
Abstract
Mean birth weight of twins is known to be lower than that of singletons, however, southern China lacks a twin-specific birth weight reference. In this paper, we use data from the Birth Certificate System in southern China, collected between January 1st 2014 and December 31st 2017 and including 161,076 twins, to calculate sex- and gestational week-specific birth weight percentiles (the 3rd, 10th, 25th, 50th, 75th, 90th, and 97th). We applied generalized additive models for location, scale and shape (GAMLSS) when calculating the birth weight percentiles, and calculated percentiles for monochorionic and dichorionic twins separately. We next used data collected between Jan 1st 2018 and Apr 30th 2018, encompassing 12,371 live births, to calculate the SGA and LGA ratios using birth weight references in Australia, South Korea and China (based on birth defects surveillance system) and birth weight percentiles calculated in this study. Compared to dichorionic twins, monochorionic twins had lower birth weights at 25 to 42 weeks of gestation. The calculated SGA and LGA ratios were relatively stable compared to the other references.
Similar content being viewed by others
Introduction
In recent years, due to the development of assisted reproductive technologies, the twin pregnancy rate continues to rise1. Twins have higher risks of preterm birth, perinatal morbidity and mortality2. Twins account for 2–4% of all infants, and the problems associated with twin pregnancies have attracted increased global attention. According to a report from the National Health and Planning Commission in China, the twin pregnancy rate increased by 4.1% in 20163. Chorionicity complicates twin health further. The risk of adverse pregnancy outcomes (e.g. congenital anomalies, growth restrictions, perinatal death) and complications of fetus during pregnancy (e.g. twin-to-twin transfusion syndrome) is higher among monochorionic twins than among dichoroitic twins4. Therefore, chorionicity must be taken into account when establishing birth weight references for twins.
Birth weight is still the most commonly used indicator of fetal development. Infants are commonly defined as SGA or LGA if their birth weight percentile falls below the 10th percentile or above the 90th percentile of the reference standard5,6. SGA and LGA are associated with increased perinatal and infant mortality and morbidity, as well as long-term health problems. Twin birth weights were consistently lower than those of singletons7. In addition, multiple pregnancies are a risk factor associated with SGA8. Therefore, proper use of birth weights reference percentiles to classify birth weight is of great significance for clinical work and research.
Several countries, including Japan, Australia, South Korea, south India, Norway and the United States of America have developed population-based twin birth weight references to assist in accurately evaluating the growth of twins7,9,10,11,12,13. Findings in these countries have demonstrated the importance of the development of national birth weight standards for twins. Researchers have suggested that gestational age-specific birth weight reference percentiles should be updated every 5–10 years1. However, there is still no reference standard for twin birth weights in southern China.
The current study aims to construct the sex- and gestational age (week)-specific birth weight reference percentiles for twins born in southern China, stratified by placental chorionicity (monochorionic and dichorionic placentation).
Materials and Methods
All birth data were obtained from the Guangdong Provincial Birth Certificate System between Jan 1st, 2014 and Dec 31st, 2017. The system covers more than 1900 medical institutions and collects all information about mothers and infants. After birth, maternity medical workers place newborn infants on electronic scales to obtain stable weight data (weighing accuracy is within 1 g). In some cases, health care attendants or midwives fill in the newborns’ information in the regional maternal and child information system. The system sets logic correction to ensure that the entered birth weight falls within a feasible range. Finally, regional maternal and child information are uploaded to the Guangdong Provincial Birth Certificate System. The Chief of Midwives and the Chief of Physicians in hospitals then confirm the information entered into the data system. Before the birth certificate is issued, the Department of Medical Administration and parents are also asked to confirm the birth information. All of the information is verified by medical professionals. The birth registry database includes the child’s date of birth, gestational age (week) at birth, birth weight, infant sex, parents’ ages, registered residence, method of delivery and placenta chorionicity, etc. From the database, we obtained 161,134 cases of twins. We excluded stillbirths (48 cases) and deaths within seven days (10 cases), which together accounted for about 0.04% (58 cases) in all twins. The final analytical sample included 161,076 twin births. Because this study is based on administrative data collected from a large population, it was not possible to obtain informed consents; however, the study was reviewed and approved by the Ethics Committee of Guangdong Women and Children Hospital.
We analyzed the raw data of all twin newborns (40,090 in 2014, 38,285 in 2015, 42,241 in 2016 and 40,460 in 2017). The gestational age (week) was determined by combining mother-reported last menstrual period, ultrasound examination, and postnatal gestational age (week) assessment. The chorionicity of the placenta was judged by ultrasound data collected during the first trimester (about 6~7 weeks of gestation) and confirmed by data collected during examination of the placenta after birth.
Birth weight percentiles were created by using the Lambda Mu Sigma (LMS) method, which were fit using the GAMLSS package, based on the assumption that birth weight had a Box-Cox Cole and Green (BCCG) distribution14,15. The GAMLSS method allows modeling of various kurtosis asymmetric distribution and the estimation of smooth percentiles to establish birth weight percentile curves for newborns of both genders. According to Cole’s reports16, a sample size of n >1000 is needed to use the GAMLSS technique to fit a curve. The Schwarz Bayesian criterion, which entails stricter curve smoothing, can be used to judge the pros and cons of the model, as well as to ensure the smoothness and accuracy of the model. GAMLSS is based on the LMS method with a specific distribution of (μ,σ,υ,τ). We used Box-Cox t (BCT) to model birth weight, a method that combines Box-Cox-Cole-Green (BCCG) with the Box-Cox-power-exponential (BCPE) distribution. Note that we take into account the skewness and kurtosis of the data to express the value of the predictor. In addition, we made the model residuals better modified and the shape of the curve tends to be smoother. Model selection was based on the generalized Akaike Information Standard (G-AIC). That is, we selected the model with the smallest GAIC value. The smoothed data were represented by birth weight percentile curves. The curves appeared in intervals of one gestational week. We estimated mean birth weights and corresponding standard deviations for twins at the 3rd, 5th, 10th, 25th, 50th, 75th, 90th, 95th, and 97th percentiles from 25 to 42 completed weeks based on the smoothed, estimated curves. The percentiles were estimated separately by infant sex (male and female) and by chorionicity. SGA and LGA were defined as birth weights below the 10th or above the 90th percentile values at a given sex- and gestational week, respectively.
Next, we used twin birth weight data collected between Jan 1st, 2018 and Apr 30st, 2018, encompassing 12,371 twin births, to verify the reliability of the four standards. We accomplished this by calculating the SGA ratio and the LGA ratio according to the standards’ 10th and 90th percentile values. If standards are reliable, the gestational age (week)-specific SGA and LGA ratios should fluctuate around 10%. We also compared the SGA and LGA ratios we generated to those generated using birth weight references from Australia, South Korea and China (established based on a birth defects surveillance system). Since birth weight may differ by race and ethnicity, the birth weight standards from other countries may differ from those we produced. Moreover, given that birth weights in China may have changed since the implementation of the two-child policy in China in 2016, previously produced birth weight standards in China may be outdated. In both cases, this could result in inaccuracies in the classification of infants as SGA or LGA.
The GAMLSS package (version 5.0.6) for R statistical software (version 3.4.2) was used for analysis.
Results
As showed in Table 1, a total of 83,940 pregnant women and 161,076 twin births included in analysis. Of the pregnant women, 55505 (66.2%) were 25 to 34 years-old and 2.0% were above age 40; 79,716 (95.0%) mothers were members of the Han ethnic group and 61,768 (73.6%) mothers were multipara. Vaginal delivery and cesarean section delivery accounted for 18.6% and 59.2% of all births respectively, while the remaining delivery modes were unclear. Of the twin births, 84,208 (52.3%) were male twins and 76868 (47.7%) were female twins. Of the 98,111 twin births which chorionic placentation were known, 34,338 were monochorionic male twins, 31,567 were monochorionic female twins, 16,720 were dichorionic male twins and 15,486 were dichorionic female twins. The mean birth weights and associated standard deviations (SD) for male twins with monochorionic and dichorionic placentation were (2436 ± 453) g and (2506 ± 480) g, respectively. While the mean birth weights and associated standard deviations (SD) of female twins with monochorionic and dichorionic placentation were (2361 ± 423) g and (2400 ± 459) g, respectively. Premature twins born at 28–36 weeks and term twins born at ≥37 weeks accounted for 45.9% and 53.7% of all twins, respectively. Low birth weight twin births (birth weight <2500 g) and normal birth weight twin births (birth weight ≥2500 g) accounted for 52.2% and 47.8% of all twins, respectively.
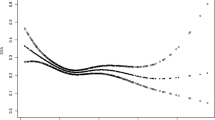
Table 2 displays smoothed percentiles for birth weights by gestational age (week) for male and female twins. We next grouped all monochorionic twins based on gestational age (week) and present the resulting data at the 3rd,10th,25th,50th,75th,90th, and 97th percentiles in Table 3. Dichorionic twins were plotted in the same way, with Table 4 displaying smoothed percentiles for birth weights (in grams) of dichorionic male twins and dichorionic female twins. As the gestational age (week) increases, the growth curves for various percentiles become smoother and increasingly steadily. In the 10th, 50th, and 90th percentile graphs of monochorionic twins and dichorionic twins, male twins showed higher BWs than females in the total infant graphs at each GA. Twins showed the most weight gain at 34–35 weeks, with growth slowing after 38 weeks (Fig. 1). Table 4 provides the sex-specific proportions of births at 25–42 gestational weeks.

Smoothed percentiles of birth weight (gms) by gestational weeks for: (A) overall male twins; (B) overall female twins; (C) monochorionic male twins; (D) monochorionic female twins; (E) dichorionic male twins; and (F) dichorionic female twins.
Table 5 provides the SGA and LGA ratios of four standards. The curves showing the incidence of SGA at different gestational ages were used to produce criteria, which were then compared to the previous criteria in China, as well as the criteria from Australia and South Korea (Fig. 2). Since Australia and South Korea’s standards only cover gestational ages ranging from 25–40 weeks, we only use these references to calculate SGA and LGA at 25–40 weeks. Moreover, the China birth defects surveillance system standards only cover gestational ages between 28–42 weeks. As a result, we only use this reference to calculate SGA and LGA at 28–42 weeks. As expected, the thresholds derived from Australia standards captured a greater proportion of SGA births (45.9%) in 40 gestational age (week), while included only 4.1% in 28 gestational age (week) among the gestation ranges in their research dataset. On the other hand, the thresholds derived from South Korea standards below the 10th and above the 90th percentile across all gestational age (week) categories were from 3.3% to 37.9%. The thresholds derived from China birth defects surveillance system standards captured a greater proportion of LGA births (46.7% in 41 gestational age (week)), while included only 6.7% (40 gestational age (week)) within the gestation ranges in their research dataset. In our research, the 10th and 90th-percentile proportions of birth weight for gestational week which got by Birth weight percentiles of southern China were relatively stable. The maximum value was found in SGA of 27 and 41 gestational age (week) (13.3%), while the minimum value is found in LGA of 27 gestational age (week) (6.7%).

Comparison with the birth weight references in Australia, South Korea, and China (based on the birth defects surveillance system standards). (A) At each gestational age (week), the SGA rate is calculated by dividing the number of twins who are defined as SGA by the total number of twins born during this gestational age (week). (B) Appropriate for gestational age (AGA) twins were defined as those with birth weights falling within the 10th and 90th percentiles. The AGA rate is calculated by dividing the number of twins who are defined as AGA by the total number of twins born during the gestational age (week) (C) The LGA rate is calculated by dividing the number of twins who are defined as LGA by the total number of twins born during the gestational age (week).
Discussion
In this study, we constructed new birth weight percentage curves for twins born in southern China. We have estimated percentage curves separately by chorionicity in order to account for chorionic membranes during twin births. Our comparison of percentile curves by chorionicity showed that birth weights of dichorionic twins were higher than monochorionic twins at 25 to 42 weeks of gestation. This finding is consistent with research conducted in south India and the US7,17. The low birth weight of monochorinic twins can be attributed to a reduction in weight due to a shared placenta, as well as to reduce effectiveness of the placenta18.
The average birth weight of male infants is greater than that of female infants for both monochorionic twins and dichorionic twins. The overall pattern of change in birth weight over gestational age is characterized by a rapid increase in birth weight up until week 37, followed by a reduced rate of change afterward. Both male and female infants grew at the fastest rate between 34 and 35 weeks, gaining an average of 192 g and 182 g per week, respectively. Studies of twin pregnancies in the US have found that twin infants have the fastest weight gain between 32 weeks and 34 weeks17, while the East Flanders Prospective Twin Survey (EFPTS) found that the most rapid period of infant weight gain occurred between 32 weeks and 34 weeks, with 156 g gained per week19.
Because of improvement in medical care facilities and nutrition in China, the proportion of twins with fetal growth restriction has declined, while perinatal survival has improved. Furthermore, due to the large sample size used in our analysis, the birth weight standard we have produced can shed new light on the current situation of twins in southern China.
According to the twin birth weight standard we have constructed for southern China, the highest prevalence (13.3%) of SGA was observed at 41 weeks of gestation, while the lowest (9.1%) was observed at 26 weeks of gestation. Relative to the other three standards, our standard led to a more stable estimate of the prevalence of LGA, which ranged from 6.7% to 11.5%. If we were to instead use one of the other three standards, we would likely misclassify SGA and LGA across all gestational age groups. In particular, the other standards lead to very different estimates of the SGA rate between 39 and 40 weeks of gestation. Compared to southern China’s twin birth weight standard, a smaller number of twins were classified as LGA by the Australian and Korean standards. However, a larger number of twins were defined as LGA if we were to use the Chinese standard (based on birth defects surveillance system). This suggests that twin growth standards for healthy twins developed in other countries are not applicable to the population of southern China. Moreover, it is important to regularly update the reference, in order to identify changes in birth weight distributions of twins over time. In addition, previous research has suggested that chrionicity should be taken into account when assessing twin fetal development17. In particular, fetal growth appears to differ for twins with monochorionic and dichorionic placentation. Until now, classification of chorionicity was not established for twin birth weight standards in southern China.
Due to the lack of appropriate reference tools, birth weight percentiles for singletons are commonly used in clinical practice in China. In this study, the use of a large, nationally representative population-based sample of twins ensures a more representative and accurate estimate of percentiles.
Unfortunately, we did not collect data on environmental factors that may have affected the pregnant women and fetuses in the study, including socio-economic conditions, diet or nutritional status. Therefore, we cannot directly analyze the relationship between environmental factors and birth weight distributions. Secondly, as with other population-based studies, our data are based on birth registry data, rather than longitudinal measurement of the development of the same fetuses over the course of pregnancy. That is, we have not measured in utero fetal growth. Birth weight percentiles are not the same as intrauterine growth percentiles in that birth weight percentiles do not reflect fetal growth but rather size at birth. The birth weight of premature babies may be affected by the pathological process leading to premature birth and the developmental status during the period of extrauterine growth to full term may be different from that of intrauterine growth until full term20,21. It has been suggested that preterm births should be assessed using estimated utero fetal growth trajectories rather than birth weight percentile, given that preterm neonates are likely affected by fetal growth restriction20. However, it is difficult to estimate utero fetal growth weight, due to challenges in obtaining accurate measurements, including estimates for fetal weight calculations and the formulas needed for the calculations21.
References
Zhang, B. et al. Birth weight percentiles for twin birth neonates by gestational age in China. Sci rep-uk 6(1), https://doi.org/10.1038/srep31290 (2016).
Cheong-See, F. et al. Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis. BMJ 354, i4353 (2016).
Team, N. H. A. F., Limei, J., Shanshan, L., Caixia, L. & Chong, Q. Ultrasound Examination of Twin Pregnancy Technical Specifications (2017). Chinese Journal of Practical Gynecology and Obstetrics 08, 815–818 (2017).
Sherer, D. M. Adverse perinatal outcome of twin pregnancies according to chorionicity: review of the literature. Am J Perinatol 18(1), 23–37 (2001).
Saenger, P., Czernichow, P., Hughes, I. & Reiter, E. O. Small for gestational age: short stature and beyond. Endocr rev 28(2), 219 (2007).
Weight, B. Large for Gestational Age. (Alphascript Publishing, 2010).
Premkumar, P. et al. Birth weight centiles by gestational age for twins born in south India. Bmc pregnancy childb 16(1), https://doi.org/10.1186/s12884-016-0850-y (2016).
Lipecka-Kidawska, E., Gottwald, L. & Niewiadomska-Jarosik, K. Intrauterine growth restriction. Int J Gynaecol Obstet 62(7), 713 (2005).
Kato, N. & Uchiyama, Y. Reference birth-length range for multiple-birth neonates in Japan. J Obstet Gynaecol Res 31(1), 43–49, https://doi.org/10.1111/j.1447-0756.2005.00248.x (2005).
Li, Z., Umstad, M. P., Hilder, L., Xu, F. & Sullivan, E. A. Australian national birth weight percentiles by sex and gestational age for twins, 2001–2010. Bmc pediatr 15, 148, https://doi.org/10.1186/s12887-015-0464-y (2015).
Lim, J. S. et al. New Korean reference for birth weight by gestational age and sex: data from the Korean Statistical Information Service (2008–2012). Annals of Pediatric Endocrinology & Metabolism 19(3), 146, https://doi.org/10.6065/apem.2014.19.3.146 (2014).
Glinianaia, S. V., Skjaerven, R. & Magnus, P. Birth weight percentiles by gestational age in multiple births. A population-based study of Norwegian twins and triplets. Acta Obstet Gynecol Scand 79(6), 450–458 (2000).
Mikolajczyk, R. T. et al. A global reference for fetal-weight and birth weight percentiles. Lancet 377(9780), 1855–1861, https://doi.org/10.1016/S0140-6736(11)60364-4 (2011).
Platt, R. W. et al. Detecting and eliminating erroneous gestational ages: a normal mixture model. Stat med 20(23), 3491–3503 (2001).
Mikis D. S., Robert A. R., Gillian Z. H., V. V. & B. F. D. Centile estimation in Flexible Regression and Smoothing Using GAMLSS in R. 449–480 (Chapman & Hall/CRC, 2017).
Cole, T. J. et al. Age- and size-related reference ranges: a case study of spirometry through childhood and adulthood. Stat med 28(5), 880–898, https://doi.org/10.1002/sim.3504 (2009).
Ananth, C. V., Vintzileos, A. M., Shen-Schwarz, S., Smulian, J. C. & Lai, Y. L. Standards of birth weight in twin gestations stratified by placental chorionicity. Obstet gynecol 91(6), 917–924 (1998).
Ramos-Arroyo, M. A., Ulbright, T. M., Yu, P. L. & Christian, J. C. Twin study: relationship between birth weight, zygosity, placentation, and pathologic placental changes. Acta Genet Med Gemellol (Roma) 37(3-4), 229–238 (1988).
Loos, R. J. et al. Determinants of birth weight and intrauterine growth in liveborn twins. Paediatric & Perinatal Epidemiology, 19(s1), 15–22 (2005).
Cooke, R. W. Conventional birth weight standards obscure fetal growth restriction in preterm infants. Arch Dis Child Fetal Neonatal Ed 92(3), F189–F192, https://doi.org/10.1136/adc.2005.089698 (2007).
Ehrenkranz, R. A. Estimated fetal weights versus birth weights: should the reference intrauterine growth curves based on birth weights be retired? Arch Dis Child Fetal Neonatal Ed 92(3), F161–F162, https://doi.org/10.1136/adc.2006.109439 (2007).
Author information
Authors and Affiliations
Contributions
Professor Zhao and Bing Li devised the idea, conceptualization, and design of the study. Moreover, they developed the data collection instruments, coordinated and supervised data collection, provided comments on the manuscript, and approved the final manuscript for submission. Huazhang Miao carried out data processing and analysis, drafted the initial manuscript, and approved the final manuscript for submission. Fei Yao, Yuntao Wu, Xiu Zhang and Rubi He participated in data collection, carried out initial analyses and revised the manuscript. In addition to their other contributions to the project, Professor Zhao and Bing Li assisted in data processing and model construction. All authors have reviewed and approved the current manuscript for submission. Special thanks to Dr. Natalie Young for helping us to revise the language of manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Miao, H., Yao, F., Wu, Y. et al. Birth weight percentiles by sex and gestational age for twins born in southern China. Sci Rep 9, 757 (2019). https://doi.org/10.1038/s41598-018-36758-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-36758-6
This article is cited by
-
Should singleton birth weight standards be applied to identify small-for-gestational age twins?: analysis of a retrospective cohort study
BMC Pregnancy and Childbirth (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
