
Abstract
The implications of Zika Virus exposure in pregnancy for early infant growth remains poorly described. The main goal of this study is to compare the growth, body composition, and feeding modality of infants in the first three months of life by prenatal Zika Virus exposure status. We selected an analytical cohort of 115 infants born without microcephaly, comprising 56 infants with qRT-PCR confirmed exposure to ZIKV during gestation and 59 infants born to women with presumptively no evidence of ZIKV in pregnancy. Infants were evaluated at birth, 1 and 3 months of age in terms of anthropometrics, body composition All the results were adjusted by maternal age, maternal BMI and gestational age. We observe no differences between anthropometric measurements at birth. Mothers in exposed group showed higher BMI. At 1 month and 3 months of age there were differences in mid arm circumference, arm muscle circumference and fat free mass. Weight and length was less in the ZIKV exposed in pregnancy infants and statistically different at 3 month of age. The findings of this investigation provide new evidence that ZIKV exposure in pregnancy may be associated with differences in body composition.
Similar content being viewed by others

Introduction
In early 2015, Brazilian public health authorities first identified an increase in a “dengue-like illness”1, subsequently laboratory-confirmed to be caused by Zika virus (ZIKV)1,2. After its emergence in Brazil, ZIKV spread rapidly through the Americas, and, by March 2017, arthropod-borne transmission was reported in more than 80 countries worldwide3. While typically recognized to cause a mild and often asymptomatic presentation among adults4, vertical transmission of ZIKV in pregnancy has been associated with severe fetal consequences, leading to microcephaly5,6 and the wider Congenital Zika Syndrome (CZS) in affected neonates7. Although a series of recent prospective cohort studies has confirmed the links between ZIKV exposure in pregnancy and adverse birth outcomes and neurologic sequelae8,9,10,11, the impact of ZIKV infection in pregnancy on infant growth and body composition–and any potential mediating role of feeding modality–remains unknown.
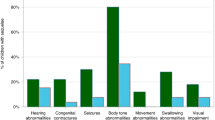
We hypothesized that ZIKV infections in pregnancy may be associated with compromised infant development. Infections during pregnancy are not infrequent, and a growing body of literature has reported associations between prenatal exposure to infectious diseases, including human immunodeficiency virus (HIV)12,13 and malaria14,15,16, with childhood growth patterns. Similarly, it is also known that, among children with neurologic impairment, such as that associated with cerebral palsy, feeding difficulties are prevalent17 and may contribute to inhibited growth18. Indeed, several case series indicate that children with neurologic damage from congenital ZIKV infections may be at heightened risk of dysphagia19,20, arising from dysfunction in tongue movement and the pharyngeal phase of swallowing21.
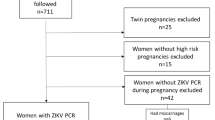
To test this hypothesis, we followed up a subset of 115 infants without microcephaly who were participating in a prospective cohort study of children born during the ZIKV epidemic in Brazil. In comparing 56 infants with qtRT-PCR (Quantitative Reverse Transcription-Polymerase Chain Reaction) confirmed exposure to ZIKV during gestation with 59 infants born to women with no evidence of ZIKV in pregnancy, we aimed to improve understanding of how prenatal ZIKV exposure may influence the growth, body composition, and feeding modality of infants in the first three months of life.
Methods
Study design and participants
As part of an on-going prospective cohort study (clinicaltrials.gov NCT 03255369) based in Rio de Janeiro, Brazil, at the Instituto Fernandes Figueira of the Fundação Oswaldo Cruz (IFF-Fiocruz; http://www.iff.fiocruz.br/), the present work compares the growth, body composition, and feeding of infants exposed and unexposed to ZIKV during gestation. The analytical cohort includes new mothers and full-term neonates delivered at IFF-Fiocruz between June 2016 and September 2017 and excludes dyads whose infants were: (i) diagnosed with microcephaly (i.e., defined as a head circumference of <−2 standard deviations (SDs) (ii) diagnosed with chromosomal abnormalities (i.e., prenatally or at birth), (iii) diagnosed with a congenital infection from toxoplasmosis, rubella, cytomegalovirus, and herpes virus, or (iv) born to mothers with human immunodeficiency virus (HIV).
Maternal-child dyads were categorized by prenatal ZIKV exposure status. The exposed group comprised new mothers and neonates with symptomatic (i.e., presenting with exanthema, fever associated with arthralgia, myalgia, non-purulent conjunctivitis, and/or headache) and quantitative reverse transcription polymerase chain reaction (qRT-PCR)-confirmed ZIKV infections during pregnancy. The unexposed group comprised new mothers and neonates for whom there was no evidence of ZIKV infection during pregnancy (i.e., defined by the lack of maternal symptoms in pregnancy. As we did not have a good serological test to prevent the inclusion of exposed children from mothers who had asymptomatic infection, we included only mothers who had good adherence to mosquito bite prevention strategies- use of repellents and appropriate clothing to be worn during the epidemic). These infants were classified with presumptively unexposed.
Clinical evaluation
Participating infants were clinically evaluated by trained researchers at birth, 1 and 3 months of age. it was accepted a variation of 15 days in these ages. During the study visits, researchers measured the following anthropometric variables in order to evaluate growth and body composition using WHO (World Health Organization) standard procedures22: weight (g), length (cm), cephalic perimeter (cm), abdominal circumference (cm), mid-arm circumference (cm), and triceps skinfold (mm).
Additional body composition indicators (i.e., percentage body water, percentage body fat, fat mass (g), and fat-free mass (g)) were assessed using electric bioimpedance and air displacement plethysmography. For total body water evaluation using biompedance (Quantum BIA 101Q device, RJL Systems, Inc., Clinton Townships, Michigan, USA), the electrodes were fixed on the right hand and foot with at least a 3 cm distance between them. The arms were kept away from the trunk, and the legs were kept apart. To record the measurement, the newborn infant was comfortable and quiet. The value of the resistance was recorded to calculate body water. The equation that was used to calculate total body water was proposed and validated by Tang, et al. using the technique of dilution with water marked with oxygen 18 isotope23. This equation uses two anthropometric measures (i.e., weight and foot length) and resistance (R) measured by electrical bioimpedance. The percentage of fat and fat-free mass was obtained through air displacement plethysmography (Pea Pod® Infant Body Composition System, Life Measurement, Inc., Concord, CA), which provides a safe and valid method to assess body composition of a newborn24,25. The muscular circumference of the arm was calculated with the circumference measurements of the mid-arm (cm) and triceps skinfold (mm, using the formula proposed by Frisancho26: Muscle Circumference of the Arm = Circumference of the Mid-Arm - (3.14 x Triceps Skinfold/10).
Nutritional status was evaluated using Z-score indices of weight, length, and head circunference for gestational age and sex based on WHO published data27. Additional information was collected on infant feeding, including: frequency, volume, and type (i.e., breast or formula milk). The presence of signs of dysphagia were also investigated (Dysphagia was reported by families with hypersalivation and difficulty in swallowing and confirmed by clinical examination or videofluoroscopy).
None of the exams required sedation or food breaks for the infant. In case of crying or irritation, the maternal breast was offered for 10 minutes if the mother was present and available for breastfeeding. Otherwise, infants were provided with 2 ml of a 10% glucose solution.
Laboratory procedures
All the mothers had positive Real-time reverse transcriptase-polimerase chain reaction (RT-PCR) assays for ZIKV were perfomed with the QuantiTect probe RT-PCR kit (Qiagen) at Fiocruz in the group considered exposed group. Mothers of infants in the not exposed group had no symptoms of Zika Virus during pregnancy and we try to use infants that was born before the outbreak. We collected blood from
Statistical analyses
The results were adjusted by maternal BMI (body mass index), maternal age and gestational age at birth. All P values are from 2-sided statistical tests, with a significance level of 5%. All data were entered into the Epi Info (Centers for Disease Control and Prevention, Atlanta, GA, USA), and all analyses were performed using the IBM SPSS Statistics, version 21.0 (Portsmouth, Hampshire, UK).
Ethics
The project “Vertical Exposure to Zika Virus and its consequences on the development of the newborn”, of which this study is part of, was approved by the Ethics Committee in Human Research of IFF/Fiocruz under CAAE 52675616.0.0000.5269 and registered as NCT 03255369. The study was conducted in accordance with the Declaration of Helsinki, the International Conference on Harmonization guideline for Good Clinical Practice, and the codes and regulations of Brazil regarding research on human subjects. Infants were included in the study after their legal guardian(s) signed the Free and Informed Consent Form. The funders of the study had no role in data collection, analysis, or interpretation.
Results
The study population consisted of a total of 115 infants, of whom 56 (48.7%) were intra-uterus exposed to ZIKV and 59 (51.3%) were unexposed. Among the ZIKV-exposed group, women tested RT-PCR positive in 24.1% of cases in the first trimester of gestation, 64.8% in the second trimester and 11.1% in the third trimester. Maternal anthropometric and comorbidity characteristics during pregnancy are described in Table 1. ZIKV-exposed women were on average older than ZIKV-unexposed women (30.1 years versus 29.5 years) although this was not statistically significant. Women exposed to ZIKV had a significantly higher BMI (26.6 versus 24, p = 0.013) and were more likely to be overweight/obese (58% versus 33.3%, P < 0.044) than unexposed women. A higher proportion of ZIKV-exposed women had hypertension (20% versus 12%) and diabetes (9.1% versus 5.2%) during pregnancy compared to unexposed women, although this was not statistically significant.
ZIKV-exposed infants were born, on average, one week before ZIKV-unexposed infants (38.5 weeks versus 39.1 weeks, p < 0.008) but still within the definition of full-term (>37 weeks) (Table 2). The mean weight (3275 g versus 3230 g), lenght (48.2 versus 50.4) and head circumference (34.9 cm versus 34.5 cm) at birth of infants exposed and unexposed to ZIKV did not differ significantly.
At the first infant follow-up, carried out during the first month of life, ZIKV-exposed infants exhibited no differences in length, triceps skinfold, body fat percentage, fat mass and fat free mas compared to unexposed infants (Tables 2 and 3). In addition, mid arm circumference and arm muscle circumference at 1 and 3 months of age were significantly lower among ZIKV-exposed compared to unexposed infants. However, when followed-up in the third month of life, the only variables that remained significantly different between exposed and unexposed infants were weight, length, mid arm circumference, arm muscle circumferences, fat free mass (Tables 2 and 3).
Among ZIKV-exposed infants, 37.8% were receiving some formula milk within the first month of life (compared to only 8.1% of unexposed infants, p = 0.002) and by the third month of life, 48.3% of exposed infants compared to 22.2% of unexposed babies were receiving some formula milk (p = 0.038). We tested the relation between the use of milk formula and the percentage of fat free mass, mid arm circumference and arm muscle circumference adjusting by group of exposition and we didn´t verify differences statistically significant. (p > 0.05)
Among ZIKV-exposed infants, 17.9% presented symptoms compatible with dysphagia (choking, hypersalivation, and reflux) and none in the not-exposed infants.
Discussion
The effects of vertical ZIKV transmission on infant growth and body composition remain unknown. The results of this study indicate that at three month of life, ZIKV-exposed neonates are significantly lighter, smaller and have a lower fat free mass compared to unexposed neonates.
Growth involves much more than just a quantitative increase in body mass. Growth is the result of a complex interaction between several factors, such as genetics, nutrition and the environment. Weight gain in growing infants and children is non-specific, and the increase in adiposity and accumulation of lean mass and bone mass are also non-specific28. Body composition is an auxiliary measure of growth that allows evaluation of the quality of the weight gain. The body composition profiles of unexposed neonates in this study were comparative to healthy term infants as reported by Field, et al.29, who analysed 160 healthy term infants who were exclusively breastfed for 6 months. According to a body composition reference curve proposed by these authors, it is expected that at 1 month, infants have approximately 18 to 19.4% body fat. In our cohort, ZIKV-exposed infants presented with 20,5% body fat at one month of age. However, we observed some improvement in growth and an increase of 20% in body fat composition from the first to the third month of life. We hypothesize that as ZIKV-exposed babies have more difficulties with feeding and swallowing, that this may have led to an earlier introduction of formula milk via bottle. As an increased consumption of artificial formula milk during infancy results in an increase in fat mass30, this may have produced the catch-up growth observed in our study in ZIKV-exposed infants between one and three months of age.
In the case of neonates congenitally exposed to ZIKV, it is still not known to what extent ZIKV alters the intrauterine milieu and what effects this could have on the growth and body composition of the developing fetus during pregnancy. Studies have demonstrated that both nutritional deprivation and excessive intake by the fetus may affect gene expression in the neonate and have deleterious effects on its overall health31. A study performed by Brasil et al.32 in Rio de Janeiro with 125 ZIKV-positive pregnant women demonstrated that 46% of the neonates presented with global adverse neurological outcomes, such as seizures, hypertonia, hyperreflexia, and varying levels of neurodevelopmental delay; these outcomes are not completely understood to date. In this study, 17.9% of ZIKV-exposed infants had symptoms compatible with an impaired swallow and reflux. Thus, a timely diagnosis and early nutritional intervention would benefit these infants in the short and long term.
Nutritional intervention is still somewhat controversial and should be based on an individual patient-centered risk-benefit analysis. There is a consensus that optimal neurodevelopmental support is the highest priority, and therefore, like in preterm neonates, the current nutritional policy for ZIKV-exposed neonates seems to involve enhancing protein and energy consumption to promote growth and improve cognitive function. Therefore, the early introduction of formula milk has become commonplace to try meet nutritional demands and support infants with swallowing difficulties or neurodevelopmental delay.
According to the World Health Organization, adequate infant feeding comprises the practice of breastfeeding until 6 months of age and, at this point, the timely introduction of complementary feeding33,34. Of note, there is no recommendation to discontinue breastfeeding in mothers with concomitant ZIKV infections or in infants prenatally exposed to ZIKV34. However, it is not known whether ZIKV-exposed infants have more difficulties with breastfeeding due to dysphagia, or whether the early introduction of formula milk and discontinuation of breastfeeding could affect the mother/infant bond in ZIKV-exposed infants. In addition, it is unclear whether the total energy requirements described in the literature for healthy infants are sufficient for the maintenance of adequate growth, and body fat composition of ZIKV-exposed infants. However, it is likely that, by promoting growth and optimal neurodevelopment, early nutritional intervention could modify the life history of a ZIKV-exposed child (reviewed in35,36).
This study had limitations. One of the limitations of this study is the possibility that some of the ZIKV-unexposed women were in fact exposed to ZIKV during pregnancy. This is due to the challenges of acute ZIKV diagnosis given the fact that the majority of infections are asymptomatic. Because a sufficiently sensitive and specific serological test is not available, we need to include infants whose mothers had a good adherence to methods to prevent the infection. Then, we classified them in presumptively unexposed children.
Long-term studies with clinical and nutritional follow-up are needed to develop standardized protocols for the care of ZIKV-exposed pregnant women and their neonates. These would aim to promote and optimize both intrauterine and postnatal growth and minimize the risk of comorbidities, thereby stimulating maximum neurodevelopmental potential.
Clinical Trials Registry: NCT 03255369.
References
Zanluca, C. et al. First report of autochthonous transmission of Zika virus in Brazil. Mem. Inst. Oswaldo Cruz 110, 569–572 (2015).
Campos, G. S., Bandeira, A. C. & Sardi, S. I. Zika Virus Outbreak, Bahia, Brazil. Emerg. Infect. Dis. 21, 1885–1886 (2015).
World Health Organization. WHO | Zika virus, Microcephaly and Guillain-Barré syndrome. WHO (2016).
Duffy, M. R. et al. Zika Virus Outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 360, 2536–2543 (2009).
de Araújo, T. V. B. et al. Association between microcephaly, Zika virus infection, and other risk factors in Brazil: final report of a case-control study. Lancet Infect. Dis. 18, 328–336 (2018).
de Araújo, T. V. B. et al. Association between Zika virus infection and microcephaly in Brazil, January to May, 2016: preliminary report of a case-control study. Lancet. Infect. Dis. 16, 1356–1363 (2016).
Miranda-Filho, DdeB. et al. Initial Description of the Presumed Congenital Zika Syndrome. Am. J. Public Health 106, 598–600 (2016).
Pomar, L. et al. Maternal-fetal transmission and adverse perinatal outcomes in pregnant women infected with Zika virus: prospective cohort study in French Guiana. BMJ 363, k4431 (2018).
Reynolds, M. R. et al. Vital Signs: Update on Zika Virus–Associated Birth Defects and Evaluation of All U.S. Infants with Congenital Zika Virus Exposure — U.S. Zika Pregnancy Registry, 2016. MMWR. Morb. Mortal. Wkly. Rep. 66, 366–373 (2017).
Rice, M. E. et al. Vital Signs: Zika-Associated Birth Defects and Neurodevelopmental Abnormalities Possibly Associated with Congenital Zika Virus Infection — U.S. Territories and Freely Associated States, 2018. MMWR. Morb. Mortal. Wkly. Rep. 67, 858–867 (2018).
Hoen, B. et al. Pregnancy Outcomes after ZIKV Infection in French Territories in the Americas. N. Engl. J. Med. 378, 985–994 (2018).
Makasa, M. et al. Early growth of infants of HIV-infected and uninfected Zambian women. Trop. Med. Int. Heal. 12, 594–602 (2007).
Nicholson, L., Chisenga, M., Siame, J., Kasonka, L. & Filteau, S. Growth and health outcomes at school age in HIV-exposed, uninfected Zambian children: follow-up of two cohorts studied in infancy. BMC Pediatr. 15, 66 (2015).
De Beaudrap, P. et al. Timing of malaria in pregnancy and impact on infant growth and morbidity: a cohort study in Uganda. Malar. J. 15, 92 (2016).
Walther, B. et al. Placental Malaria is associated with reduced early life weight development of affected children independent of low birth weight. Malar. J. 9, 16 (2010).
Kalanda, B. F., van Buuren, S., Verhoeff, F. H. & Brabin, B. J. Catch-up growth in Malawian babies, a longitudinal study of normal and low birthweight babies born in a malarious endemic area. Early Hum. Dev. 81, 841–850 (2005).
Sullivan, P. B. et al. Prevalence and severity of feeding and nutritional problems in children with neurological impairment: Oxford Feeding Study. Dev. Med. Child Neurol. 42, 674–80 (2000).
Fung, E. B. et al. Feeding dysfunction is associated with poor growth and health status in children with cerebral palsy. J. Am. Diet. Assoc. 102, 361–73 (2002).
van der Linden, V. et al. Description of 13 Infants Born During October 2015–January 2016 With Congenital Zika Virus Infection Without Microcephaly at Birth — Brazil. MMWR. Morb. Mortal. Wkly. Rep. 65, 1343–1348 (2016).
van der Linden, V. et al. Congenital Zika syndrome with arthrogryposis: retrospective case series study. BMJ 354, i3899 (2016).
Leal, M. C. et al. Characteristics of Dysphagia in Infants with Microcephaly Caused by Congenital Zika Virus Infection, Brazil, 2015. Emerg. Infect. Dis. 23, 1253–1259 (2017).
World Health Organization. WHO | Physical status: the use and interpretation of anthropometry. WHO (2013).
Tang, W., Ridout, D. & Modi, N. Assessment of total body water using bioelectrical impedance analysis in neonates receiving intensive care. Arch. Dis. Child. Fetal Neonatal Ed. 77, F123–6 (1997).
Yao, M., Nommsen-Rivers, L., Dewey, K. & Urlando, A. Preliminary evaluation of a new pediatric air displacement plethysmograph for body composition assessment in infants. Acta Diabetol. 40, s55–s58 (2003).
Ma, G. et al. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 79, 653–660 (2004).
Frisancho, A. R. Anthropometric standards for the assessment of growth and nutritional status. Clin. Nutr. 10, 131–132 (1991).
WHO Multicentre Growth Reference Study Group. Assessment of differences in linear growth among populations in the WHO Multicentre Growth Reference Study. Acta Paediatr. Suppl. 450, 56–65 (2006).
Perng, W. et al. An observational cohort study of weight- and length-derived anthropometric indicators with body composition at birth and 5 mo: the Healthy Start study. Am. J. Clin. Nutr. 106, 559–567 (2017).
Fields, D. A. et al. Longitudinal Body Composition Data in Exclusively Breast-Fed Infants: A Multicenter Study. Obesity 19, 1887–1891 (2011).
Mameli, C., Mazzantini, S. & Zuccotti, G. Nutrition in the First 1000 Days: The Origin of Childhood Obesity. Int. J. Environ. Res. Public Health 13, 838 (2016).
Hortencio, T. D. R. et al. Factors impacting the growth and nutritional status of cystic fibrosis patients younger than 10 years of age who did not undergo neonatal screening. Rev. Paul. Pediatr. 33, 3–11 (2015).
Brasil, P. et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro. N. Engl. J. Med. 375, 2321–2334 (2016).
Victora, C. G. et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet (London, England) 387, 475–90 (2016).
Organization, W. H. WHO|IHR Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations. WHO (2017).
Moreira, M. E. L. & Goldani, M. Z. Child is the father of man: new challenges for child health. Ciência & Saúde Coletiva 15, 321–327 (2010).
Woo Baidal, J. A. et al. Risk Factors for Childhood Obesity in the First 1,000 Days. Am. J. Prev. Med. 50, 761–779 (2016).
Acknowledgements
CNPq 441098/2016-9 and 305090/2016-0; Faperj E_18/2015TXB; Wellcome Trust & the United Kingdom’s Department for International Development (205377/Z/16/Z); European Union’s Horizon 2020 research and innovation programme under Zika-PLAN grant agreement no. 734584.
Author information
Authors and Affiliations
Contributions
A.D.A., S.L., L.V., D.A., S.N., L.S., Y.A., S.P. and M.P. acquisition, analysis, and interpretation of data. They revised and approve the final version of the manuscript. F.S., M.E.M., S.C.G.J., P.B. and K.N.-S.: conception, design of the work; the acquisition, analysis, interpretation of data and wrote and revision the manuscript approving the final version of the manuscript. L.L., N.S.C. and E.B. conceptions and design, wrote, revision and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Soares, F., Abranches, A.D., Villela, L. et al. Zika virus infection in pregnancy and infant growth, body composition in the first three months of life: a cohort study. Sci Rep 9, 19198 (2019). https://doi.org/10.1038/s41598-019-55598-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-55598-6
This article is cited by
-
Feeding characteristics and growth among children with prenatal exposure to Zika virus with and without microcephaly in the microcephaly epidemic research group pediatric cohort
BMC Pediatrics (2024)
-
Characteristics of children of the Microcephaly Epidemic Research Group Pediatric Cohort who developed postnatal microcephaly
Scientific Reports (2022)
-
Cross-sectional study of the anthropometric characteristics of children with congenital Zika syndrome up to 12 months of life
BMC Pediatrics (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
