
Abstract
Obesity and relative leucocyte telomere length (RTL) are both linked to accelerated aging and premature mortality. We examined if nuchal subcutaneous adipose tissue (SAT) thickness, a surrogate marker of central trunk-weighted obesity, is an independent predictor of RTL that provides information beyond BMI, metabolic and inflammatory markers. RTL and nuchal SAT thickness were determined in 362 participants of the STYJOBS/EDECTA study (STYrian Juvenile Obesity Study, Early DEteCTion of atherosclerosis), which included overweight individuals and matched eutrophic controls. Fasting plasma samples were used for the measurement of leptin, resistin, adiponectin, glucose, insulin, high-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), liver enzymes, creatinine, cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, oxidized LDL, triglycerides, homocysteine and uric acid. Furthermore, all participants underwent carotid artery ultrasound. Obese individuals had markedly higher body mass index (BMI), nuchal SAT thickness, hip and waist circumferences and carotid intima media thickness (IMT) than eutrophic controls. In addition, they showed typical biochemical abnormalities related to energy metabolism, systemic inflammation and liver function. RTL was inversely correlated with nuchal SAT thickness, IMT, hs-CRP, alkaline phosphatase, insulin, resistin, and leptin. Positive correlations were seen with homocysteine and creatinine. Stepwise linear regression analyses identified nuchal SAT thickness and insulin as the only significant predictors of RTL. In conclusion, nuchal SAT thickness is a robust predictor of RTL that provides information beyond traditional obesity-related metabolic and inflammatory biomarkers. This suggests an important role of fat depots at the neck for accelerated telomere shortening.
Similar content being viewed by others


Introduction
Telomeres are protective nucleoprotein structures at the end of all chromosomes that shorten with age. When telomeres become critically short, they induce apoptosis. Telomere length in circulating leucocytes is considered a surrogate marker of genomic aging in the entire body. In previous longitudinal studies, telomere length has firmly been established as a predictor of mortality risk. For example, in the Ludwigshafen Risk and Cardiovascular Health (LURIC) study, cardiovascular patients with the lowest relative leucocyte telomere length (RTL) had an 18% higher risk of mortality during an average follow-up period of 9.9 years when compared to all other participants1. Mons et al. analyzed 12,199 individuals from two population-based prospective cohort studies with an age range of 43–75 years. Participants in the first RTL quartile with the shortest telomeres had a 23% higher risk of dying from any cause than those in the fifth quintile with the longest telomeres2.
Solid knowledge about the factors that influence RTL is important for a potential clinical use of this promising marker and an appropriate interpretation of results. Lifestyle factors, such as physical activity, nutrition and stress have been suggested as potential modulators of telomere length3,4,5,6,7,8,9,10,11. For example, regular endurance exercise induces telomerase, an enzyme that can prolong telomeres, and thus prevent telomere shortening4,5,6,7. Nutritional factors also appear to be involved in telomere biology. Pusceddu et al. have shown that vitamin B6, B12 and homocysteine relate to RTL and mortality in cardiovascular patients11. In contrast, in longitudinal studies various diets or food supplements, considered generally healthy have shown little or no effect on telomere attrition8,9.
Obesity is a very common condition in Western societies that is associated with a broad range of metabolic alterations, elevated oxidative stress and chronic low-grade inflammation10,12. According to current concepts adipose tissue promotes the process of aging and drives the development of chronic diseases, such as type 2 diabetes (T2DM), non-alcoholic fatty liver disease (NAFLD), cancer, and cardiovascular diseases12. Based on the aforementioned observations it has been hypothesized that obesity accelerates telomere shortening. However, studies of leucocyte RTL in obese phenotypes yielded conflicting results, and the association between body mass index (BMI) and RTL during life time is still unclear13,14,15. A recent meta-analysis showed a converse relationship between BMI and RTL in cross sectional studies16. However, the authors of this meta-analysis claimed a lack of longitudinal studies with comprehensive controlling for age- and sex-specific confounders. Irrespective of an increased BMI, the location of fat accumulation appears to matter. In the past, three body types have been assigned based upon the distribution of body fat: android (apple shape), intermediate, and gynoid (pear shape). The apple shape has repeatedly been associated with an increased risk of diabetes, hypertension and hypercholesterolemia17,18.
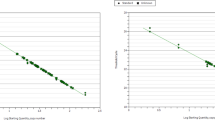
Considering that the classification of body shape is rather subjective, alternative approaches, like waist-to-hip ratio (WHR) or weight-shape-index (WSI) have been explored. The analysis of subcutaneous adipose tissue (SAT) thickness at standardized anatomical points across the whole body using a recently developed optical lipometric device is a more objective and precise way to assess adiposity and fat distribution patterns19. Using this method, we have recently shown that RTL has a robust negative correlation with nuchal SAT thickness20. However, other circulating biomarkers that are commonly altered in obese subjects were not considered.
This raised the question if nuchal SAT remains an independent predictor of RTL when other metabolic and inflammatory biomarkers are included in a multivariate analysis. This gap of knowledge prompted us to analyze a broad range of additional obesity-related biomarkers and explore if nuchal SAT remains an independent predictor of RTL that provides information beyond these traditional biochemical analyses.
Materials and Methods
Study population
For the purpose of this study, we analyzed RTL and SAT distribution in all 362 participants of the STYJOBS/EDECTA study (STYrian Juvenile Obesity Study, Early DEteCTion of atherosclerosis) from whom DNA samples were available. The STYJOBS/EDECTA study cohort consists primarily of overweight/obese individuals and sex and age matched normal weight controls aged between 7–68 years. Participants were recruited between 2005–2014 through campaigning on local media, at our outpatient patient clinic at the Medical University Graz (Austria), at collaborating medical practitioners and in local schools. Overweight was defined as having a BMI > 90th and <97th percentile in underage individuals (≤18 years), and between>25 and <29.9 kg/m2 in adults (>18 years). Underage participants with a BMI > 97th percentile and adults with>30 kg/m2 were classified as obese. All participants underwent physical examination, fasting blood collection, carotid ultrasound and standardized lipometry. Moreover, height, weight, waist and hip circumference were assessed. Exclusion criteria were endocrine diseases (e.g. hypothyreosis, manifest type 2 diabetes), infectious, inflammatory or any other chronic diseases. Detailed information of STYJOBS is available at ClinicalTrials.gov (Identifier NCT00482924).
Lipometry
SAT thickness was assessed at 15 anatomically well-defined body sites distributed from neck to calf on the left side of all participants. Lipometry was performed using an optical device (EU Patent No. 0516251). The sensor head of the lipometer, that is held perpendicular to the measurement site, consists of a set of light emitting diodes (λ = 660 nm, light intensity 3.000 mcd) and a photodetector, that measures the corresponding light intensities that are back scattered in the SAT. Calibration and evaluation were done using computed tomography (CT) as the reference method21,22,23.
Analysis of telomere length
Genomic DNA was prepared from stored EDTA whole blood using a MagNA Pure instrument (Roche, Vienna, Austria). Purity and concentration of the extracted DNA were measured by UV photometry at 260 nm and 280 nm, respectively. DNA samples were diluted to a concentration of 10 ng/µl. RTL was measured by a qPCR assay developed by Cawthon24 with minor modifications. The assay quantified the ratio of average telomere length to a single-gene copy (RPLP0, previously denoted as “36B4”). All qPCR analyses were performed as triplicates in 96-well plates on a CFX96 Real-Time PCR Detection System (Bio-Rad Laboratories, Vienna, Austria). Total reaction volume was 25 µl. For the quantification of the single copy gene, forward primer 5′-CAGCAAGTGGGAAGGTGTAATCC-3′ and reverse primer 5′- CCCATTCTATCATCAACGGGTACAA-3′ were used. For the quantification of telomeres, forward primer 5′-CGGTTTGTTTGGGTTTGGGTTTGGGTTTGGGTTTGGGTT-3′ and reverse primer 5′-GGCTTGCCTTACCCTTACCCTTACCCTTACCCTTACCCT-3′ were used. Primers were purchased at Metabion GmbH (Martinsried, Germany). Each reaction contained 300 nmol/L forward primer, 300 nmol/L reverse primer, 40 ng DNA, 1x SYBR Green I Stain (Lonza Cologne GmbH, Cologne, Germany) and 2.5 µl PerfeCTa qPCR 10x SuperMix (Quanta, Beverly, USA). Thermal cycling profile was 10 min at 95 °C followed by 40 cycles of 15 s at 95 °C, 30 s at 54 °C and 30 s at 72 °C with fluorescence data collection. Each run included a standard curve made by dilutions of available HeLa-DNA (New England Biolabs, Frankfurt, Germany) to determine the quantity of targeted templates in each sample relative to the HeLa-DNA. RTL was calculated as the ratio of telomere quantity to single copy gene quantity. PCR efficiencies were 106% for telomere amplification and 94% for single copy gene amplification. Mean intra-assay coefficient of variability (CV) was 8.7% and plate-to-plate CV was 12.7%.
Laboratory analysis
During the initial study visit, fasting blood samples were collected from all patients, and stored at −20 °C until analysis. Leptin, resistin and adiponectin were determined from human plasma by ELISAs from Biovendor Laboratory Medicine, Inc. (Brno, Czech Republic), oxidized low-density lipoprotein (LDL), and plasma insulin by commercially available ELISAs from Mercodia (Uppsala, Sweden). Intra- and inter-assay coefficients of variation for all ELISAs in our study were below 10%. HOMA-IR (homeostatic model assessment – insulin resistance) was calculated as the product of the fasting plasma insulin value (in micro units per ml) and the fasting plasma glucose value (in mmol/L), divided by 22.525. High-sensitivity C-reactive protein, IL-6, liver transaminases [aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (gamma-GT)], alkaline phosphatase (ALP), creatinine, alkaline phosphatase, glucose, cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, homocysteine (HCY) and uric acid were measured by commercial routine laboratory methods from Roche Diagnostics on a Cobas 8000 chemical analyzer (Roche Diagnostics Mannheim, Germany).
Carotid artery ultrasound
The ultrasound protocol involved scanning of the bulbous near common carotid artery26 on both sides with a 12-to-5-MHz broad-band linear transducer on a HDI 5000 (ATL, Bothell, Washington, DC, USA). The same investigator performed all scans to identify the greatest wall thickness. Longitudinal images directed through the center of the artery were analyzed at each vessel site. Measurements were made from stored digital images by an experienced reader. The IMT was assessed at the far wall as the distance between the interface of the lumen and intimae, and the interface between the media and adventitia26,27,28. The maximal IMT was recorded at each of the vessel segments and averaged for the left and right sides. The lumen diameter was calculated as the inter-adventitial diameter minus twice the maximum far wall IMT. All diameters were measured during diastole to avoid image blurring due to systolic arterial wall motion, and to minimize the influence of blood pressure28.
Ethics
STYJOBS/EDECTA was approved by the ethical committee of the Medical University of Graz (EK number 20–029 ex 08/09), and conducted in compliance with guidelines for human studies as described in the Helsinki Declaration of 1975, revised in 1996. Blood collection occurred after written informed consent by the participants. If the volunteers were under the age of 18 years, informed consent has been obtained from a parent and/or legal guardian.
Statistics
All variables were checked for normal distribution using the Kolmogorov-Smirnov test. Mean and standard deviation (SD) were calculated for all normally distributed variables, whereas median and interquartile ranges (IQR) were determined for not normally distributed variables. Relationships between RTL and various indices of body composure were identified by Pearson correlation analyses. P-values < 0.05 were considered significant. In order to identify the strongest determinants of RTL we entered all variables that correlated significantly with RTL into a stepwise linear regression analysis. All statistical analyses were conducted using the PASW Statistics 24.0 package.
Results
The 362 participants had a mean age of 34.2 + 14.0 (SD) years (range: 7.2–68years), a mean height of 170 + 10.6 (SD) cm (range: 126–197 cm) and a mean weight of 79.4 + 23.7 (SD) kg (range: 24–180 kg). Table 1 summarizes anthropometric, clinical and biochemical characteristics of all participants. BMI, hip and waist circumference as well as nuchal SAT thickness were markedly higher in obese individuals than in eutrophic controls. Obese participants also showed numerous biochemical abnormalities related to energy metabolism, systemic inflammation and liver function (Table 2).
In the Pearson correlation analysis RTL was inversely correlated with nuchal SAT thickness, carotid IMT, hs-CRP, ALP, insulin, HOMA-IR, resistin, and leptin (Table 3). Positive correlations were seen with HCY and creatinine. The strongest correlation was found between RTL and leptin followed by nuchal SAT thickness.
Subsequently a stepwise linear regression analyses with RTL as the dependent variable was performed. As independent variables, we included sex, age and all biochemical analytes that were significantly correlated with RTL in the previous Pearson correlation analysis. This analysis identified nuchal fat thickness and insulin as the only significant predictors of RTL in the final model (Table 4).
Discussion
In this study we provide evidence for a link between centralized SAT accumulation, disturbed glucose metabolism and genomic ageing. Nuchal SAT thickness appears to be a robust predictor of RTL that provides additional information beyond traditional obesity-related metabolic and inflammatory biomarkers. Fat depots at the neck and upper trunk seem to be particularly critical for accelerated shortening of telomeres. According to our observation, recent prospective studies showed that cardiovascular patients with an increased neck circumference have higher cardiovascular and all-cause mortality compared to those with a normal or low-neck circumference29. Our results further imply that a substantial part of the risk related to obesity is not captured by the measurement of traditional biomarkers, such as lipids, inflammatory markers or adipokines.
The link between nuchal SAT accumulation, plasma insulin levels and RTL relates a specific SAT distribution pattern to an altered glucose metabolism and accelerated genomic aging, indicated by short RTL. An association between obesity and telomere physiology has been reported before13,30,31,32,33,34,35,36. However, most previous studies used BMI to characterize individuals as overweight/obese or normal weight. A recently published meta-analysis of 87 observational studies including data from 146.114 subjects showed a significant inverse relationship between BMI and leucocyte telomere length, especially in young persons37. Mean telomere length decreased by 3.99 base pairs per unit increase in BMI37. However, on an individual basis the majority of the studies included show a trend, but failed to reach significance. Indirect evidence for an adverse effect of obesity on genomic aging comes from the observation that sustained weight loss 3–5 years after a gastric bypass operation is associated with an increase in RTL38. Even in childhood, obesity appears to link to short telomeres39. Otherwise, two recent studies challenged the clinical usefulness of RTL analysis in diabetes risk stratification. The first study investigated participants from the multiethnic Women’s Health Initiative and reported only limited clinical usability of RTL for diabetes risk stratification among postmenopausal women40. The second study analyzed RTL and glucose tolerance status in 205 mixed-ancestry South Africans and found no association of RTL with glycaemia41.
Body shape and fat distribution are important determinants of the health risks related to obesity (20,21). However, SAT distribution has not been considered systematically in previous investigations, especially in young people data are scarce. The strength of our study is the investigation of not only metabolic but also inflammatory parameters and RTL. Furthermore, an extensive noninvasive evaluation of the subcutaneous body fat distribution was performed, including young participants. According to current concepts, SAT is considered the least harmful adipose depot42. Nevertheless, when the SAT adipose cells become expanded (hypertrophic obesity), SAT become dysfunctional and drive the deposition of fat in ectopic depots, such as the liver and visceral organs. Increased hepatic and visceral fat reflects the inability of SAT to accommodate excess fat and lead to paracrine and endocrine effects that promote metabolic dysfunction42. The accumulation of visceral and nuchal fat depots often coincides in obese subjects and may represent an ‘overflow phenomenon’ where the storage capacity of SAT is exceeded so that fat has to be stored in ectopic depots42. If this process starts in the young and remains over time, the perdurability of “overflow” may create a more dangerous impact for serious obesity related clinical sequels. Risk algorithms including nuchal SAT thickness are missing because a simple method for the assessment of SAT distribution was not available in the past. The 15-point lipometry used here is a simple manageable tool that facilitates the assessment of SAT distribution. With the help of this method we have been able to identify “healthy obese” and “unhealthy lean” phenotypes in the STYJOBS cohort43. Moreover, we could show that nuchal SAT thickness is most predictive for other obesity-related biomarkers44.
Typically, obesity is accompanied by a broad range of metabolic alterations, elevated oxidative stress and chronic low-grade inflammation12,45,46,47,48,49,50,51. In previous studies, numerous blood biomarkers that address these pathomechanistic aspects have been linked to RTL. For example, significant associations with RTL have been reported for hs-CRP52, adiponectin53, and leptin54. Inflammation and oxidative stress of obesity are a pre-disease mechanisms for chronic diseases of ageing like cardiovascular disease, and cancer. The inflammatory cytokines TNF-α, IL-6 and IFN-γ may promote RTL shortening but direct influence lacks evidence and mechanisms remain ultimately unknown55. Interestingly, in the multivariate stepwise regression analysis of the present study insulin and nuchal SAT thickness but not hs-CRP or IL-6 were the only significant predictors of RTL. This argues for a strong influence of a disturbed glucose metabolism and central fat accumulation on RTL length. Previous case-control studies in patients with T2DM56,57,58 support this observation. A recent meta-analysis of 17 studies including 5575 diabetic patients and 6389 controls confirmed shorter RTL in T2DM patients in different geographic regions58. In type 1 diabetes (T1DM) this difference is much less pronounced, which highlights the potential role of insulin for telomere function. Circulating insulin is chronically elevated in T2DM until exhaustion of ß-cells in the later stages of the disease59. A recent 6-year prospective study of 67 T2DM patients revealed insulin use as a strong and significant predictor of accelerated telomere attrition in these patients. In a recent study of 44,168 individuals, investigating a new risk profile for all-cause mortality increased blood glucose levels had a strong influence to all-cause mortality60. The concept of insulin excess as a promotor of accelerated aging is also supported by a study in Asian Indians where Satishkumar et al. found an association between, insulin resistance, inflammation and cellular senescence61. These results have led to the hypothesis that RTL might be a biomarker of cellular senescence and predict CVD62. Supporting this hypothesis, Strazhesko I et al. showed that decreased RTL independently associates positively with atherosclerotic changes of the arterial wall, such as plaques number62. Primarily in 2010, Preis et al.63 showed in the Framingham Heart Study that increased neck circumference indicates a high risk for cardiovascular diseases. Recently, Caro et al.64 and Koppad et al.65 confirmed these observations. Our herein observed association between nuchal fat accumulations, decreased RTL and increased insulin levels may indicate the beginning of a pathological process leading to cardiovascular disease later in life. Several mechanism(s) linking RTL, insulin, and nuchal fat accumulation have been discussed. For example, hypo-methylation of the subtelomeric region has been proposed as a potential promotor of accelerated telomere shortening in T2DM66. However, this concept is not supported by another study of 418 Chinese T2DM patients where shorter leucocyte telomere length associated with LINE-1 hyper-methylation56.
Alternatively, high insulin levels may have direct damaging effects on telomeres and shelterin proteins. For example, Ras-proximate-1 or Ras-related protein 1(RAP1), a part of the shelterin complex, is a major regulator of energy metabolism67. In mice, inhibition of RAP 1 affects hepatic and adipose cell functions, resulting in disturbed glucose metabolism, insulin resistance, and obesity68. However, human studies exploring the link between obesity, insulin, RAP1 and RTL are lacking.
This study has limitations as follows. The lack of serial blood collections over a longer period prevents an evaluation of telomere dynamics in normal and overweight subjects. Furthermore, including low-weight subjects might have given important additional information. However, so far we were not able to recruit a relevant number of underweight/anorectic individuals. Another limitation is the method used for analysis of RTL. This qPCR method determines an average RTL value across chromosomes and cells, without considering differences between single chromosomes and cells. Moreover, we did not analyze glycemic statuses of participants, and individuals with an increased insulin concentration and participants with an abnormal HOMA index did not undergo an oral glucose tolerance test in order to prove insulin resistance. Finally yet importantly, the lipometry method used here describes SAT distribution but ignores visceral fat depots. Dual x-ray absorptiometry that can provide valuable information on body composition was unavailable for this study.
In conclusion, the relationship between nuchal SAT thickness, insulin and RTL observed in the present study suggests that central obesity and decreased insulin sensitivity are a fatal combination. Longitudinal studies are needed to explore the kinetics of RTL and glucose metabolism in normal and overweight subjects over time. These studies should keep track of future cardiovascular diseases and individual life expectancy.
References
Pusceddu, I. et al. Telomere length and mortality in the Ludwigshafen Risk and Cardiovascular Health study. PloS one 13, e0198373, https://doi.org/10.1371/journal.pone.0198373 (2018).
Mons, U. et al. Leukocyte Telomere Length and All-Cause, Cardiovascular Disease, and Cancer Mortality: Results From Individual-Participant-Data Meta-Analysis of 2 Large Prospective Cohort Studies. Am J Epidemiol 185, 1317–1326, https://doi.org/10.1093/aje/kww210 (2017).
Herrmann, M., Pusceddu, I., Marz, W. & Herrmann, W. Telomere biology and age-related diseases. Clinical chemistry and laboratory medicine 56, 1210–1222, https://doi.org/10.1515/cclm-2017-0870 (2018).
Werner, C. et al. Physical exercise prevents cellular senescence in circulating leukocytes and in the vessel wall. Circulation 120, 2438–2447, https://doi.org/10.1161/CIRCULATIONAHA.109.861005 (2009).
Werner, C. M. et al. Differential effects of endurance, interval, and resistance training on telomerase activity and telomere length in a randomized, controlled study. Eur Heart J 40, 34–46, https://doi.org/10.1093/eurheartj/ehy585 (2019).
Ludlow, A. T. et al. Chronic exercise modifies age-related telomere dynamics in a tissue-specific fashion. J Gerontol A Biol Sci Med Sci 67, 911–926, https://doi.org/10.1093/gerona/gls002 (2012).
Ludlow, A. T. et al. Relationship between physical activity level, telomere length, and telomerase activity. Medicine and science in sports and exercise 40, 1764–1771, https://doi.org/10.1249/MSS.0b013e31817c92aa (2008).
Perez, L. M. et al. Effects of Diet on Telomere Length: Systematic Review and Meta-Analysis. Public Health Genomics 20, 286–292, https://doi.org/10.1159/000486586 (2017).
Meinila, J. et al. Healthy diets and telomere length and attrition during a 10-year follow-up. European journal of clinical nutrition, https://doi.org/10.1038/s41430-018-0387-4 (2019).
Maffetone, P. B., Rivera-Dominguez, I., Laursen, P. B. & Overfat and Underfat: New Terms and Definitions Long Overdue. Frontiers in public health 4, 279, https://doi.org/10.3389/fpubh.2016.00279 (2016).
Pusceddu, I. et al. Subclinical inflammation, telomere shortening, homocysteine, vitamin B6, and mortality: the Ludwigshafen Risk and Cardiovascular Health Study. Eur J Nutr, https://doi.org/10.1007/s00394-019-01993-8 (2019).
Mangge, H. et al. Inflammation, adiponectin, obesity and cardiovascular risk. Current medicinal chemistry 17, 4511–4520 (2010).
Wulaningsih, W., Kuh, D., Wong, A. & Hardy, R. Adiposity, Telomere Length, and Telomere Attrition in Midlife: the 1946 British Birth Cohort. J Gerontol A Biol Sci Med Sci 73, 966–972, https://doi.org/10.1093/gerona/glx151 (2018).
Buxton, J. L. et al. Multiple measures of adiposity are associated with mean leukocyte telomere length in the northern Finland birth cohort 1966. PloS one 9, e99133, https://doi.org/10.1371/journal.pone.0099133 (2014).
Tzanetakou, I. P., Katsilambros, N. L., Benetos, A., Mikhailidis, D. P. & Perrea, D. N. “Is obesity linked to aging?”: adipose tissue and the role of telomeres. Ageing Res Rev 11, 220–229, https://doi.org/10.1016/j.arr.2011.12.003 (2012).
Muezzinler, A., Zaineddin, A. K. & Brenner, H. Body mass index and leukocyte telomere length in adults: a systematic review and meta-analysis. Obes Rev 15, 192–201, https://doi.org/10.1111/obr.12126 (2014).
Capers, P. L., Kinsey, A. W., Miskell, E. L. & Affuso, O. Visual Representation of Body Shape in African-American and European American Women: Clinical Considerations. Clin Med Insights Womens Health 9, 63–70, https://doi.org/10.4137/CMWH.S37587 (2016).
Rimm, A. A., Hartz, A. J. & Fischer, M. E. A weight shape index for assessing risk of disease in 44,820 women. J Clin Epidemiol 41, 459–465 (1988).
Moller, R., Tafeit, E., Smolle, K. H. & Kullnig, P. “Lipometer”: determining the thickness of a subcutaneous fatty layer. Biosens Bioelectron 9, xiii–xvi (1994).
Mangge, H. et al. Subcutaneous adipose tissue distribution and telomere length. Clinical chemistry and laboratory medicine, https://doi.org/10.1515/cclm-2018-0801 (2019).
Moller, R., Tafeit, E., Sudi, K. & Reibnegger, G. Quantifying the ‘appleness’ or ‘pearness’ of the human body by subcutaneous adipose tissue distribution. Annals of human biology 27, 47–55 (2000).
Moeller, R. et al. Evaluation of risk profiles by subcutaneous adipose tissue topography in obese juveniles. Obesity 15, 1319–1324, https://doi.org/10.1038/oby.2007.154 (2007).
Moller, R., Tafeit, E., Pieber, T. R., Sudi, K. & Reibnegger, G. Measurement of subcutaneous adipose tissue topography (SAT-Top) by means of a new optical device, LIPOMETER, and the evaluation of standard factor coefficients in healthy subjects. American journal of human biology: the official journal of the Human Biology Council 12, 231–239, 10.1002/(SICI)1520-6300(200003/04)12:2<231::AID-AJHB9>3.0.CO;2-X (2000).
Cawthon, R. M. Telomere measurement by quantitative PCR. Nucleic acids research 30, e47 (2002).
Matthews, D. R. et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Kiechl, S. & Willeit, J. The natural course of atherosclerosis. Part II: vascular remodeling. Bruneck Study Group. Arterioscler Thromb Vasc Biol 19, 1491–1498 (1999).
Pignoli, P. & Longo, T. Ultrasound evaluation of atherosclerosis. Methodological problems and technological developments. Eur Surg Res 18, 238–253 (1986).
Pignoli, P., Tremoli, E., Poli, A., Oreste, P. & Paoletti, R. Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation 74, 1399–1406 (1986).
Dai, Y., Wan, X., Li, X., Jin, E. & Li, X. Neck circumference and future cardiovascular events in a high-risk population–A prospective cohort study. Lipids in health and disease 15, 46, https://doi.org/10.1186/s12944-016-0218-3 (2016).
Batsis, J. A. et al. Association of adiposity, telomere length and mortality: data from the NHANES 1999-2002. Int J Obes (Lond) 42, 198–204, https://doi.org/10.1038/ijo.2017.202 (2018).
Iglesias Molli, A. E. et al. Metabolically healthy obese women have longer telomere length than obese women with metabolic syndrome. PloS one 12, e0174945, https://doi.org/10.1371/journal.pone.0174945 (2017).
Guzzardi, M. A., Iozzo, P., Salonen, M. K., Kajantie, E. & Eriksson, J. G. Maternal adiposity and infancy growth predict later telomere length: a longitudinal cohort study. Int J Obes (Lond) 40, 1063–1069, https://doi.org/10.1038/ijo.2016.58 (2016).
Muezzinler, A. et al. Body mass index and leukocyte telomere length dynamics among older adults: Results from the ESTHER cohort. Exp Gerontol 74, 1–8, https://doi.org/10.1016/j.exger.2015.11.019 (2016).
Mundstock, E. et al. Effect of obesity on telomere length: Systematic review and meta-analysis. Obesity 23, 2165–2174, https://doi.org/10.1002/oby.21183 (2015).
Chen, S. et al. Short leukocyte telomere length is associated with obesity in American Indians: the Strong Heart Family study. Aging (Albany NY) 6, 380–389, https://doi.org/10.18632/aging.100664 (2014).
Garcia-Calzon, S. et al. Longitudinal association of telomere length and obesity indices in an intervention study with a Mediterranean diet: the PREDIMED-NAVARRA trial. Int J Obes (Lond) 38, 177–182, https://doi.org/10.1038/ijo.2013.68 (2014).
Gielen, M. et al. Body mass index is negatively associated with telomere length: a collaborative cross-sectional meta-analysis of 87 observational studies. Am J Clin Nutr 108, 453–475, https://doi.org/10.1093/ajcn/nqy107 (2018).
Dershem, R. et al. Changes in telomere length 3-5 years after gastric bypass surgery. Int J Obes (Lond) 41, 1718–1720, https://doi.org/10.1038/ijo.2017.156 (2017).
Buxton, J. L. et al. Childhood obesity is associated with shorter leukocyte telomere length. The Journal of clinical endocrinology and metabolism 96, 1500–1505, https://doi.org/10.1210/jc.2010-2924 (2011).
You, N. C. et al. A prospective study of leukocyte telomere length and risk of type 2 diabetes in postmenopausal women. Diabetes 61, 2998–3004, https://doi.org/10.2337/db12-0241 (2012).
Weale, C. J. et al. Leucocyte Telomere Length and Glucose Tolerance Status in Mixed-Ancestry South Africans. Cells 8, https://doi.org/10.3390/cells8050464 (2019).
Gustafson, B. & Smith, U. Regulation of white adipogenesis and its relation to ectopic fat accumulation and cardiovascular risk. Atherosclerosis 241, 27–35, https://doi.org/10.1016/j.atherosclerosis.2015.04.812 (2015).
Weghuber, D. et al. High risk vs. “metabolically healthy” phenotype in juvenile obesity - neck subcutaneous adipose tissue and serum uric acid are clinically relevant. Experimental and clinical endocrinology & diabetes: official journal, German Society of Endocrinology [and] German Diabetes Association 121, 384–390, https://doi.org/10.1055/s-0033-1341440 (2013).
Mangge, H. et al. Nuchal thickness of subcutaneous adipose tissue is tightly associated with an increased LMW/total adiponectin ratio in obese juveniles. Atherosclerosis 203, 277–283, https://doi.org/10.1016/j.atherosclerosis.2008.06.013 (2009).
Mangge, H. et al. Branched-chain amino acids are associated with cardiometabolic risk profiles found already in lean, overweight and obese young. The Journal of nutritional biochemistry 32, 123–127, https://doi.org/10.1016/j.jnutbio.2016.02.007 (2016).
Weghuber, D., Mangge, H., Hochbrugger, E. & Stulnig, T. M. Impact of age and metabolic syndrome on the adipokine profile in childhood and adult obesity. Experimental and clinical endocrinology & diabetes: official journal, German Society of Endocrinology [and] German Diabetes Association 122, 363–367, https://doi.org/10.1055/s-0034-1375647 (2014).
Mangge, H. et al. Antioxidant food supplements and obesity-related inflammation. Current medicinal chemistry 20, 2330–2337 (2013).
Stelzer, I. et al. Link between leptin and interleukin-6 levels in the initial phase of obesity related inflammation. Translational research: the journal of laboratory and clinical medicine 159, 118–124, https://doi.org/10.1016/j.trsl.2011.10.001 (2012).
Pruller, F. et al. Trunk weighted obesity, cholesterol levels and low grade inflammation are main determinants for enhanced thrombin generation. Atherosclerosis 220, 215–218, https://doi.org/10.1016/j.atherosclerosis.2011.09.035 (2012).
Gruber, H. J. et al. Obesity reduces the bioavailability of nitric oxide in juveniles. Int J Obes (Lond) 32, 826–831, https://doi.org/10.1038/sj.ijo.0803795 (2008).
Mangge, H. et al. Low grade inflammation in juvenile obesity and type 1 diabetes associated with early signs of atherosclerosis. Experimental and clinical endocrinology & diabetes: official journal, German Society of Endocrinology [and] German Diabetes Association 112, 378–382, https://doi.org/10.1055/s-2004-821023 (2004).
Rode, L., Nordestgaard, B. G., Weischer, M. & Bojesen, S. E. Increased body mass index, elevated C-reactive protein, and short telomere length. The Journal of clinical endocrinology and metabolism 99, E1671–1675, https://doi.org/10.1210/jc.2014-1161 (2014).
Al-Attas, O. S. et al. Adiposity and insulin resistance correlate with telomere length in middle-aged Arabs: the influence of circulating adiponectin. Eur J Endocrinol 163, 601–607, https://doi.org/10.1530/EJE-10-0241 (2010).
Broer, L. et al. Association of adiponectin and leptin with relative telomere length in seven independent cohorts including 11,448 participants. Eur J Epidemiol 29, 629–638, https://doi.org/10.1007/s10654-014-9940-1 (2014).
Zhang, J. et al. Ageing and the telomere connection: An intimate relationship with inflammation. Ageing Res Rev 25, 55–69, https://doi.org/10.1016/j.arr.2015.11.006 (2016).
Wu, Y., Cui, W., Zhang, D., Wu, W. & Yang, Z. The shortening of leukocyte telomere length relates to DNA hypermethylation of LINE-1 in type 2 diabetes mellitus. Oncotarget 8, 73964–73973, https://doi.org/10.18632/oncotarget.18167 (2017).
Zee, R. Y., Castonguay, A. J., Barton, N. S., Germer, S. & Martin, M. Mean leukocyte telomere length shortening and type 2 diabetes mellitus: a case-control study. Translational research: the journal of laboratory and clinical medicine 155, 166–169, https://doi.org/10.1016/j.trsl.2009.09.012 (2010).
Shen, Q. et al. Association of leukocyte telomere length with type 2 diabetes in mainland Chinese populations. The Journal of clinical endocrinology and metabolism 97, 1371–1374, https://doi.org/10.1210/jc.2011-1562 (2012).
Rorsman, P. & Braun, M. Regulation of insulin secretion in human pancreatic islets. Annu Rev Physiol 75, 155–179, https://doi.org/10.1146/annurev-physiol-030212-183754 (2013).
Deelen, J. et al. A metabolic profile of all-cause mortality risk identified in an observational study of 44,168 individuals. Nat Commun 10, 3346, https://doi.org/10.1038/s41467-019-11311-9 (2019).
Sathishkumar, C., Prabu, P., Mohan, V. & Balasubramanyam, M. Linking a role of lncRNAs (long non-coding RNAs) with insulin resistance, accelerated senescence, and inflammation in patients with type 2 diabetes. Hum Genomics 12, 41, https://doi.org/10.1186/s40246-018-0173-3 (2018).
Strazhesko, I. D. et al. Growth Hormone, Insulin-Like Growth Factor-1, Insulin Resistance, and Leukocyte Telomere Length as Determinants of Arterial Aging in Subjects Free of Cardiovascular Diseases. Front Genet 8, 198, https://doi.org/10.3389/fgene.2017.00198 (2017).
Preis, S. R. et al. Neck circumference as a novel measure of cardiometabolic risk: the Framingham Heart study. J Clin Endocrinol Metab 95, 3701–3710, https://doi.org/10.1210/jc.2009-1779 (2010).
Caro, P., Guerra, X., Canals, A., Weisstaub, G. & Sandana, C. Is neck circumference an appropriate tool to predict cardiovascular risk in clinical practice? A cross-sectional study in Chilean population. BMJ Open 9, e028305, https://doi.org/10.1136/bmjopen-2018-028305 (2019).
Koppad, A. K., Kaulgud, R. S. & Arun, B. S. A Study of Correlation of Neck Circumference with Framingham Risk Score as a Predictor of Coronary Artery Disease. J Clin Diagn Res 11, OC17–OC20, https://doi.org/10.7860/JCDR/2017/25710.10609 (2017).
Makino, N., Maeda, T. & Abe, N. Short telomere subtelomeric hypomethylation is associated with telomere attrition in elderly diabetic patients (1). Can J Physiol Pharmacol 97, 335–339, https://doi.org/10.1139/cjpp-2018-0568 (2019).
Martinez, P. et al. RAP1 protects from obesity through its extratelomeric role regulating gene expression. Cell reports 3, 2059–2074, https://doi.org/10.1016/j.celrep.2013.05.030 (2013).
Yeung, F. et al. Nontelomeric role for Rap1 in regulating metabolism and protecting against obesity. Cell reports 3, 1847–1856, https://doi.org/10.1016/j.celrep.2013.05.032 (2013).
Acknowledgements
This work was funded by the ‘Zukunftsfond Steiermark’ Projects ‘STYJOBS’ and ‘STYJOBS-Extension’.
Author information
Authors and Affiliations
Contributions
H.M.: wrote the main manuscript text and prepared figures, he is PI of the STYJOBS project. M.H.: participated in preparation of the manuscript. G.A.: participated in management of the study and experimental settings. S.Z.: participated in analytical work. R.M.: participated in statistical analysis and lipometry. R.H.: participated in lipometry. W.R.: supervised the genetic analysis of telomeres.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mangge, H., Herrmann, M., Almer, G. et al. Telomere shortening associates with elevated insulin and nuchal fat accumulation. Sci Rep 10, 6863 (2020). https://doi.org/10.1038/s41598-020-63916-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-63916-6
This article is cited by
-
Study of association of leptin with leukocyte telomere length in a Chinese rural population
Lipids in Health and Disease (2024)
-
Obesity: a perfect storm for carcinogenesis
Cancer and Metastasis Reviews (2022)
-
Influence of Moxonidine and Bisoprolol on Morphofunctional Condition of Arterial Wall and Telomerase Activity in Postmenopausal Women with Arterial Hypertension and Osteopenia. The Results from a Moscow Randomized Study
Cardiovascular Drugs and Therapy (2022)
-
Association between telomere length and hepatic fibrosis in non-alcoholic fatty liver disease
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
