
Abstract
UNAIDS report documents 95% increase in new HIV infections among key populations in Eastern Europe and Middle East and North Africa region. Data on HIV and STIs among MSM in Lebanon is still scarce. Therefore, the aim was to assess prevalence of HIV and sexually transmitted infections (STIs) among men who have sex with men (MSM) in Lebanon and associations with sexual practices and substance-use. 2238 MSM attended a sexual health clinic in Lebanon between 2015–2018. Demographics, substance-use and sexual practices were collected. Attendees tested for HIV and other STIs. HIV infection was diagnosed in 5.6% of the sample. Only 19% received sexual health education from reliable sources (school/university/healthcare workers), 78% reported having multiple partners in the past three months (2–5 partners: 58%, 6+: 20%) and 67% reported inconsistent condom-use. Moreover, 40% of HIV + cases were returning attendees who already received information about condom-use. Additionally, having only a school level education (11%) increases the odds of having inconsistent condom-use with casual partners (adj.OR:1.9, p < 0.001). The results reflect the urgent need for: (1) accurate and comprehensive sexual health and harm reduction education and promotion in Lebanon; (2) making pre-exposure prophylaxis available for free to key populations to contain the epidemics at an early stage.
Similar content being viewed by others

Introduction
The UNAIDS shared in July 2018 the alarming numbers of new human immunodeficiency virus (HIV) infections in key populations: 47% increase globally, 95% increase in Eastern Europe and Central Asia as well as in the Middle East and North Africa (MENA)1. The risk of acquiring HIV is 27 times higher among men who have sex with men (MSM), compared to men who have sex with women globally1. With the emergence of more data on HIV in the MENA region, hidden epidemics among key population groups, such as MSM, have not only been identified across the region but may also be growing in size2, mirroring the latest findings of UNAIDS. While a number of studies have found high levels of risky sexual practices and substance use among MSM around the world3,4, there are insufficient data in the MENA region in general and in Lebanon in particular. Additionally, a global study conducted by the World Health Organization (WHO) in 2016 emphasized the importance of increasing research efforts on sexually transmitted infections (STIs) given the high rates of infections globally5.
Lebanon, a Middle Eastern country, remains conservative especially with topics related to sex and sexuality. Penal code 534 criminalizes sexual acts that are “against nature”; and is commonly used against the Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) community and particularly against MSM6. Substance use is also highly stigmatized and criminalized in Lebanon6. These punitive laws put additional strains on people living in Lebanon and especially those who are LGBTQ, thus limiting their access to necessary sexual health and harm reduction services7,8. The National AIDS Program (NAP) of the Ministry of Public Health in Lebanon (MOPH) reported a cumulative of 2366 people living with HIV (PLHIV) in Lebanon by the end of 20189. Few studies have investigated HIV prevalence among MSM in Lebanon10,11,12, their sexual practices10 or condom-use13. Furthermore, while a strong association between substance use and risky sexual practices was reported among the Lebanese youth14, this was not investigated among MSM specifically. A comprehensive evaluation of the relationship between HIV and STIs prevalence, sexual practices and substance use among MSM in Lebanon has never been addressed.
Thus, the aim of this study was to assess the associations of STIs, including HIV, with risky sexual practices and substance use among MSM attending a sexual health clinic in Lebanon.
Methods
Sample
Data were collected from individuals voluntarily attending Marsa sexual health center (a non-governmental organization) located in Beirut, Lebanon between January 1st, 2015 and December 31st, 2018 for voluntary counseling and testing (VCT) and/or medical consultation for symptoms related to STIs.
Healthcare professionals administered an anonymous questionnaire for each attendee prior to undergoing medical testing and/or medical consultation, and a file number was delivered to each attendee. Data from the questionnaire, testing and medical consultation were saved digitally under each file number and could only be viewed by selected health professionals at the clinic who had signed a confidentiality agreement. To ensure the attendees’ anonymity, a verbal consent was obtained prior to the administered questionnaire. Attendees who did not give verbal consent could opt-out of the questionnaire administered by the health professional. Those who opted out of answering the questionnaire still received testing services. Ethical considerations, including anonymity and consent, were approved by the IRB office of our academic institution (USJ2016-77). The methods were carried out in accordance with the relevant guidelines and regulations.
The inclusion criterion was being a cisgender man having sex with men. The questionnaire included sections on demographics, substance use, sexual practices and previous unprotected sexual exposures. Age was categorized into the following groups: <20, 20–24, 25–29, 30–34, 35–39, ≥40 years old. Attendees were also asked about sources of sexual health education. The following sources were considered as reliable: school, university and/or healthcare providers; the following sources were considered as unreliable: friends/peers, sexual partners, internet/pornography; and various sources were those who reported both (reliable and unreliable sources). Attendees were asked about substance-use: smoking, alcohol, and recreational drugs such as cannabis, cocaine, muscle relaxant (poppers), ecstasy, GHB (Gamma-HydroxyButyrate), MDMA (3,4-MethyleneDioxyMethAmphetamine), heroine, ketamine. The term recreational drug-use refers to the use of a psychoactive drug to induce an altered state of consciousness for pleasure. Attendees were also asked about condom-use during penetrative sex with exclusive partners, regular partners (frequent but not exclusive), and casual partners (one-time partners). The detailed collected data were displayed in Table 1.
Collected data
Attendees who underwent VCT were given the option of being tested for viral Hepatitis B (HBV), viral Hepatitis C (HCV), syphilis (at subsidized prices) and/or HIV (for free) using rapid tests (Abon®), and the results were collected. The HIV kit was a third-generation test. Individuals who were in their serological window period after having a risk of sexual exposure were asked to do the test after completion of the window period. The latest result was included in this study.
Prevalence of HIV was reported among new and returning attendees. Some of the rapid tests were not consistently available throughout the duration of the study, specifically for HCV. Positive results were complemented by laboratory testing for confirmation (Elisa 4G and Western Blot for HIV, VDRL for Syphilis, DNA/RNA PCR for Hepatitis B/C). Positive cases were immediately referred to the clinic’s physicians. Those who tested positive were not aware of their status prior to the test.
Symptoms indicative of other STIs were documented through medical consultations. Although medical laboratory tests were provided at subsidized cost, very few attendees chose to undergo these tests due to financial constraints. Therefore, treatment relied on symptomatic diagnosis.
The explored STIs were Neisseria gonorrhea Ng/Chlamydia trachomatis Ct (presence of discharge and burning sensation during urination, and/or diagnosed biologically by Multiplex PCR test), Human Papilloma Virus (HPV, presence of genital, anal, oral warts and/or diagnosed by histology), Herpes Simplex Virus (HSV, presence of herpes zoster), scabies (presence of scabies rash), and pubic lice (presence of lice in pubic area). Medical laboratory tests were based on anal, oral or intra-uretral swabs, urine sample, and/or blood sample.
Statistics
Prevalence of HIV, HBV, HCV, Syphilis, Ng/Ct, HPV, pubic lice and coinfections were reported. In order to predict possible determinants of testing positive for any STI, a univariate analysis (simple binomial regression) followed by a multivariate analysis (stepwise binomial regression models) were computed. The outcome variables of HIV, HBV, HCV and Syphilis were considered as dependent variables, while independent variables were all variables listed in the following categories: demographics, substance use, sexual practices, unprotected sexual exposures in the past three months.
In order to explore possible factors linked to condom and recreational drug use, a univariate analysis (simple binomial regression) followed by a multivariate analysis (stepwise binomial regression models) were performed. The dependent variable was either condom-use or recreational drug use, while the independent variables were variables listed in the following categories: demographics, substance use, sexual practices, and sexual exposures.
Only variables with significant correlations in the univariate analysis were included in the multivariate analysis. Adjusted Odds Ratios (Adj. OR) with their respective confidence intervals (CI) were reported for each model. The level of significance was set at 0.05. Statistics were performed under Xlstat® (version 19.02, Addinsoft, Paris, France) and SPSS® (version 20, IBM, Armonk, NY, USA).
Results
A total of 2238 MSM attendees presented to Marsa sexual health clinic between the 1st of January 2015 and the 31st of December 2018. From this sample, 1326 subjects attended the clinic only once, whereas 912 (41%) attended the clinic several times during the period of the study. In total, 1477 (66%) of the sample where residing in Beirut. All 2238 underwent VCT, 502 also underwent medical consultations.
Population characteristics
The age of the MSM sample ranged between 15 and 69 years old, with a median of 26 years (1st quartile: 23; 3rd quartile: 31). The results of demographics, substance use, sexual practices, and sexual exposures were displayed in Table 1.
Prevalence of STIs
Prevalence of HIV (5.6%), HPV (41.0%;), and other STIs were displayed in Table 2. From the 119 attendees who tested positive for HIV (5.6%), 48 were returning clients (40%). Prevalence of co-infections was as follows: HIV and Syphilis in three cases; HIV and HPV in 18 cases; HIV and Ng/Ct in four cases; HIV and HCV in two cases.
Statistical models were restricted to HIV and Syphilis due to the low prevalence of HBV and HCV. The multivariate analysis showed that:
-
(1)
HIV status was found to be significantly related to anal sex intercourse only (Table 3).
Table 3 Associations between HIV/Syphilis status and demographics, substance use, sexual practices and sexual exposures in MSM in Lebanon. -
(2)
Syphilis status was found to be significantly related with age only (Table 3).
Condom-use and other sexual practices
Inconsistent condom-use during anal sex were reported by 67% (Table 1). In addition, 78% had more than one sexual partner in the last three months. Having had condomless sex or having symptoms of an STI were the primary reasons for attending (69%). Among the reasons for the absence of condom-use, 19% were under the influence of a substance (alcohol in 71%, recreational drug in 14% and mixing alcohol with drugs in 15%). The majority reported unprotected oral and anal sex exposures in the past three months (99% and 53% respectively).
The mutinomial regression model showed that: 1) those who reported having only a school level education were found to be at greater odds of having inconsistent condom-use with casual partners compared to those who reported having a university level education (adj. OR: 1.9); 2) those who received sexual health education from unreliable sources were at higher odds of having inconsistent condom-use with casual partners compared to those who received it from reliable sources (adj. OR: 1.6); 3) Those who reported having condomless anal sex in the past 3 months were more likely to have inconsistent condom-use with casual partners compared to those who did not have condomless anal sex (adj. OR: 7.6; Table 4).
Substance use
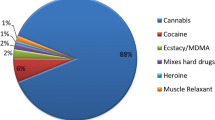
Cigarette smoking was reported in 35% of the sample, while 79% reported alcohol consumption and 29% reported using recreational drugs (details in Fig. 1). The binomial regression model showed that recreational drug use was found to be significantly associated with age, level of education, number of sexual partners, occupation, alcohol and smoking status; more precisely, those who reported having multiple partners (more than 2) in the last three months were found to be at greater odds of using recreational drugs (having between two to five partners adj. OR: 1.6, having between six to ten partners adj. OR: 2.7, having more than ten partners adj. OR: 3) than those who reported having 0 to 1 partner in the last three months (more details in Table 4).

Substance use in 2238 MSM in Lebanon: recreational drug use in addition to the reported types of drugs.
Discussion
Sex and sexuality are highly stigmatized in the MENA region and in Lebanon, especially for those with non-normative sexual practices. UNAIDS has drawn attention to the rising number of new HIV infections in the MENA region among key affected populations such as MSM. This study assessed the prevalence of HIV and other STIs as well as sexual practices and substance use among 2238 MSM in Lebanon. The prevalence of HIV was 5.6% (40% were returning attendees) and 41% presented with genital warts.
This study was based on attendees who voluntarily came to the clinic, most of them were young and were university students (47%), or had a university level education (89%), as in previous studies based on respondent driven samples (RDS)11. Sexual health education is not implemented in the majority of schools and universities in Lebanon, and there is little access to accurate and comprehensive information about sexual health. This is obvious in the result obtained in this study where only 19% of the sample received sexual health education from reliable sources.
Prevalence of HIV and other STIs in this study were higher than those reported in previous studies on MSM in Lebanon11,15. HIV prevalence in this study was 5.6% (out of 2126 MSM who underwent HIV testing) while it was 3.7% (out of 101 MSM)15, and 1.5% (out of 213 MSM)11 in previous studies. Only one local study found a higher HIV prevalence rate of 12.3% among its sample of 292 MSM recruited through RDS. However, the authors highlighted a number of factors that may have overestimated the rate of HIV prevalence such as: 1) the majority of HIV positive cases had already known their status prior to the study and 2) 25% of the sample were Syrian individuals who have moved to Lebanon recently12.
Even with the relatively lower prevalence of HBV compared to other STIs among our sample, it remains necessary to promote HBV testing and vaccination to key populations and particularly MSM in order to prevent further spread of the virus. The low prevalence of HCV among the sample (0.5%) could be indicative of a low prevalence of injection drug use16.
No official local data exist on prevalence of Syphilis, Ng/Ct among the MSM population in Lebanon. In this study, 3% of the MSM who underwent the syphilis rapid test had positive results, which is lower than previous reports in the literature17,18, notably among Chinese MSM (8%) and a sample of Peruvian MSM (4.4%). The positive association between syphilis and age may be attributed to greater time for exposure.
Furthermore, 17.5% of 502 individuals who sought medical consultation were treated for Ng/Ct based on indicative symptoms, a percentage higher than rates reported in a study on a sample of MSM in Germany19.
Genital warts were reported among 41% of the MSM who presented for medical consultations which is greater than the only other reported prevalence of HPV among MSM in Lebanon (10% among 42 MSM)20.
Upon examining common sexual practices, the majority had inconsistent condom-use (67%) as previously shown11. Among those, 46% reported inconsistent condom-use with casual partners, whose STI status (including HIV) was likely unknown to them, which would therefore put them at an increased risk of STIs. The model run on condom-use found that those who had only a school level education and those who reported receiving sexual health education from unreliable sources (such as peers, sexual partners, internet or pornography) were at higher odds of having inconsistent condom-use. This is likely attributed to the lack of sexual health education in the Lebanese educational system, especially at schools. These results should be used to lobby governmental agencies to include a comprehensive sexual health curriculum in schools.
While data on substance use and sexual practices among MSM exist across different regions, this is the first study to explore substance use among MSM in Lebanon. The connection between alcohol use and risky sexual practices among MSM has already been reported in previous studies in Australia21. This was also evident in this study where 19% of the sample stated that they did not use a condom during their last sexual intercourse because they were under the influence of a substance; among those alcohol being that substance in 71%.
With nearly one third of the sample reporting recreational drug use, further exploration of the determinants of drug use was warranted. No local sources were identified that evaluated drug use among MSM in Lebanon. However, various international sources attest to the fact that MSM are more likely to use drugs than their heterosexual peers22,23. Previous studies showed that drug use was found to be associated with different risky sexual practices22,23. The latter is concurrent with findings from this study, where MSM who reported multiple sexual partners in the past month, as well as those who were smokers, were at higher odds of using recreational drugs. Additionally, 29% of those who reported not using a condom because of substance use were using recreational drugs or mixing drugs with alcohol. The latter is also known to be a common trigger for risky sexual practices among MSM in different regions22,24.
This study has some limitations that should be considered. The quality of sexual health education provided in schools in Lebanon might vary, which could affect the efficacy of the results related to sexual health education. Additionally, a reporting bias might be present in the analysis as the topics discussed during the administered questionnaire are of a sensitive nature and therefore individuals might have refrained from disclosing risky sexual practices due to fears of being stigmatized. However, the sexual health center, that has been active since 2011, is well trusted by the MSM community for providing quality anonymous sexual health services in a non-stigmatizing and confidential environment. This will likely reduce the risk of reporting bias. Moreover, the heterogeneity of the sample with regards to age, nationality, education level etc. may affect the generalizability of the results.
However, to the best of our knowledge, this study remains the first comprehensive study to assess different STIs, sexual practices and substance use, including the largest number of MSM in Lebanon and MENA region25,26.
Another possible limitation might be the use of symptomatic methods of diagnosing Ng/Ct and HPV rather than laboratory testing. This was due to the high cost of laboratory testing that most attendees could not afford. However, symptoms such as genital warts or burning sensation during urination and/or penile or anal discharge are known to be indicative of HPV or Ng/Ct, respectively. In fact, it is likely that the reported prevalence of HPV and Ng/Ct are underestimated since these infections can be asymptomatic.
A sampling bias might also exist since this sample is comprised of individuals presenting to a sexual health clinic and therefore actively seeking STI testing and/or information regarding sexual health. They are therefore more likely to be sexually active and/or to have engaged in risky sexual practices. Nevertheless, the sample included in this study represents 37% of the MSM population estimated to be residing in Beirut27.
The relatively high prevalence of HIV detected in this study confirms the presence of pockets of endemic transmission among MSM which were not easily detected in previous studies conducted in Lebanon using RDS. Even though evidence of its success in decreasing new infections among some MSM communities has been documented28, pre-exposure prophylaxis (PrEP) is still not provided by the MOPH, except for married heterosexual sero-discordant couples, and is very expensive when purchased at pharmacies. Forty percent of those tested positive for HIV were returning attendees indicating that receiving information about condom-use to prevent HIV transmission, during their previous visit(s), was not sufficient. Negotiations with the MOPH and international agencies (UNAIDS and WHO) to make PrEP available to the MSM community in Lebanon for free or at a subsidized cost should be accelerated in order to contain the epidemic at an early stage. Similarly, the high prevalence of HPV indicates an urgent need for promoting screening and prevention through provision of HPV vaccine for free or at a subsidized cost.
Finally, advocacy efforts must highlight the importance of decriminalizing homosexuality to improve MSM’s access to HIV testing and other sexual health services. This is especially important since stigma has been found to deter the success of HIV prevention programs and activities28,29.
Conclusions
The results of this study portray the importance of enhancing sexual health services in Lebanon, especially with the rising prevalence of HIV and STIs locally and in the MENA region. These results are key in making a case to governmental and non-governmental institutions on the importance of promoting sexual health education and services, including making PrEP available and covering its cost for the MSM community, in order to contain the epidemics at an early stage. Additionally, the high prevalence of recreational drug use among the sample and its possible ties with risky sexual practices require efforts to advocate harm reduction and the breaking of prejudicial punitive laws and policies that are hindering access to services, consequently deterring the health of MSM and others.
References
UNAIDS. Fact sheet - Latest statistics on the status of the AIDS epidemic. 2017 GLOBAL HIV STATISTICS (2018).
Mumtaz, G. R., Riedner, G. & Abu-Raddad, L. J. The emerging face of the HIV epidemic in the Middle East and North Africa. Curr. Opin. HIV AIDS 9, 183–191 (2014).
Zellner, T. et al. Color it real: A program to increase condom use and reduce substance abuse and perceived stress. Int. J. Environ. Res. Public Health, https://doi.org/10.3390/ijerph13010051 (2015).
Vosburgh, H. W., Mansergh, G., Sullivan, P. S. & Purcell, D. W. A review of the literature on event-level substance use and sexual risk behavior among men who have sex with men. AIDS and Behavior, https://doi.org/10.1007/s10461-011-0131-8 (2012).
Rowley, J. et al. World Health Organization Global Health Sector Strategy on STIs (2016).
Jimenez, R. “It’s Part of the Job “ Ill-treatment and Torture of Vulnerable Groups in Lebanese Police Stations Cover design “ It’s Part of the Job “ Ill-treatment and Torture of Vulnerable Groups in Lebanese Police Stations. (2013).
Mumtaz, G. et al. Are HIV epidemics among men who have sex with men emerging in the middle east and north Africa? A systematic review and data synthesis. PLoS Medicine, https://doi.org/10.1371/journal.pmed.1000444 (2011).
Wagner, G. J., Hoover, M., Green, H., Tohme, J. & Mokhbat, J. Social, Relational and Network Determinants of Unprotected Anal Sex and HIV Testing Among Men Who Have Sex with Men in Beirut, Lebanon, https://doi.org/10.1080/19317611.2014.969467.
Ministry of Public Health in Lebanon- National Aids Control Program. Epidemiology World AIDS day 2017. (2017). Available at, https://www.moph.gov.lb/en/Pages/2/4000/aids.
Mahfoud, Z. et al. HIV/AIDS among female sex workers, injecting drug users and men who have sex with men in Lebanon: results of the first biobehavioral surveys. Wolters Kluwer Heal. 24, 45–54 (2010).
Wagner, G. J. et al. HIV Prevalence and Demographic Determinants of Unprotected Anal Sex and HIV Testing Among Men Who Have Sex with Men in Beirut, Lebanon. Arch Sex Behav 43, 779–788 (2014).
Heimer, R. et al. HIV Risk, Prevalence, and Access to Care Among Men Who Have Sex with Men in Lebanon. AIDS Res. Hum. Retroviruses 33, 1149–1154 (2017).
Wagner, G. J. et al. A Qualitative Exploration of Sexual Risk and HIV Testing Behaviors among Men Who Have Sex with Men in Beirut, Lebanon. PLoS One, https://doi.org/10.1371/journal.pone.0045566 (2012).
Ghandour, L. A., Mouhanna, F., Yasmine, R. & El Kak, F. Factors associated with alcohol and/or drug use at sexual debut among sexually active university students: cross-sectional findings from Lebanon. BMC Public Health, https://doi.org/10.1186/1471-2458-14-671 (2014).
Kassak, K. et al. Hepatitis B virus and hepatitis C virus infections among female sex workers and men who have sex with men in Lebanon: prevalence, risk behaviour and immune status. Sex. Health 8, 229 (2011).
Lee, M.-H., Yang, H.-I., Yuan, Y., L’Italien, G. & Chen, C.-J. Epidemiology and natural history of hepatitis C virus infection. World J. Gastroenterol. 20, 9270–80 (2014).
Tang, S. et al. HIV epidemiology and responses among men who have sex with men and transgender individuals in China: a scoping review. BMC Infect. Dis, https://doi.org/10.1186/s12879-016-1904-5 (2016).
Park, H. et al. Risk factors associated with incident syphilis in a cohort of high-risk men in peru. PLoS One, https://doi.org/10.1371/journal.pone.0162156 (2016).
Dudareva-Vizule, S. et al. Prevalence of pharyngeal and rectal Chlamydia trachomatis and Neisseria gonorrhoeae infections among men who have sex with men in Germany. Sex. Transm. Infect. 90, 46–51 (2014).
Maatouk, I. & Abdo, K. Human papillomavirus prevalence in the oral cavity of men who have sex with men: a study of its first from Beirut, Lebanon. Sex. Health 13, 397 (2016).
Lea, T. et al. Alcohol use among a community-based sample of gay men: Correlates of high-risk use and implications for service provision. Drug Alcohol Rev. 34, 349–57 (2015).
Bourne, A. et al. ‘Chemsex’ and harm reduction need among gay men in South London. Int. J. Drug Policy, https://doi.org/10.1016/j.drugpo.2015.07.013 (2015).
Mercer, C. H. et al. The health and well-being of men who have sex with men (MSM) in Britain: Evidence from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). BMC Public Health, https://doi.org/10.1186/s12889-016-3149-z (2016).
Race, K., Lea, T., Murphy, D. & Pienaar, K. The future of drugs: recreational drug use and sexual health among gay and other men who have sex with men, https://doi.org/10.1071/SH16080.
Mumtaz, G. R. et al. HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis. PLoS medicine, https://doi.org/10.1371/journal.pmed.1001663 (2014).
Melhem, N. M., Rahhal, N., Charide, R., Kreidieh, K. & El-Khatib, R. Human immunodeficiency virus and viral hepatitis among high-risk groups: Understanding the knowledge gap in the Middle East and North Africa Region. World Journal of Hepatology, https://doi.org/10.4254/wjh.v7.i25.2619 (2015).
Middle East and North Africa Harm Reduction Association, M. Project crossroads. Size estimation, risk behavior assessment, and disease prevalence among key populations in Lebanon (2015).
Ghosn, J., Taiwo, B., Seedat, S., Autran, B. & Katlama, C. HIV. Lancet 392, 685–697 (2018).
Arreola, S. et al. Sexual Stigma, Criminalization, Investment, and Access to HIV Services Among Men Who Have Sex with Men Worldwide. AIDS Behav. 19, 227–234 (2015).
Acknowledgements
This study has been funded by Drosos foundation and the KIP project (support of US Department of State). The sponsors did not intervene at any stage of the data collection, statistics, data interpretation, manuscript writing and publishing. The authors would like to thank the National Aids Control Program (Dr. Mostafa El Nakib) for their support in providing the HIV rapid testing kits, HIV confirmation tests and free treatment for people living with HIV in Lebanon.
Author information
Authors and Affiliations
Contributions
A.A., S.A.Z., J.N., A.G. and Z.B. performed the research. A.A., S.A.Z., J.G. and R.T. designed the research study. N.K., D.A.A. and G.A. contributed essential reagents and tools. A.A., S.A.Z., J.G. and R.T. analyzed the data. J.G., R.T. and D.A.A. edited the manuscript. A.A., S.A.Z. wrote the paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Assi, A., Abu Zaki, S., Ghosn, J. et al. Prevalence of HIV and other sexually transmitted infections and their association with sexual practices and substance use among 2238 MSM in Lebanon. Sci Rep 9, 15142 (2019). https://doi.org/10.1038/s41598-019-51688-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-51688-7
This article is cited by
-
Late presentations and missed opportunities among newly diagnosed HIV patients presenting to a specialty clinic in Lebanon
Scientific Reports (2024)
-
Sexually transmitted infections and associated risk factors among the transgender population of Pakistan
BMC Infectious Diseases (2023)
-
Facilitators and barriers to condom use in Middle East and North Africa: a systematic review
Journal of Public Health (2023)
-
Why do men who have sex with men practice condomless sex? A systematic review and meta-synthesis
BMC Infectious Diseases (2022)
-
Sociodemographic characteristics and HIV risk behaviors of native-born and displaced Syrian men and transgender women who have sex with men in Lebanon
AIDS and Behavior (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
