
Abstract
To support point-of-care decision making by presenting outcomes of past treatment choices for cohorts of similar patients based on observational data from electronic health records (EHRs), a machine-learning precision cohort treatment option (PCTO) workflow consisting of (1) data extraction, (2) similarity model training, (3) precision cohort identification, and (4) treatment options analysis was developed. The similarity model is used to dynamically create a cohort of similar patients, to inform clinical decisions about an individual patient. The workflow was implemented using EHR data from a large health care provider for three different highly prevalent chronic diseases: hypertension (HTN), type 2 diabetes mellitus (T2DM), and hyperlipidemia (HL). A retrospective analysis demonstrated that treatment options with better outcomes were available for a majority of cases (75%, 74%, 85% for HTN, T2DM, HL, respectively). The models for HTN and T2DM were deployed in a pilot study with primary care physicians using it during clinic visits. A novel data-analytic workflow was developed to create patient-similarity models that dynamically generate personalized treatment insights at the point-of-care. By leveraging both knowledge-driven treatment guidelines and data-driven EHR data, physicians can incorporate real-world evidence in their medical decision-making process when considering treatment options for individual patients.
Similar content being viewed by others

Introduction
Management of chronic disease is a global challenge. In the US, 86% of people over 65 have at least one chronic condition1. To help manage the care of patients with chronic diseases, physicians use treatment guidelines, results of randomized clinical trials (RCTs), and their own patient-panel experience, to inform treatment decisions for individual patients. Treatment guidelines are usually based on the results of RCTs and expert opinions2. What is not widely appreciated, however, is that only a small minority of patients could actually meet the inclusion/exclusion eligibility criteria for clinical trials, thus substantially limiting the generalizability of the trial results and the applicability of common clinical guidelines3,4. Consequently, to make treatment decisions for individual patients, physicians often draw on their own experience, however the number of patients in their panel who are similar to a specific patient is very limited5. The rapid adoption of electronic health records (EHRs) has led to the capture of health information on millions of patients, with detailed longitudinal information including demographics, diagnoses, medications, diseases, laboratory observations, procedure orders, and associated outcomes3,6,7. Each medication order, laboratory order, or procedure order recorded in the EHR can be viewed as an intervention8,9. In this paper, we analyze the outcomes of individual patient medication treatment decisions.
Our approach provides information about the outcomes of similar patients in a similar clinical situation to the patient of interest, which we call a Precision Cohort, at the point-of-care. During a clinic visit, our system dynamically creates a precision cohort of clinically similar patient decision points. It then generates distributional and comparative statistics of the resulting outcomes of diverse treatment options administered to other patients in the precision cohort. We demonstrate the suitability of the approach by implementing it using EHR data from a large health care provider for three chronic diseases: hypertension (HTN), type 2 diabetes mellitus (T2DM), and hyperlipidemia (HL). A retrospective analysis demonstrated that treatment options with better outcomes were available for a majority of cases across the three diseases: 75%, 74%, 85% for HTN, T2DM, HL, respectively. The resultant models for HTN and T2DM were actively used by primary care physicians (PCPs) during clinic visits, in a pilot study.
Background
Work on developing and applying patient similarity is not new10,11. Some work focused on the development of methods to compute patient similarity, to assist in identifying clinically similar patients: for example, by developing a locally supervised metric learning (LSML) method that can automatically learn disease-specific similarity metrics12, by applying multiple similarity criteria depending on variable types13, by analyzing images14, and by identifying genetic similarities15. Common approaches to identify groups of patients with similar time-dependent characteristics include time-series analysis methods16,17,18 and clustering techniques19,20. Other work has focused on the application of patient similarity to specific use cases: e.g., for predicting disease onset risk21,22, drug effectiveness23, identifying disease sub-phenotypes24, personalized risk factors25, personalizing blood glucose prediction26, and diagnosing chronic diseases27. There has also been work on clinical decision support (CDS) approaches that leverage patient similarity. These include:
-
A system that uses clinical data (originating in notes and structured fields), to map a patient to a position in a clinical pathway (extracted from guidelines) to inform treatment28,
-
A system for individualized cancer treatments, by predicting an individual’s responsiveness to different treatments, based on gene expression profiles29,
-
A system to identify a patient as a candidate for a specific treatment, that includes methods to create patient clusters a priori, based on a collection of clinical characteristics with an associated desired treatment, as well as methods to efficiently create patient clusters 30, and
-
A system that generates a patient trajectory graph from EHR data, capturing conditions, associated outcomes, and medical interventions, and suggests medical guidelines at patient group/cluster levels31.
Our precision cohort treatment options (PCTO) approach differs from these existing CDS approaches in the following ways:
-
(1)
It identifies and extracts appropriate disease-specific “clinical treatment decision points” from the longitudinal patient EHR data to use as the primary events of interest for modeling and analysis,
-
(2)
It selects variables for assessing patient similarity leveraging multiple sources of information: (a) variables associated with the propensity of receiving treatment derived from knowledge-driven clinical guidelines, and (b) variables associated with disease control outcomes using data-driven variable construction and feature selection from EHR data,
-
(3)
It dynamically creates, at runtime, a precision cohort of patient events that are clinically similar to the current state of the patient of interest (instead of using static pre-computed patient cohorts), and
-
(4)
It personalizes the treatment options by augmenting them with outcome and distributional statistics, based on retrospective analysis of the precision cohort.
Our high-level goal—to help clinicians leverage aggregated de-identified patient data for improved decision making at the point of care is—aligned with that of the “Green Button” (GB) approach8. The GB authors suggest that deploying a green “patients like mine” button as a tool in the EHR would support patient care decisions in the absence of published evidence. The GB represents personalized cohorts of retrospective observational data, constructed at the point of care, that can be analyzed to provide actionable clinical insights32. GB has been implemented as an informatics consult service at Stanford Medical Center33,34. Some key differences between our PCTO approach and the GB approach are: (1) PCTO is designed to support specific chronic diseases whereas the GB process is potentially applicable for any condition, (2) PCTO has an automated runtime to generate personalized treatment option insights in real-time whereas GB is implemented via an offline specialty consult service, (3) PCTO and GB leverage different algorithms and methods in the implementation of the main workflow components: clinical event extraction, patient similarity assessment, cohort construction, and treatment/outcome analysis.
Methods
As illustrated in Fig. 1, the PCTO workflow consists of four major steps: (1) data extraction, (2) similarity model training, (3) precision cohort identification, and (4) treatment options and outcomes analysis. Steps 1 and 2 make up the training stage, which is performed offline (and in advance). Steps 3 and 4 form the runtime stage used in real-time, during the patient visit encounter. The workflow processing was implemented using a combination of SQL, Python, and R35,36.

High-level Precision Cohort Treatment Options (PCTO) workflow. The PCTO workflow consists of four major steps: (1) data extraction, (2) similarity model training, (3) precision cohort identification, and 4) treatment options analysis. Steps 1 and 2 make up the training stage which is performed offline and in advance. Steps 3 and 4 form the runtime stage which is used in real-time during the patient visit encounter.
Data extraction
A four-step data extraction process was performed on the clinical treatment guidelines and EHR data, to create a training data set and a scoring data set. The training data set was used to train a model for computing patient similarity. The scoring data set served as the repository of clinical events used to create the precision cohorts at runtime. Table 1 describes each step in the data extraction process, including the method used (manual or automatic) and the domain knowledge needed (clinical or data science).
The first step was identifying and extracting appropriate points in time from the EHR, to serve as the events of interest for subsequent modeling and analysis. We identified outpatient encounters, during which a patient’s condition was not controlled, as ‘decision points’ (DPs), since they represent opportunities to initiate a change in treatment plans. The DPs were drawn from all office encounters regardless of department, and include primary care and specialist visits (refill encounters were excluded). It is common for one patient to have multiple DPs over the course of their health history. As illustrated in Fig. 2, each clinical DP is associated with a date (index date), a preceding baseline period, and an observation period that follows. Data in the baseline period were used to extract baseline variables capturing the health condition and active treatment status at the DP. Observed treatment decisions were identified at the DP, with a limited time buffer to allow for delays in treatment initiation. Data in the follow-up observation period were analyzed to determine the associated outcome status (i.e., disease controlled or uncontrolled). The selection criteria for the DPs, duration of the baseline and follow-up periods, specification of the baseline variables, identification of the treatment options, and definition of the outcomes are disease-specific and were determined by clinical expert domain knowledge. Clinical outcomes were used because of their links to important health outcomes (e.g., mortality, significant clinical events). Once all of these criteria were in place, data extraction and variable construction scripts were configured and run on the EHR data, to identify the DPs.

Decision point specification. Each clinical decision point is associated with an index date, a baseline period that precedes the decision point, and an observation period that follows the decision point. Data in the baseline period are processed to extract baseline variables to represent the health condition and active treatment status. Observed treatment decisions are identified at the time of the decision point. Data in the follow-up observation period are analyzed to determine the associated outcome status.
The second step was the manual identification of variables derived from knowledge-driven clinical guidelines. After relevant disease-specific clinical guideline documents were identified, clinical domain experts manually reviewed the published guidelines, not to extract or replicate the treatment logic, but to identify (1) the universe of recommended treatments, and (2) all of the variables used in making the treatment decisions. The recommended treatments were used to limit the treatment options considered to those that are clinically acceptable. In this work, only pharmacologic treatments were considered. Since the identified variables are associated with the propensity of receiving specific treatments, they were treated as baseline confounders for adjustment in the subsequent analysis. A subset of these variables was manually selected based on their clinical significance to be “exact match” or “filter” variables (used in the filtering step of the precision cohort construction). The remaining variables were included in the salient variable selection process (step 4).
The third step was the identification of variables from the EHR using clinical-domain-knowledge-specified variable template definitions, and implemented via automated data extraction and variable construction tools. The goal was to extract as much potentially useful information from the EHR as possible. Thousands of variables were generated by this data-driven process. Medication variables were constructed based on RxNorm concept unique identifier (RxCUI) clinical drug codes37. Lab variables were constructed based on Logical Observation Identifiers Names and Codes (LOINC) codes38. Disease variables were constructed based on the Agency for Healthcare Research and Quality’s Clinical Classifications Software (CCS) categories39, using codes from the International Classification of Diseases (ICD) 9th and 10th revisions40,41.
The fourth step was the selection of the most salient variables associated with the outcome of interest (i.e., disease control), from the pool of variables extracted from the guidelines in Step 2 and from the EHR data in Step 3. The variable selection process combined an initial automatic data-driven pass using stability ranking feature selection42 (to reduce the number of candidate variables) with a final manual review pass guided by clinical domain expertise. The stability selection constructed 200 different L1-regularized logistic regression models43. Each model used a random subset (75%) of the DPs and generated a set of selected features. Features that appeared consistently across many of the models were considered stable. In our implementation, only highly stable features that were selected by at least 150 of the 200 models (≥ 75%) were chosen. Data-driven correlation and clustering analysis were then performed to link highly related variables from the initial pass, to facilitate subsequent clinical review. The final manual adjudication and selection were performed, considering whether the variable was physiologically nonsensical, duplicative, or unaddressable (i.e., unmodifiable). The resulting set of variables for HTN, T2DM, and HL are described in Supplementary Tables S1, S2, and S3 online, respectively.
The result of this data extraction process was a data frame where the rows consisted of individual DPs and the columns included the treatment decision, the associated outcome, and the selected baseline variables. Only DPs with no missing variable values were retained. A random sample of the rows was selected to form the training data set and the remaining rows made up the scoring data set.
Similarity model training
In step 2, the training data set was used to train a model for computing patient similarity. There were several challenges in training the similarity model. One challenge was that patient similarity is context dependent: two patients may be very similar to each other with respect to HTN but may differ from each other with respect to T2DM, as each disease is unique in its characteristics and etiology. The use of static similarity measures, e.g., Euclidean or Mahalanobis, for all disease conditions, may not be optimal. The similarity measure must therefore be specifically tailored to each disease. A second challenge was that the dimensionality of the variable space was very large. With all the diseases, medications, procedures, lab tests, and patient characteristics, there were thousands of variables to consider. To address these challenges, we used machine learning methods to learn the best metric from the data automatically. Specifically, we used a trainable similarity measure called locally supervised metric learning (LSML) that can be customized for a specific disease condition12. The method learns a disease-specific distance measure that is a generalization of the Mahalanobis distance: \({D}_{LSML}({{\varvec{x}}}_{i},{{\varvec{x}}}_{j})=\sqrt{{({{\varvec{x}}}_{i}-{{\varvec{x}}}_{j})}^{T}{\varvec{W}}{{\varvec{W}}}^{T}({{\varvec{x}}}_{i}-{{\varvec{x}}}_{j})}\), where \({{\varvec{x}}}_{i}\) and \({{\varvec{x}}}_{j}\) are the patient variable vectors for patients i and j respectively and W is a transformation weight matrix that is learned from the training data. LSML is formulated as an average neighborhood margin maximization problem and tries to find a weight matrix W where the local class discriminability (e.g., disease-controlled status) is maximized (i.e., the variable weights are determined based on their relative effect on patient outcomes). In this work, a separate LSML similarity measure was trained for each disease condition, and then used during runtime to generate the precision cohorts. The automatically learned similarity weights for each variable (computed as \({1}^{T}{\varvec{W}}{{\varvec{W}}}^{T}\)) for HTN, T2DM, and HL are shown in Supplementary Tables S1, S2, and S3 online, respectively.
Precision cohort identification
In step 3, a precision cohort of clinically similar patient DPs was dynamically created, at runtime, based on the data for the patient of interest at the point of care. Since the precision cohort will be used to identify the different observed treatment options, and to compare their treatment effects, the precision cohort construction process can be viewed as an approach to adjust for baseline confounders, to ensure that the treatment effect analyses are valid. Several causal inference methods can be used to adjust for baseline confounders, including matching, stratification or regression, standardization or inverse probability weighting, g-estimation, or doubly robust methods44,45. Although the methods have different tradeoffs in terms of capabilities and complexity45, when applied appropriately, any of these methods can be used to reduce bias in the treatment effect analyses for our use case. To align with how clinicians identify and select similar patient events, we used a multi-step matching based approach46, where the goal was to select DPs that are very similar, if not identical, to (a) one another, and (b) the current state of the patient of interest, in all respects except for one: the treatment decision at the time of the DP. The “covariate balance” of the DPs in the “no treatment change” group versus the “treatment change” group was used to assess bias and matching validity47,48. Covariate balance was estimated using the “standardized bias,” which was computed as the difference in means of each covariate between the two groups, divided by the standard deviation in the full treated group—smaller values closer to 0 represent better balance. The precision cohort construction process involved: (1) filtering the DPs in the scoring set, to only keep those that have identical values of the filter variables as the patient of interest, (2) computing similarity scores for the filtered DPs, using the disease-specific similarity model, and (3) ranking the DPs based on the similarity score, and selecting the most similar subset based on a tradeoff between reasonable cohort size and good covariate balance. An illustrative example of this process for one HTN patient of interest is shown in Fig. 3.

An illustration of the precision cohort construction process for one hypertension (HTN) patient of interest. (A) The cohort starts with all approximately 733,000 decision points in the scoring set, is reduced to approximately 130,000 after filtering based on the filter variables, and finally to approximately 15,000 after similarity scoring, ranking, and selection. (B) A histogram of the similarity scores for the 130,000 decision points after filtering. Those with scores closer to 0 are more similar to the patient of interest. Even when considering decision points with identical filter variables as the patient of interest, there are still many that are not very similar. Overlaid on the histogram is a plot of the covariate balance as a function of the similarity score threshold (red curve). As expected, there is a tradeoff between cohort size and covariate balance. As the cohort grows, there is more diversity, which results in less balance and higher values of the covariate balance score. A hyperparameter grid search approach can be used to find a similarity score threshold that results in a reasonably sized precision cohort with good covariate balance. In this example, a similarity score threshold of 0.7 is selected, with a covariate balance < 0.03, resulting in a precision cohort of approximately 15,000 decision points.
Treatment options analysis
In step 4, a retrospective analysis was performed on the DPs in the precision cohort, to generate personalized treatment options for the individual patient of interest. This was done by first grouping the DPs by the observed treatment decision, at the time of the DP, and then, for each of these treatment option groups, computing: (1) the size of the group (number of DPs), (2) the follow-up outcome (percent controlled), (3) the difference in the outcome compared to the “no treatment change” baseline option, and (4) a statistical significance assessment of this outcome difference using a Bonferroni corrected \({\chi }^{2}\) p-value threshold of 0.05 to adjust for multiple testing49. The outcome comparisons for various treatment options were presented graphically to physicians, in real-time, within the EHR system, as a modified Sankey diagram50 (Fig. 4). As part of the clinical pilot study, we purposefully designed a visualization of the precision-cohort analysis for use by the practicing clinician at the point-of-care. We tested prototype displays through iterative feedback sessions. The final visualization appeared as a frame within the clinic’s EHR system (Supplementary Fig. S4). Because RCTs are infrequently conducted using head-to-head comparisons of treatment alternatives (new interventions are commonly tested against placebo), it is unusual for physicians to receive comparative data on medication alternatives. We found that physicians in our pilot group understood the Sankey-diagram presentation accurately.

Personalized treatment options and associated outcomes in a precision cohort using a Sankey diagram. (1) The initial node (black) represents all decision points in the precision cohort for the individual patient of interest who has an HTN diagnosis, is over age 65, and is on Lisinopril (ACEI). (2) Each pathway leaving the initial node is a different treatment decision that is observed in the data. The thickness of the edge is proportional to the number of decision points. The label contains the medication class and ingredient, the start or stop of the medication (“+” or “−” suffix), and the percentage (in parentheses) of decision points under control in the follow-up. The “no change” or “stay the current course” treatment option is shown in gray and is considered the “baseline” treatment option. (3) The terminal nodes represent the outcome for the disease condition under control (green) and not under control (red). (4) Treatment options associated with better control than the baseline are shown as green pathways above the baseline with dark green indicating statistical significance. (5) Treatment options associated with worse control than the baseline are shown as red pathways below the baseline with dark red indicating statistical significance.
Results
Study design
The PCTO workflow was applied to de-identified EHR data from a large health care provider in eastern Massachusetts, containing over 20 years of longitudinal data for approximately 2.5 million patients, for three disease conditions: HTN, T2DM, and HL. The Western Institutional Review Board (WIRB) had reviewed the study and gave it an exemption as a human subjects study. The decision-point criteria and characteristics for the three disease conditions are described in Table 2. The table lists the clinical treatment guidelines referenced, the start and end dates of the study period used for extracting data from the EHR, the decision-point criteria, the specifications for the baseline period, baseline variables, treatment options, follow-up period, and outcome. The clinical treatment guidelines were selected based on what was currently in use at the pilot health system. The study period was selected to include data covered by the time of the JNC7 publication to the present (for HTN), and the most recent 10 years of data (for T2DM and HL), so only recent and relevant treatments and practice patterns are included. The DP criteria, baseline period, follow-up period, and outcome specifications were based on clinic expert opinion. The baseline variables were derived using the process described in “Data extraction”. The treatment options were manually extracted from the guidelines, so only clinically acceptable treatments were included. Finally, the table shows the number of unique patients selected, and the number of DPs extracted based on these criteria. After the DP extraction, 50,000 DPs were selected at random to form the training data set. The remaining DPs were used as the scoring data set, following the process described in “Data extraction”. A disease-specific LSML similarity measure was trained using the training data set as described in “Similarity model training”. To perform runtime analysis, a leave-one-out cross-validation (LOOCV) approach51 was adopted. Each DP in the scoring data set was selected, in turn, to represent the individual patient’s office visit. That DP was then removed from the scoring data set, and the precision cohort identification (from “Precision cohort identification”) and treatment options analysis (from “Treatment Options Analysis”) were performed using the selected DP of interest and the updated scoring data set. Finally, the personalized treatment option outputs were aggregated and analyzed. The following sections present results from analyzing the data and output for individual DPs, groups of DPs, and all DPs.
In terms of computational cost, the extraction of the data to create the training and scoring data sets typically took under one processor-hour. Creating a new scoring model took between 4 to 8 processor-hours, and the dynamic generation of the precision cohort and personalized treatment options report for an individual patient of interest took a few processor-seconds. The entire LOOCV analysis typically took 3000 processor-hours (since all DPs had to be processed). However, since the runtime was parallelizable, the analysis was performed on a cluster of approximately 160 processors, thus providing results within a day.
Filter variable cohorts
The largest observed cohorts based on the “exact match” filter variables for HTN, T2DM, and HL are shown in Supplementary Figs. S5, S6, and S7, online, respectively. Since the filter variables capture the active treatments and key patient characteristics used to inform treatment decisions (based on the clinical guidelines), these cohorts represent the most commonly observed active treatment combinations at the DPs. Although there is a large number of cohorts (32,656 for HTN, 1867 for T2DM, and 253 for HL), it is much less than all the possible combinations (290 for HTN, 248 for T2DM, and 214 for HL); moreover the cumulative coverage curve indicates that most DPs belong to only a small number of cohorts (40% in the top 10 cohorts for HTN, 62% for T2DM, and 91% for HL) and that there is a long tail (70% of the groups have less than five DPs for HTN, 60% for T2DM, and 34% for HL). These observations are consistent with other published findings where the number of unique treatment pathways for HTN and T2D is large and diverse52. Unsurprisingly, the largest cohorts are those that are not currently on any treatment, followed by cohorts that are only on a single treatment (e.g., Lisinopril for HTN, Metformin for T2DM, and Simvastatin for HL). For HTN and T2D, the size of the “no treatment” cohorts may be increased because the selection criteria (Table 2) can include DPs where the patient does not have an official disease diagnosis (i.e., based only on abnormal lab test measurements). It is also possible that some diagnosed patients are only on lifestyle (e.g., diet and exercise) modification treatments that are not explicitly tracked in the analysis. Although an explicit disease diagnosis is required for HL, there is variability in the initiation of pharmacologic treatment based on LDL levels, which results in more “no treatment” DPs (especially for younger patients and those with borderline LDL levels)53. In addition, similar to HTN and T2D, some HL patients may only be on non-medication lifestyle modification treatments.
Global treatment options
The largest observed global treatment option decisions across all DPs for HTN, T2DM, and HL are shown in Supplementary Figs. S8, S9, and S10 online, respectively. Across all three conditions, the most common treatment decision is to “stay the current course” and make no change to the current medication-treatment ingredient (81% for HTN, 85% for T2DM, and 94% for HL). Note that since the dosage was not considered, treatment decisions that only changed the dosage appeared as refills and were considered “no ingredient change.” For HTN and T2DM, some no-change treatments reflect no active pharmacologic treatments for undiagnosed patients. Even for undiagnosed patients who have measurement-proven conditions, however, “clinical inertia” occurs when a PCP does not treat a condition that is not under control. Due to the large number of DPs without any active treatments, the next most common set of treatment option decisions are the start of first-line medications: Lisinopril (ACEI) and Hydrochlorothiazide (thiazide diuretic) for HTN, Metformin (biguanides) for T2DM, and Simvastatin and Atorvastatin (statin) for HL. Overall, there are many treatment option decisions (3966 for HTN, 883 for T2DM, and 223 for HL). However, many are unique and have only a single DP (60% for HTN, 53% for T2DM, and 29% for HL), again consistent with prior findings on the uniqueness of treatment pathways52. In terms of treatment decisions that switch ingredients within the same class, it is interesting to note that, for T2DM, the most common are Sulfonylurea changes: stopping Glyburide and starting Glipizide or Glimepiride. For HL, the most common are Statin changes: stopping Simvastatin and starting Atorvastatin, Pravastatin, or Rosuvastatin.
Personalized treatment options
Figure 4 illustrates the patient-level personalized treatment options and associated outcomes, resulting from applying the PCTO analysis to a single DP for an individual patient. In this case, the patient has an HTN diagnosis, is over age 65, and is on Lisinopril (ACEI) at the time of the DP. In addition to identifying treatment options that have statistically significantly better outcomes (dark green pathways) than the baseline “no change” treatment option (grey pathway), the analysis also lists treatment options that have significantly worse outcomes (dark red pathways). Options in light green or light red have better or worse outcomes, respectively, but are not statistically significant. The complexity of each treatment option, estimated as the number of unique medications, is also available.
DPs from different filter variable cohorts are expected to have different personalized treatment options. For example, Fig. 5A shows the treatment options for a DP, in a group that is over age 60, and on Hydrochlorothiazide (Thiazide), while Fig. 5B shows the treatment options for a DP, in a group that is over age 60, and on Lisinopril (ACEI). The treatment options associated with significantly better-than-the-baseline outcomes (dark green pathways), for these two DPs, are different: in Fig. 5A, it is adding Lisinopril (ACEI), while in Fig. 5B, it is adding either Amlodipine (CCB) or a Thiazide (Hydrochlorothiazide or Chlorthalidone). However, patient DPs that belong to the same filter variable cohort can also have different personalized treatment options. Figure 5C shows the personalized treatment options for a patient DP that belongs to the same group as Fig. 5B [over age 60 and on Lisinopril (ACEI)], but the effective treatment options here are different: only adding Hydrochlorothiazide passes the selection criteria. Since the precision cohort is created dynamically for each patient DP, based on its specific characteristics, the composition of the precision cohort can differ, resulting in different personalized treatment options.

Personalized treatment options for three different HTN patient decision points. (A) The patient decision point belongs to a filter variable group that is over age 60 and on Hydrochlorothiazide (Thiazide). (B, C) The patient decision point belongs to a filter variable group that is over age 60 and on Lisinopril (ACEI). Note that the treatment options associated with significantly better control (dark green pathways) across the three patient decision points are different.
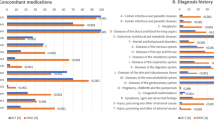
To assess the applicability and potential impact of the PCTO method, and to better understand its behavioral characteristics, all DPs in the scoring data set were processed using the LOOCV strategy described in “Results”; the results are summarized in Supplementary Figs. S11, S12, and S13 online (for HTN, T2DM, and HL, respectively). Each figure shows the number of DPs, grouped by filter variable cohorts (rows), and the percentage of DPs that have personalized treatment options with statistically significantly better outcome (green), with fewer medications (purple), with the same number medications (yellow), and with more medications (red). As expected, filter variable cohorts with no active medication treatments (e.g., “All guideline variables false” for all conditions, “age_60_or_above” for HTN, “T2D” for HL) have the largest percentage with significantly better treatment options. For HTN, it is interesting to note that for the African American (“black”) group on no active HTN medications, only 70% of the DPs have treatment options with statistically significantly better outcomes compared to taking no HTN medications. Similar behavior is seen in the diabetes (“dm”) group on no active HTN medications where only 78% of the DPs have treatment options with statistically significantly better outcomes. This implies that it may be more challenging to control HTN for patients that are black or have diabetes and is consistent with prior findings54,55. With a few exceptions, filter variable cohorts with one active medication treatment (e.g., “ACEI_Lisinopril” or “Thiazide_Hydrochlorothiazide” for HTN, “Biguanides_Metformin” and “Sulfonylurea_Glyburide” for T2DM, and “Statin_Simvastatin” and “Statin_Pravastatin” for HL) have the next largest percentage with significantly better treatment options. The notable exceptions are “Beta_Blockers_Metoprolol” for HTN, “Insulin_Glargine” for T2DM, and “Statin_Atorvastatin” and “Statin_Rosuvastatin” for HL. Indeed, beta blockers for HTN and insulin for T2DM are not typically first-line treatments, and patients on these medications likely have already tried (unsuccessfully) other medications before settling on these. For HL, atorvastatin and rosuvastatin are the most effective statins available56 and would be difficult to improve upon. Recognizing that successful disease management should not only consider disease control, but other factors such as treatment complexity and cost57, information about the number of medications relative to the baseline (fewer, same, more) for each treatment option is also computed. Across the three diseases, many filter variable cohorts that are on multiple medications, have treatment options with fewer or the same number of medications with comparable outcomes (percent controlled). Treatment options with more medications are almost always possible. The impact and utility of PCTO are dependent on the specific filter variable cohort, but overall, 75%, 74%, and 85% of all the DPs for HTN, T2DM, and HL, respectively, have at least one significantly better treatment option identified.
Discussion
Physicians are encouraged to base treatment decisions on clinical guidelines, where available. Unfortunately, the evidence basis for clinical guidelines relies on the results of RCTs whose inclusion/exclusion criteria exclude the majority of the population. That makes it difficult to appropriately extrapolate the experience from clinical trials to the general population, or to individual patients. Similarly, generating an analysis of undifferentiated observational data derived from the experiences of the general population, would not lead to insights sufficiently relevant to a particular patient.
We developed an analytic workflow to create precision cohorts representing patients similar to the patient of interest, using a model derived from machine learning. Tracking and analyzing the clinical responses of similar patients in similar clinical situations, when prescribed various medication treatments, provides physicians with observational data from real-world experience as input to inform decisions about an individual patient. Our analysis of historical observational data does not lead to recommended actions, nor does it replace clinical guidelines. These analyses supplement guidelines based on RCTs and expert opinion and require human judgment to appropriately incorporate the results of the statistical analysis into medical decision making.
The PCTO workflow, summarized in Fig. 1, can be applied to any disease condition, as long as the necessary data and criteria are provided. For the results presented in “Results”, the specific criteria were finalized after several iterations of a specification, implementation, analysis, and review process involving both data scientists and clinicians, and represent just one set of clinically relevant use cases for HTN, T2DM, and HL.
There are several limitations to the current work. Due to data availability, only medication-based treatment options were considered, and dosage information was not available. As mentioned in “Results”, this limited the granularity of the analysis: non-pharmacologic treatments would appear as “no treatment” and changes only in drug dose would appear as “no change in drug class.” Since nothing in the method explicitly precludes handling additional treatment types, a natural extension would be to include non-pharmacologic treatment options such as diet, exercise, smoking cessation, and other lifestyle modifications or interventions, to ameliorate unfavorable social determinants of health (SDOH), as long as the necessary data is available. Dosage information, if available, could also be included to differentiate the treatment options.
The study only explored three chronic conditions: HTN, T2DM, and HL. The method should be applied to other common chronic disease conditions (e.g., chronic obstructive pulmonary disease and congestive heart failure) to better understand how the method can generalize.
The patient characteristics used to create the precision cohorts in the pilot were limited to information available in the outpatient EHR. More data from external sources could potentially help refine cohort measurement, making it even more precise. Given appropriate data, for example, variables could be included to capture social, behavioral, and adherence factors that have been shown to have a significant impact on health outcomes58,59.
The method is sensitive to the size of the precision cohort. Our data set contained approximately 2.5 million patients from one health system. Although the size of our patient pool was sufficient to provide statistically significant treatment options for the common diseases we studied, less common diseases may not allow us to identify statistically meaningful precision cohorts. Combining data from multiple health systems would increase the numbers but may introduce other confounders that influence the similarity of patients. Applying our methods to data from other health systems would help assess the generalizability of our approach. Another approach is to make more efficient use of the available data by using all of the DPs, by weighting their contribution based on the similarity score, instead of thresholding and using only a small subset.
There are additional limitations to the use of observational data. In addition to missingness, incompleteness, and errors, there is increasing attention to the inadvertent presence of bias in training data60. Even with the causal inference mitigation methods described in “Precision cohort identification”, the selection of confounder covariates may not be fully complete, and biases may not be eliminated entirely. In this work, we used observational data from EHRs, which has rich clinical information (such as lab test results) that was important for our use case of being able to assess chronic disease control. Other types of observational healthcare data, such as claims, have not been found to be as reliable61. However, claims data can be leveraged for different use cases, where less detailed information is required, e.g., if the outcomes can be characterized using only billing codes62.
Finally, this work used data from a single healthcare system, and the DPs were extracted from historical data, which may contain outdated treatment information and historical biases63. We attempted to mitigate the impact of this by adjusting the lookback period to coincide with the publication date of the most recent national guidelines and only considering drugs approved by current guidelines. However, prospective evaluation and independent validation of the PCTO workflow on data from different healthcare systems are needed to establish and verify its clinical utility and effectiveness on patient health outcomes.
In addition to addressing these limitations in future work, there are other possible extensions. One is to leverage the method to perform retrospective population-based analysis that could be useful to both healthcare providers and payers. The current approach to population health management relies on creating reports of patients whose disease was not under control when the report was generated. From a patient-risk perspective, this time-slice view does not adequately reflect the cumulative morbidity risks of patients’ uncontrolled state over time. From a provider perspective, the periodic reports do not portray the opportunities the health professional had to make changes to the interventions to improve the control of the chronic condition. One possible approach to address these issues is to apply the PCTO workflow to historical patient data, compare the resulting personalized treatment options and outcomes against the actual treatment options and outcomes, analyze the data to identify potential care gaps and missed treatment decision opportunities, and then aggregate the results across the DPs to generate population-level insights. We recently performed this “precision population analysis” and found that, for the majority of DPs, there were alternative treatment options administered to patients in the precision cohort that resulted in a significantly increased proportion of patients under control than the actual treatment option chosen for the index patient64.
In summary, we presented a novel approach to analyzing observational data from a large number of patients to derive best practices that achieve better clinical outcomes for similar patients. The workflow was successfully implemented using EHR data from a large health care provider for three different chronic diseases (HTN, T2DM, and HL). A retrospective analysis demonstrated that alternative treatment options with better outcomes were available for a majority of cases. The resultant models for HTN and T2DM were deployed in a pilot study with PCPs who used it during clinic visits. Presenting AI-derived insight from analysis of population data in the EHR can complement recommendations from clinical guidelines and personal experience, to help physicians personalize treatment decisions for individual patients.
Data availability
The data that support the findings of this study are available from Atrius Health, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Atrius Health.
Abbreviations
- ACEI:
-
Angiotensin converting enzyme inhibitor
- ACC:
-
American college of cardiology
- ADA:
-
American diabetes association
- AHA:
-
American heart association
- CCB:
-
Calcium channel blocker
- CCS:
-
Clinical classifications software
- CDS:
-
Clinical decision support
- CKD:
-
Chronic kidney disease
- EHR:
-
Electronic health record
- GB:
-
Green Button
- HL:
-
Hyperlipidemia
- HTN:
-
Hypertension
- ICD:
-
International classification of diseases
- JNC:
-
Joint national committee
- LOOCV:
-
Leave-one-out cross-validation
- LSML:
-
Locally supervised metric learning
- PCP:
-
Primary care physician
- PCTO:
-
Precision cohort treatment options
- RCT:
-
Randomized clinical trial
- RxCUI:
-
RxNorm concept unique identifier
- SDOH:
-
Social determinants of health
- T2DM:
-
Type 2 diabetes mellitus
References
Health Policy Data Requests: Percent of U.S. Adults 55 and Over with Chronic Conditions. https://www.cdc.gov/nchs/health_policy/adult_chronic_conditions.htm (2019).
Fischer, F., Lange, K., Klose, K., Greiner, W. & Kraemer, A. Barriers and strategies in guideline implementation: A scoping review. Healthcare 4, 36 (2016).
Stewart, W. F., Shah, N. R., Selna, M. J., Paulus, R. A. & Walker, J. M. Bridging the inferential gap: The electronic health record and clinical evidence. Health Aff. Proj. Hope 26, w181-191 (2007).
Van Spall, H. G. C., Toren, A., Kiss, A. & Fowler, R. A. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: A systematic sampling review. JAMA 297, 1233–1240 (2007).
Raffoul, M., Moore, M., Kamerow, D. & Bazemore, A. A primary care panel size of 2500 is neither accurate nor reasonable. J. Am. Board Fam. Med. JABFM 29, 496–499 (2016).
Ronquillo, J. G. How the electronic health record will change the future of health care. Yale J. Biol. Med. 85, 379–386 (2012).
Office-based Physician Electronic Health Record Adoption, Health IT Quick-Stat #50. https://dashboard.healthit.gov/quickstats/pages/physician-ehr-adoption-trends.php.
Longhurst, C. A., Harrington, R. A. & Shah, N. H. A ‘green button’ for using aggregate patient data at the point of care. Health Aff. Proj. Hope 33, 1229–1235 (2014).
Black, N. Why we need observational studies to evaluate the effectiveness of health care. BMJ 312, 1215–1218 (1996).
Sharafoddini, A., Dubin, J. A. & Lee, J. Patient similarity in prediction models based on health data: A scoping review. JMIR Med. Inform. 5, e7 (2017).
Parimbelli, E., Marini, S., Sacchi, L. & Bellazzi, R. Patient similarity for precision medicine: A systematic review. J. Biomed. Inform. 83, 87–96 (2018).
Wang, F., Sun, J., Li, T. & Anerousis, N. Two Heads Better Than One: Metric+Active Learning and its Applications for IT Service Classification. in Ninth IEEE International Conference on Data Mining, 2009. ICDM ’09 1022–1027 (2009). https://doi.org/10.1109/ICDM.2009.103.
Gottlieb, A., Stein, G. Y., Ruppin, E., Altman, R. B. & Sharan, R. A method for inferring medical diagnoses from patient similarities. BMC Med. 11, 1 (2013).
Qian, B., Wang, X., Cao, N., Li, H. & Jiang, Y.-G. A relative similarity based method for interactive patient risk prediction. Data Min. Knowl. Discov. 29, 1070–1093 (2015).
Wang, B. et al. Similarity network fusion for aggregating data types on a genomic scale. Nat. Methods 11, 333–337 (2014).
Dowding, D. W., Turley, M. & Garrido, T. The impact of an electronic health record on nurse sensitive patient outcomes: An interrupted time series analysis. J. Am. Med. Inform. Assoc. 19, 615–620 (2012).
Rathlev, N. et al. Time series analysis of emergency department length of stay per 8-hour shift. West. J. Emerg. Med. 13, 163–168 (2012).
Durichen, R., Pimentel, M. A. F., Clifton, L., Schweikard, A. & Clifton, D. A. Multitask Gaussian processes for multivariate physiological time-series analysis. IEEE Trans. Biomed. Eng. 62, 314–322 (2015).
Fabbri, D. & LeFevre, K. Explaining accesses to electronic medical records using diagnosis information. J. Am. Med. Inform. Assoc. 20, 52–60 (2013).
Shah, S. J. et al. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation 131, 269–279 (2015).
Wang, F., Hu, J. & Sun, J. Medical prognosis based on patient similarity and expert feedback. in Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012) 1799–1802 (2012).
Wang, F. & Sun, J. PSF: A unified patient similarity evaluation framework through metric learning with weak supervision. IEEE J. Biomed. Health Inform. 19, 1053–1060 (2015).
Zhang, P., Wang, F., Hu, J. & Sorrentino, R. Towards personalized medicine: Leveraging patient similarity and drug similarity analytics. AMIA Jt. Summits Transl. Sci. 2014, 132–136 (2014).
Li, L. et al. Identification of type 2 diabetes subgroups through topological analysis of patient similarity. Sci. Transl. Med. 7, 311174 (2015).
Ng, K., Sun, J., Hu, J. & Wang, F. Personalized predictive modeling and risk factor identification using patient similarity. AMIA Jt. Summits Transl. Sci. 2015, 132–136 (2015).
Woldaregay, A. Z. et al. Data-driven modeling and prediction of blood glucose dynamics: Machine learning applications in type 1 diabetes. Artif. Intell. Med. 98, 109–134 (2019).
Battineni, G., Sagaro, G. G., Chinatalapudi, N. & Amenta, F. Applications of machine learning predictive models in the chronic disease diagnosis. J. Pers. Med. 10, 21 (2020).
Becker, M. & Böckmann, B. Personalized guideline-based treatment recommendations using natural language processing techniques. Stud. Health Technol. Inform. 235, 271–275 (2017).
Lancaster, J. & Nevins, J. Individualized Cancer Treatments (Springer, New York, 2007).
Pecora, A. L. Clinical Outcome Tracking and Analysis (Springer, New York, 2017).
Monier, L., Zimmerman, N. & Percha, B. System for Generating and Updating Treatment Guidelines and Estimating Effect Size of Treatment Steps (Springer, New York, 2016).
Gallego, B. et al. Bringing cohort studies to the bedside: Framework for a ‘green button’ to support clinical decision-making. J. Comp. Eff. Res. 4, 191–197 (2015).
Schuler, A., Callahan, A., Jung, K. & Shah, N. H. Performing an informatics consult: Methods and challenges. J. Am. Coll. Radiol. JACR 15, 563–568 (2018).
Gombar, S., Callahan, A., Califf, R., Harrington, R. & Shah, N. H. It is time to learn from patients like mine. NPJ Digit. Med. 2, 16 (2019).
Pedregosa, F. et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 12, 2825–2830 (2011).
R Development Core Team. R: A Language and Environment for Statistical Computing. (R Foundation for Statistical Computing, Vienna, 2008).
Liu, S., Ma, W., Moore, R., Ganesan, V. & Nelson, S. RxNorm: Prescription for electronic drug information exchange. IT Prof. 7, 17–23 (2005).
LOINC Table, Reports, and Users’ Guide. LOINC https://loinc.org/downloads/loinc-table/.
HCUP-US Tools & Software Page. https://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp.
ICD: ICD-9-CM: International Classification of Diseases, Ninth Revision, Clinical Modification. https://www.cdc.gov/nchs/icd/icd9cm.htm (2019).
ICD: ICD-10-CM: International Classification of Diseases, Tenth Revision, Clinical Modification. https://www.cdc.gov/nchs/icd/icd10cm.htm (2019).
Meinshausen, N. Stability selection. J. R. Stat. Soc. B https://doi.org/10.1111/j.1467-9868.2010.00740.x (2010).
Ng, A. Y. Feature selection, l1 vs. l2 regularization, and rotational invariance. ICML (2004).
Rubin, D. B. Estimating causal effects of treatments in randomized and nonrandomized studies. J. Educ. Psychol. https://doi.org/10.1037/h0037350 (1974).
Hernan, M. A. & Robins, J. M. Causal Inference: What If (Chapman & Hall/CRC, Boca Raton, 2020).
Causal Inference without Balance Checking: Coarsened Exact Matching|Political Analysis|Cambridge Core. https://www.cambridge.org/core/journals/political-analysis/article/causal-inference-without-balance-checking-coarsened-exact-matching/5ABCF5B3FC3089A87FD59CECBB3465C0.
Stuart, E. A. Matching methods for causal inference: A review and a look forward. Stat. Sci. Rev. J. Inst. Math. Stat. 25, 1–21 (2010).
Sauppe, J. J. & Jacobson, S. H. The role of covariate balance in observational studies. Nav. Res. Logist. NRL 64, 323–344 (2017).
Bland, J. M. & Altman, D. G. Multiple significance tests: the Bonferroni method. BMJ 310, 170 (1995).
Sankey Diagram|Charts. Google Developers https://developers.google.com/chart/interactive/docs/gallery/sankey.
Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. in Proceedings of the 14th international joint conference on Artificial intelligence - Volume 2 1137–1143 (Morgan Kaufmann Publishers Inc., 1995).
Hripcsak, G. et al. Characterizing treatment pathways at scale using the OHDSI network. Proc. Natl. Acad. Sci. USA. 113, 7329–7336 (2016).
Grundy Scott, M. et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 139, e1082–e1143 (2019).
Lackland, D. T. Racial differences in hypertension: Implications for high blood pressure management. Am. J. Med. Sci. 348, 135–138 (2014).
Grossman, A. & Grossman, E. Blood pressure control in type 2 diabetic patients. Cardiovasc. Diabetol. 16, 3 (2017).
McKenney, J. M. et al. Comparison of the efficacy of rosuvastatin versus atorvastatin, simvastatin, and pravastatin in achieving lipid goals: Results from the STELLAR trial. Curr. Med. Res. Opin. 19, 689–698 (2003).
Zhang, F. et al. Increasing use of prescription drugs in the United Kingdom. Pharmacoepidemiol. Drug Saf. 25, 628 (2016).
Walker, R. J., StromWilliams, J. & Egede, L. E. Influence of race, ethnicity and social determinants of health on diabetes outcomes. Am. J. Med. Sci. 351, 366–373 (2016).
Beck, A. F. et al. Perspectives from the Society for Pediatric Research: Interventions targeting social needs in pediatric clinical care. Pediatr. Res. 84, 10–21 (2018).
Obermeyer, Z., Powers, B., Vogeli, C. & Mullainathan, S. Dissecting racial bias in an algorithm used to manage the health of populations. Science 366, 447–453 (2019).
Tang, P. C., Ralston, M., Arrigotti, M. F., Qureshi, L. & Graham, J. Comparison of methodologies for calculating quality measures based on administrative data versus clinical data from an electronic health record system: Implications for performance measures. J. Am. Med. Inform. Assoc. JAMIA 14, 10–15 (2007).
Wirbka, L., Haefeli, W. E. & Meid, A. D. A framework to build similarity-based cohorts for personalized treatment advice: A standardized, but flexible workflow with the R package SimBaCo. PLoS ONE 15, e0233686 (2020).
T. W. H. Big Data: A Report on Algorithmic Systems, Opportunity, and Civil Rights. https://www.whitehouse.gov (2016).
Tang, P. C. et al. Precision population analytics: Population management at the point-of-care. J. Am. Med. Inform. Assoc. JAMIA https://doi.org/10.1093/jamia/ocaa247 (2020).
James, P. A. et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 311, 507–520 (2014).
Association, A. D. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes—2018. Diabetes Care 41, S73–S85 (2018).
Acknowledgements
This project was supported in part by IBM Research and Watson Health. The authors would like to thank the clinician users of the pilot system at Atrius Health, who provided excellent feedback on the system, and the Atrius Health information systems team, who implemented the system in their EHR. We thank the IBM Watson Health offering management team and software developers for developing the software used in production at Atrius Health.
Author information
Authors and Affiliations
Contributions
P.T., K.N., and U.K. contributed to the creation and formulation of the methods. K.N., U.K., and H.S. implemented the methods and performed the data analysis. K.N., P.T., and U.K. wrote the manuscript. P.T. and J.Z. supervised the study and provided clinical guidance and feedback. J.Z. facilitated access to the data. All authors reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
K.N., U.K., and H.S. are employees of IBM. P.T. is currently affiliated with Stanford University but was an employee of IBM during the time the research was conducted. J.Z. is an employee of Atrius Health.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ng, K., Kartoun, U., Stavropoulos, H. et al. Personalized treatment options for chronic diseases using precision cohort analytics. Sci Rep 11, 1139 (2021). https://doi.org/10.1038/s41598-021-80967-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-80967-5
This article is cited by
-
Diabetes medication recommendation system using patient similarity analytics
Scientific Reports (2022)
-
Enhancing Clinical Prediction Performance by Incorporating Intuition
Journal of Medical Systems (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
