group) with morbid obesity between the ages of 18 and 65 years were enrolled in the General Surgery Department to undergo bariatric surgery. Nine patients (7 in VLCKD-SDM, 2 in MD group) could not adhere to the diet and 6 patients (3 in VLCKD-SDM, 3 in MD group) were operated on earlier than originally planned, excluding 15 patients from the study. Thus, the total study sample was 30 patients, 15 in the VLCKD-SDM group and 15 in the MD group. Each group consisted of 4 (26.7%) men and 11 (73.3%) women. The respective mean age of VLCKD-SDM versus MD patients was 42.9 ± 12.6 (median 46) years versus 41.3 ± 14.6 (median 47) years (p > 0.05); height, 160.3 ± 10.0 (median 158) cm versus 163.9 ± 8.2 (median 161) cm (p > 0.05); and absolute weight, 125.3 kg versus 135.0 kg.
The daily energy and macronutrients in each diet group are shown in Table 1.
In conjunction with diet-induced weight loss, significant decreases in anthropometric measurements from baseline (p = 0.001) were observed in both groups (Table 2).
Metabolic parameters in each diet group are shown in Table 3. The greater weight loss and changes in anthropometric measurements in the VLCKD-SDM group generally translated into statistically greater improvements in metabolic parameters (Table 3). Both diet groups experienced significant change from baseline in total cholesterol, low-density lipoprotein (LDL), and triglyceride (TG) levels (all p < 0.05); however, the reductions in the VLCKD-SDM group were significantly greater relative to the MD group with respect to total cholesterol, HDL, and LDL (all p < 0.05).
Liver and blood biochemical parameters are shown in Table 4.
Finally, urinalysis revealed ketone presence in all VLCKD-SDM patients; however, this was not the case for all patients in the MD group. The McNemar test was used to statistically evaluate the ketone measurement in the urine.
Correlations between total energy, weight loss%, fat%, and LBM and metabolic parameters from Total Group (VLCKD-SDM + MD), VLCKD-SDM and MD are shown in Addendum Tables 1, X2, C3.
Minor complications of the two diets included nausea, constipation, and diarrhea in the VLCKD-SDM group, and only constipation in the MD group.
Discussion
The protective effects on the cardiovascular system of implementing a long-term Mediterranean diet have been well demonstrated. In the 1960s, Ancel Keys formally elaborated the characteristics of the MD25 as inclusive of monosaturated fats (especially from olive oil), vegetables and fruits, whole grains, and low-fat dairy consumed daily; poultry, fish, legumes and nuts consumer weekly; and modest consumption of red meat 2–3 times monthly. Epidemiological studies and clinical trials have reported the anti-metabolic syndrome effects and anti-inflammatory and antioxidant properties of implementing a MD26,27,28. More recently, VLCKDs, MDs, and other programs comprised of appropriate protein and energy levels have demonstrated statistically significant preoperative weight loss and improvement of anatomical access after short-term pre-bariatric surgery diets.
The literature reports an array of preoperative dietary program durations, ranging from 10 days through 20 weeks, and a variety of claims regarding the reduction of intraoperative risks, postoperative complications, operating room time, hospital stay, and improvement of comorbidities through preoperative dieting7,29. Our discussion herein focuses solely on comparisons of our findings with recent studies of diets of between 10 days and 12 weeks’ duration, and on changes in weight loss, liver size reduction, and metabolic parameters30,31,32. We believe the current study is the first to directly compare an MD with a VLCKD product for a duration of 2 weeks to identify which approach facilitated the most advantageous overall preoperative weight loss in patients with morbid obesity.
The specific VLCKD in our study, VLCKD-SDM, contained n-3 PUFA, whey protein, and probiotic and vitamin/mineral supplements, and the MD was based on normal foods with carefully prescribed content and measures. It was comprised of an amount of protein similar to that of other VLCKDs, with a greater amount of fat3,29,33. The program consisted of industrial foods with whey protein, with a level of carbohydrate 17–29% higher than that of other VLCKDs and 18–20% lower than in other VLCDs and LCDs. On the other hand, the Mediterranean diet we studied can only be discussed in the context of the Pro-MD product identified in the literature. The MD diet included protein and fat content that was 8–12% higher than that of Pro-MD9.
The short-term weight loss goal of 5–10% was thought to be safe and feasible. Patients on the VLCKD-SDM attained this goal fully; MD patients achieved 50.0% of this primary weight loss endpoint. The VLCKD-SDM resulted in significantly greater decreases in LDL, and HDL compared to the MD, and, significantly greater increases in vitamin B12 and D levels. VLCKD-SDM also achieved a greater reduction in median liver size (5.5% versus 1.7%). In our study, as in other studies, serum iron levels trended toward significant increases with the duration of diet therapy but remained within normal limits3. We did not assess the effect of the two diets on complications, as systematic reviews suggest that successful preoperative weight-loss diets do not necessarily confer protection against intraoperative risks or postoperative complications8.
Other presurgical diets are based predominantly on meal replacements consisting of whey-casein proteins with added micronutrients and macronutrients. Diets of this type include: industrial liquid formulations of VLCD, 400–800 kcal/day for 10 days–12 weeks2,4,7,30,31; normal food-based VLCDs, 400–800 kcal/day for 10 days–6 weeks3,6,18,32,33; industrial liquid formulations of LCDs, 800–1500 kcal/day for 3–7 weeks2,34,35,36; normal/industrial food-based LCDs, for 10 days–4 weeks (3,36); protein-based Mediterranean diets (Protein-MD), 1200 kcal/day for 8 weeks9; and very low-calorie ketogenic diets (VLCKD), 400–800 kcal/day for 10–30 days)3,29,33,37,38.
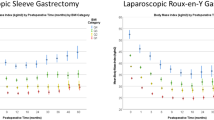
Recent short-term presurgical studies, randomized trials, and a systematic review provide a basis for estimating the relative effectiveness of VLCDs, industrial liquid formulations of VLCDs, normal food-based VLCDs, industrial liquid formulations of VLCDs, a Protein-MD, and VLCKDs on weight, BMI, waist circumference, fat percentage, lean body mass, nutrient content, triglycerides, high-density lipoprotein (HDL), and liver size2,3,4,5,6,7,8,9,10,11,12,14,27,28,29,30,31,32,33,34,35,36,37,38,39. As depicted in the reference Protein-MD and VLCKDs reviewed were equivalent to one another in achieving the greatest percentage fat loss and liver size reduction; VLCKDs were also most effective in increasing lean body mass. The reference Protein-MD resulted in the greatest weight loss and HDL reduction. The reference VLCKD-SDMs were dominant in reducing BMI and waist circumference. Essential nutrients were most increased by the reference industrial liquid formulations VLCDs; and triglycerides were most decreased by normal food based VLCDs.
No nutritional supplements were administered since MD contains a significant amount of nutrients and is balanced and healthy. Vitamins and probiotics were added to the ketogenic commercial meals consumed in VLCKD-SDM as they lacked appropriate vitamin and fiber content. With the nutritional supplements given to the ketogenic diet group, it was made sure that the two diet groups in this study had comparable ratios of all macronutrients, with the exception of protein and carbohydrates.
The contents of the two meals were assessed for these nutritional supplements, but whether they were in the same quantities was not determined. Although no calculations were conducted, it is believed that both groups' nutrients are relatively similar. The outcomes demonstrate this as well (Table 4). It was discovered that there were no statistically significant variations between these two diet groups' biochemical markers. In VLCKD-SDM, only vitamin B12 and vitamin D levels increased. This also has to do with supplements. High levels of vit B12 and D in VLCKD are thought to be related to supplementation. Patients on the MD diet did not receive vit D supplements according to the pre-diet blood levels of vit D. The impact on the biochemical outcomes might have been the same if MD had received B12 and vitamin D supplements in accordance with the levels of vitamin D in the blood. According to studies in the literature, patients' constipation and elevated ketone levels are caused by ketogenic industrial items. Based on these data, probiotic supplementation was administered. Fish eating is part of the healthy MD nutritional approach, hence was presented in MD. Patients with VLCKD-SDM were supplemented with n-3 PUFAs since fish could not be provided to them. Potassium was given in studies with VLCKD. This was given because it was a consensus. To ensure that the nutritional profiles of the two groups were comparable, n-3 PUFA supplementation was given to the VLCKD-SDM group in this study. They were not supplied separately as supplements since it was believed that these nutrients were satisfied by natural meals in the MD group. Therefore, giving n-3 PUFA supplements to VLCKD-SDM does not completely neutralize this superiority of MD.
In relating current results to that of the reference diets in terms of duration, the mean weight loss attained by patients in the 2-week VLCKD-SDM (7.3 ± 2.3 kg, total weight loss [TWL] 5.7%) was reached only by the reference industrial liquid formulations VLCDs and industrial liquid formulations of LCDs following 3–6 weeks. Weight loss achieved in the studied MD (3.4 ± 0.8 kg, TWL 2.6%) was approximately half that of the reference VLCKDs, more than half of the industrial liquid formulations VLCDs and industrial liquid formulations of LCDs, and equivalent to the normal food-based VLCDs and normal/industrial food-based LCDs.
The decrease in HDL levels was greater in VLCKD-SDM. Both total and VLCKD-SDM showed a positive correlation between post-diet HDL change and LBM levels (i.e., as HDL levels decreased, LBM levels also decreased, or vice versa) (Addendum Table 2). In the total group, a positive correlation was observed between post-diet HDL change and fat% and weight loss% (Addendum Table 1). It was observed that HDL decreased more with increasing weight loss, which is consistent with the literature3,6,40. As in the article, during the acute phase of weight loss, HDL levels fall as a result of a change in the activity of lecithin cholesterol ester transfer protein (LCAT), and when low body weight is stably maintained, HDL either rises to baseline levels or higher40. During weight loss therapy using VLCDs, HDL initially decreases, but then either increases to baseline levels or results in an overall improvement in HDL levels during weight maintenance3,6,40.
Reference diets, as a group, appeared to reduce liver size by between 12 and 30%. A systematic review of preoperative diets showed that liver size decreased on average by 15% (range 5–20%), though not with low-energy diets8. The greatest reduction in liver size among the reference diets was in the Protein-MD group and VLCKD group between 2 and 3 weeks. In VLCKD studies, the occurrence of ketonuria and ketonemia is evidence of compliance with the diet, wherein a 1-unit increase in ketonuria increased TWL by 2.0%3,6,37. In this context, the greater weight loss seen in the studied VLCKD-SDM group versus the MD group was likely associated with a higher satiety level related to the development of ketones.
Limitations
Limitations of our study included a relatively low number of patients, the short-term nature of the study, and the difficulty of comparing the studied diets to other reported diets of varying durations. Dividing the VLCKD-SDM group into two subgroups (one containing added n-3, one without it) would have provided additional insight into the most effective form of this diet.
The limitations of the study include that nutrients were not calculated in the same ratios in both groups before the diet, and supplements were not administered to our MD group based on pre-diet serum vitamin-mineral levels. Further research should be conducted by administering supplements in the same ratio to both groups.
Conclusions
Ketogenic diets have higher protein and lower carbohydrate content than MDs, and for this reason may be the superior preoperative 2-week weight-loss diet. The MD appears to require a significantly longer period of time to achieve similar results. The MD facilitated 50.0% less weight loss than the VLCKD-SDM. However, if the VLCKD-SDM results in gastrointestinal side effects, the MD can be effectively employed.
To the best of our knowledge, this is the first study to directly compare the preoperative effects of a VLCKD with a Mediterranean diet. The current findings showed that liver size was significantly decreased following both diets; however, the VLCKD-SDM, with its high whey protein content, sufficient pre-measured energy, n-3 PUFA, and a balance of macro and micro nutrients appeared significantly more effective than the Mediterranean diet in reducing weight prior to bariatric surgery.
Data availability
Raw data pertaining to this study are not publicly available outside of the university database for ethical reasons with the exception of its presentation in this analyzed article for publication in the medical literature. The data that support the findings of this study are openly available by reasonable request to the first author (Dr. Nihal Zekiye Erdem: nzerdem@yahoo.com).
References
NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 387(10026), 1377–1396 (2016).
Contreras, A. G. et al. Effects of two preoperatory weight loss diets on hepatic volume, metabolic parameters, and surgical complications in morbid obese bariatric surgery candidates: A randomized clinical trial. Obes. Surg. 28(12), 3756–3768. https://doi.org/10.1007/s11695-018-3413-7 (2018).
Leonetti, F. et al. Very low-carbohydrate ketogenic diet before bariatric surgery: Prospective evaluation of a sequential diet. Obes. Surg. 25(1), 64–71. https://doi.org/10.1007/s11695-014-1348-1 (2015).
Lewis, M. C. et al. Change in liver size and fat content after treatment with Optifast very low-calorie diet. Obes. Surg. 16(6), 697–701 (2006).
Tarnoff, M., Kaplan, L. M. & Shikora, S. An evidence-based assessment of preoperative weight loss in bariatric surgery. Obes. Surg. 18, 1059–1061. https://doi.org/10.1007/s11695-008-9603y (2008).
Faria, S. L., Faria, O. P., de Almeida, C. M. & Ito, M. K. Effects of a very low-calorie diet in the preoperative stage of bariatric surgery: A randomized trial. Surg. Obes. Relat. Dis. 11(1), 230–237. https://doi.org/10.1016/j.soard.2014.06.007 (2015).
Van Nieuwenhove, Y. et al. Preoperative very low-calorie diet and operative outcome after laparoscopic gastric bypass: A randomized multicenter study. Arch. Surg. 146(11), 1300–1305. https://doi.org/10.1001/archsurg.2011.273 (2011).
Holderbaum, M., Casagrande, D. S., Sussenbach, S. & Buss, C. Effects of very low-calorie diets on liver size and weight loss in the preoperative period of bariatric surgery: A systematic review. Surg. Obes. Relat. Dis. 14(2), 237–244. https://doi.org/10.1016/j.soard.2017.09.531 (2018).
Schiavo, L. et al. Clinical impact of Mediterranean-enriched-protein diet on liver size, visceral fat, fat mass, and fat-free mass in patients undergoing sleeve gastrectomy. Surg. Obes. Relat. Dis. 11(5), 1164–1170. https://doi.org/10.1016/j.soard.2015.04.003 (2015).
Alvarado, R. et al. The impact of preoperative weight loss in patients undergoing laparoscopic Roux-en-Y gastric bypass. Obes. Surg. 15(9), 1282–1286 (2005).
Still, C. D. et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch. Surg. 142(10), 994–998 (2007).
Isom, K. A. et al. Nutrition and metabolic support recommendations for the bariatric patient. Nutr. Clin. Pract. 29(6), 718–739. https://doi.org/10.1177/0884533614552850 (2014).
Mechanick, J. I. et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update. Co-sponsored by the American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery. Surg. Obes. Relat. Dis. 9(2), 159191 (2013).
Esposito, K., Kastorini, C. M., Panagiotakos, D. B. & Giugliano, D. Mediterranean diet and metabolic syndrome: An updated systematic review. Rev. Endocr. Metab. Disord. 14, 255–263 (2013).
Merdol, T. K. Standard Recipes 171–184 (Alp Offset Printing, 2014).
Beslenme Bilgi Sistemi Nutrition Information System (BeBiS) database software program. Ebispro for Windows 8.0. Entwickelt an der Universitat Hohenheim; Stuttgart, Germany, 2010. Turkish Version (BEBIS), Pasifik Elektirik Elektronik Ltd. Şti. www.bebis.com.tr; Istanbul.
Frisancho, A. R. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am. J. Clin. Nutr. 40, 808–819 (1984).
Lohman, T. G. et al. (eds) Anthropometric Standardization Reference Manual (Kinetics Books, 1988).
Dagan, S. S. et al. Inadequate protein intake after laparoscopic sleeve gastrectomy surgery is associated with a greater fat free mass loss. Surg. Obes. Relat. Dis. 13(1), 101–110 (2017).
Schofield, W. N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 39(1), 5–41 (1985).
Mahan, L. K. & Raymond, J. L. Krause’s Food and the Nutrition Care Process 390–412 (Elsevier, 2017).
Bishop, C. W., Bowen, P. E. & Ritchey, S. J. Norms for nutritional assessment of American adults by upper arm anthropometry. Am. J. Clin. Nutr. 34, 2530–2539 (1981).
Buzby, G. P. et al. Study protocol: A randomized clinical trial of TPN in malnourished surgical patients. Am. J. Clin. Nutr. 47, 366–381 (1988).
Patzak, M. et al. Assessment of liver size by ultrasonography. J. Clin. Ultrasound. 42(7), 399–404 (2014).
Keys, A. et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 124, 903–915 (1968).
Toobert, D. J. et al. Biologic and quality-of-life outcomes from the Mediterranean Lifestyle Program: A randomized clinical trial. Diabetes Care 26(8), 2288–2293. https://doi.org/10.2337/diacare.26.8.2288 (2003).
Gerhard, G. T. et al. Effects of a low-fat diet compared with those of a high-monounsaturated fat diet on body weight, plasma lipids and lipoproteins, and glycemic control in type 2 diabetes. Am. J. Clin. Nutr.. 80(3), 668–673. https://doi.org/10.1093/ajcn/80.3.668 (2004).
Viscogliosi, G. et al. Mediterranean dietary pattern adherence: Associations with prediabetes, metabolic syndrome, and related microinflammation. Metab. Syn. Relat. Dis. 2013, 210–216. https://doi.org/10.1089/met.2012.0168 (2013).
Yolsuriyanwong, K. et al. Effectiveness, compliance, and acceptability of preoperative weight loss with a liquid very low-calorie diet before bariatric surgery in real practice. Obes. Surg. 29(1), 54–60. https://doi.org/10.1007/s11695-018-3444-0 (2019).
Colles, S. L. et al. Preoperative weight loss with a very low-energy diet: Quantitation of changes in liver and abdominal fat by serial imaging. Am. J. Clin. Nutr.. 84, 304–311 (2006).
Collins, J. et al. Preoperative weight loss in high-risk superobese bariatric patients: A computed tomography-based analysis. Surg. Obes. Relat. Dis. 7(4), 480–485. https://doi.org/10.1016/j.soard.2010.09.026 (2011).
González-Pérez, J. et al. Clinical impact of a 6-week preoperative very low-calorie diet on body weight and liver size in morbidly obese patients. Obes. Surg. 23, 1624–1631 (2013).
Albanese, A. et al. Pre-operative very low-calorie ketogenic diet (VLCKD) vs very low-calorie diet (VLCD): Surgical impact. Obes. Surg. 29, 292–296 (2019).
Edholm, D. et al. Preoperative 4-week low-calorie diet reduces liver volume and intrahepatic fat, and facilitates laparoscopic gastric bypass in morbidly obese. Obes. Surg. 2, 345–350 (2011).
Nielsen, L. V., Nielsen, M. S., Schmidt, J. B., Pedersen, S. D. & Sjödin, A. Efficacy of a liquid low-energy formula diet in achieving preoperative target weight loss before bariatric surgery. J. Nutr. Sci. 5, 1–7. https://doi.org/10.1017/jns.2016.13 (2016).
Benjaminov, O. et al. The effect of a low-carbohydrate diet on the nonalcoholic fatty liver in morbidly obese patients before bariatric surgery. Surg. Endosc. 21, 1423 (2007).
Pilone, V. et al. Metabolic effects, safety, and acceptability of very low-calorie ketogenic dietetics scheme on candidates for bariatric surgery. Surg. Obes. Relat. Dis. 14, 1013–1019 (2018).
Ministrini, S. et al. Lysosomal acid lipase as a molecular target of the very low carbohydrate ketogenic diet in morbidly obese patients: The potential effects on liver steatosis and cardiovascular risk factors. J. Clin. Med. 8, 621–633. https://doi.org/10.3390/jcm8050621 (2019).
Fris, R. J. Preoperative low energy diet diminishes liver size. Obes. Surg. 14, 1165–1170 (2004).
Rolland, C. & Broom, I. The effects of very-low-calorie diets on HDL: A review. Cholesterol https://doi.org/10.1155/2011/306278 (2011).
Acknowledgements
The authors are grateful to Prof. Dr. Mustafa Taskın for his excellent assistance during the study. We thank J.N. Buchwald, Medwrite Medical Communications, and T.W. McGlennon, McGlennon MotiMetrics, Maiden Rock, WI, USA who received a grant for substantial assistance with statistical analysis and manuscript development.
Author information
Authors and Affiliations
Contributions
Equal contributions to the development of the manuscript were made by the four co-authors. N.Z.E. was responsible for designing the study, drafting the protocol and report, conducting literature review, developing database and analyzing data, interpreting results, developing the reference list, creating tables, and reviewing all drafts. D.O. was responsible for screening potentially eligible studies, contributing to writing the report, extracting and analyzing data, and reviewing drafts. H.E.T. contributed to writing the report, interpreting results, developing figures, and reviewing manuscript drafts. F.M.A. participated in designing the study, drafting the protocol and report, performing the surgery, interpreting results, and reviewing all drafts.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Erdem, N.Z., Ozelgun, D., Taskin, H.E. et al. Comparison of a pre-bariatric surgery very low-calorie ketogenic diet and the Mediterranean diet effects on weight loss, metabolic parameters, and liver size reduction. Sci Rep 12, 20686 (2022). https://doi.org/10.1038/s41598-022-24959-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-24959-z
This article is cited by
-
Ketogenic nutritional therapy (KeNuT)—a multi-step dietary model with meal replacements for the management of obesity and its related metabolic disorders: a consensus statement from the working group of the Club of the Italian Society of Endocrinology (SIE)—diet therapies in endocrinology and metabolism
Journal of Endocrinological Investigation (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
