
Abstract
The aim of current study was to assess the effectiveness of losartan 50 mg in reducing blood pressure among post-dialysis euvolemic hypertensive patients, observing their survival trends and adverse events during the course of study. A multicentre, prospective, randomised, single-blind trial was conducted to assess the effect of losartan 50 mg every other day (EOD), once a morning (OM) among post-dialysis euvolemic hypertensive patients. Post-dialysis euvolemic assessment was done by a body composition monitor (BCM). Covariate Adaptive Randomization was used for allocation of participants to the standard or intervention arm. Of the total 229 patients, 96 (41.9%) were identified as post-dialysis euvolemic hypertensive. Final samples of 88 (40.1%) patients were randomized into standard and intervention arms. After follow-up of 12 months’ pre-dialysis systolic (p < 0.001) and diastolic (p 0.01), intradialysis diastolic (p 0.02), post-dialysis systolic (p < 0.001) and diastolic (p < 0.001) blood pressure was reduced from the baseline among intervention-arm patients Compared to only pre-dialysis systolic blood pressure (p 0.003) among standard arm patients after 12 months of follow. Total of six deaths were reported among standard-arm patients compared to 2 deaths among the intervention arm. Losartan 50 mg achieve an overall significant decline in blood pressure among post-dialysis euvolemic hypertensive patients.
Similar content being viewed by others


Introduction
The risk of mortality among end-stage renal disease (ESRD) patients receiving haemodialysis is 100 times greater than for the general population1. Every year, between 10–20% of patients on haemodialysis die, 45% of these deaths are attributed to cardiovascular events2. Net cardiovascular events in haemodialysis patients are multi-factorial, but elevated blood pressure in particular has a profound effect3. As the role of the kidney is impaired in end-stage renal disease patients, chronic volume overload of the renin-angiotensin-aldosterone system (RAAS), increased sympathetic activity and several other factors contribute to elevated blood pressure among haemodialysis patients. Despite known etiological causes, prevalence of hypertension among haemodialysis patients ranges between 60–80%4.
Exchangeable sodium, plasma volume and plasma-renin activity are almost twice as high in hypertensive haemodialysis patients as normotensive patients and are directly correlated with mean blood pressure5,6. This suggests that plasma volume and plasma-renin activity are two major factors contributing to hypertension among haemodialysis patients. A study on haemodialysis patients looking into response in RAAS with change in volume reported that patients with high plasma-renin activity before saline loading had an increase in blood pressure compared to normal or low plasma-renin activity7. Other studies have reported blood pressure to be more volume-dependent among haemolysis patients8. Textor et al. took this concept further and identified two groups of hypertensive haemodialysis patients: as volume-dependent and renin-dependent9.
Volume-dependent hypertensive haemodialysis patients can be managed by appropriate fluid removal. This is done by identifying the correct dry weight and extracting fluid accordingly. A body composition monitor (BCM) allows quantifiable analysis of excess extracellular volume through a comparison with a healthy population, thereby providing a reliable account of a patient’s dry weight and hydration status10. However, despite a reliable estimation of dry weight, and attaining post-dialysis euvolemic state, a group of patients are still hypertensive11,12, because of RAAS and are known as renin-dependent hypertensive patients9.
The current study was an attempt to analyse both concepts simultaneously, i.e accurately identifying patients’ dry weight, achieving euvolemic state post-dialysis, and treating post-dialysis euvolemic-but-hypertensive patients with an RAAS inhibitor. Thus the aim of current study was to assess the effectiveness of Losartan (ARB) in reducing blood pressure among post-dialysis euvolemic patients and assessing their survival trends.
Method
The study protocol with complete research design has been published12. The study was a multicentre, prospective, randomised, parallel design, single-blind trial. The Hospital Universiti Sains Malaysia (HUSM) in Kelantan and its associated dialysis centres were the main research site. The study protocols were approved by the ethical and research committee of Universiti Sains Malaysia (USM/JEPeM/15050173), and the trial was registered under Australian New Zealand Clinical Trials Registry (ACTRN12615001322527, registered 02/12/2015). The study protocols met consolidated standard of reporting trials (CONSORT) guidelines. All study procedures were in accordance with clinical practice guidelines for haemodialysis from National Kidney Foundation Kidney Disease Outcome Quality Initiative (NKF KDOQI)13. The study purpose was explained and informed consent was obtained before enrolling study participants.
Study participants
Post-dialysis euvolemic patients with systolic blood pressure >140 mmHg post-dialysis, patients aged 30–80, patients undergoing dialysis for of at least 12 months, and patients willing to participate were included in the trial. Patients with amputations, pre-existing heart disease, neoplasm and cystic kidneys, patients treated with ARBs and patients with symptomatic, predialytic hypotension (SBP less than 110 mm Hg) or high blood pressure >200/100 mmHg were excluded from the study.
Study procedure
A body composition monitor device (BCM) made by Fresenius (BCM 4BJA3641) was used for assessing the volume status of patients at the end of a dialysis session and was also used for estimating patients’ dry weight10,14. After assessing dry weight, all efforts were made to ensure patients achieved their dry weight at the end of the dialysis sessions. Patients with systolic blood pressure >140/90 mmHg thirty minutes after the dialysis sessions underwent a volume assessment by a BCM device. The blood pressure (BP) readings were taken at sitting position by a haemodialysis staff nurse using a manually calibrated sphygmomanometer. Post-dialysis hypertensive patients (>140/90 mmHg) found euvolemic in three consecutive dialysis sessions were included in the trial. In addition, a regular BCM assessment for dry weight was done to ensure patients attained their specific dry weights and euvolemic states. Literature suggests that systolic blood pressure is constantly associated with cardiovascular adverse events12,15, which is why systolic blood pressure was considered as a marker for outcomes in the current trial.
Randomization of study participants
Covariate-adaptive randomization was used for assigning all pre-screened participants who agreed to participate in the study to the intervention or standard arms16. On the basis of pre-existing literature, the covariates considered for the current study were age, gender, diabetes, and year of dialysis. All participants were randomized using covariate-adaptive randomization to prevent any influence of covariates on randomization17. Randomization of study participants was done by a computer program to minimize the risk of selection bias and avoid any influence of the researcher, the prescriber or the participant in the selection of group or medication18. Furthermore, all enrolled patients underwent a minimum two-week wash-out period to avoid any bias in the study.
Rationale for intervention
An observational study suggests that an ARB in combination with other antihypertensive medication (but not an ACEI) may have a beneficial effect on cardiovascular mortality among ESRD patients on dialysis by reducing blood pressure19. Based on cost-effectiveness and availability, and the opinion of a panel of experts, a decision was taken to use an ARB (Losartan) for the intervention group.
Standard and intervention study arms
The standard-arm patients received antihypertensive therapy (except RAAS inhibitors) including calcium channel blockers, diuretics, alpha and beta blockers, whereas the intervention-arm patients were prescribed ARB (losartan) alone or in combination with standard antihypertensive pharmacotherapy. In both study arms, upon discussion with a panel of experts, patients were allowed multiple antihypertensive pharmacotherapies to control blood pressure when necessary, to avoid any deterioration in a patient’s health. Study intervention (losartan) and antihypertensive medication was given to the patients on a weekly basis by the principle investigator. Only the study participants were blinded during the course of study.
Study End Point
A medication dose of losartan 50 mg/day was initiated for three weeks as a test dose to note any incidence of hypotension. Upon satisfaction, patients were continued with 50 mg/day every day apart from dialysis days. A persistent > 180 mmHg post-dialysis blood pressure despite adding three hypertensive agents resulted in dose titration. The dose titration was initiated with losartan 50 mg to 100 mg followed by non-RAAS antihypertensive agents for the intervention group. For the standard group, the choice of dose titration was left to expert opinion18,20. The primary end point was achieving a post-dialysis blood pressure of <140/90 mmHg and maintaining this for four weeks, whereas the secondary end point was all causes of mortality. Figure 1 describes the study flow.

Study flow chart.
Sample size and statistical analysis
The sample size for the current study was based on a statistical superiority trial (continuous data) design of a randomized control trial21.
Calculating the sample size using the equation above:
where, N = size per group; p = the response rate of standard treatment group; z = the standard normal deviate for a one or two sided x; δ = a clinically acceptable margin; S2 = Polled standard deviation of both comparison groups The sample size calculated from statistical superiority for randomized control trials is 35 for each arm, so altogether 70 euvolemic hypertensive patients. Moreover a 25% dropout was also included, making total of 88 patients (44 in each arm).
Statistical analysis
Results were expressed as mean or percentage. Comparisons between treatment groups were made by using Wilcoxon tests after adjustment for the dynamic stratification variables (age, sex, years on dialysis, and diabetes). Cohen’s d test was applied to note the effect size. In addition, linear regression was applied to note any influence of patient characteristics on treatment outcome. This data is presented as hazard ratios and 95% confidence intervals. Statistical significance was set at P less than 0.05.
At the end of patient follow-up, both arms underwent survival analysis. Note that the patients that were dropouts/withdrew or transferred from the study could not be followed up. However, their final status at the end of patient follow-up was tracked. At the end of the trial, all transferred and withdrawn cases were alive and hence were categorised as living. Kaplan-Meier analyses were used for survival analysis after 12 months of patient follow-up. For this purpose, patient demographics and characteristics were analysed against patient status at the end of the trial through Kaplan-Meier analysis. All statistical calculations were performed using SPSS version 20.
Results
A total of 229 haemodialysis patients underwent post-dialysis BCM analysis: 130 (56.8%) male and 99 (43.2%) female patients. The mean age of haemodialysis patients was 55.98 (SD ± 12) years. Since the study was carried out in the Malaysian state of Kelantan, the overwhelming majority of patients were of Malay ethnicity (n = 228, 99.6%). Of the total 229 patients, 113 (49.3%) had completed primary education and 117 (51.1%) were urban residents. 98 patients (42.8%) were categorised as normal weight, and 86 as overweight (37.6%), according to BMI classification. Thirty six (15.7%) patients were smokers and 2 (0.9%) patients were alcoholic. The largest number of patients (n = 89, 38.9%) were on dialysis for 2–3 years, followed by 1–2 years (n = 53, 23.1%), 3–4 years (n = 44, 19.4%), >5 years (n = 25, 10.9%) and 4–5 years on dialysis (n = 18, 7.9%). Hypertension (n = 186, 81.2%), anaemia (n = 176, 76.9%) and diabetes (n = 144, 62.9%) were the most common comorbidities among haemodialysis patients. A calcium channel blocker was the most prescribed antihypertensive among patients (n = 153, 66.8%) followed by a diuretic (n = 131, 62.9%) (Table 1).
Of the total 229 haemodialysis patients, 48 (21%) were classified as post-dialysis hypervolemic, 37 (16.2%) were post-dialysis hypervolemic and 144 (62.9%) were post-dialysis euvolemic, according to post-dialysis BCM analysis. Furthermore, post-dialysis euvolemic patients (n = 144, 62.9%) were further classified with respect to their post-dialysis blood pressure. A total of 43 (18.8%) patients were euvolemic normotensive, 5 (2.2%) patients were euvolemic hypotensive whereas 96 (41.6) patients were classified as euvolemic hypertensive (Fig. 2).

Selection of euvolemic hypertensive patients.
Of the total 96 post-dialysis euvolemic patients, 8 (8.3%) patients experienced blood pressure variations and were thus dropped from the study. Altogether, final samples of 88 post-dialysis euvolemic patients were equally randomized into the standard and intervention arms. Twenty one (47.7%) male patients were randomized to the standard arm whereas 24 (54.5%) male patients were randomized to the intervention arm. Similarly, 23 (52.3%) female patients were randomized to the standard arm compared to 20 (45.4%) females in the intervention arm. The mean age of study participants was also comparable in the standard (54 ± 10.2 years) and intervention arms (53.7 ± 10.8 years). Thirty one (70.5%) diabetic patients were randomized to the standard arm, compared to 28 (63.6%) diabetic patients in the intervention arm. A calcium channel blocker was the most prescribed antihypertensive drug in both the study arms (standard n = 37, 84.1%; intervention = 32, 72.7%) (Table 2).
Baseline pre-dialysis blood pressure among standard-arm patients was 167.5 mmHg (SD ± 18.2), which at the end of the 12-month follow-up was reduced to 162.4 mmHg (SD ± 10.2), giving a difference of 5.1 mmHg. This drop in pre-dialysis systolic blood pressure was statistically significant (Cohen’s d = 0.54, p 0.003). Whereas baseline pre-dialysis systolic blood pressure in the intervention arm was 168.65 mmHg (SD ± 16.33), at the end of the 12-month follow-up it was reported as 158.45(SD ± 10.65), giving a difference of −10.23 mmHg. Statistical analysis suggests a significant decline in pre-dialysis systolic blood pressure (p < 0.001) with a large effect size (Cohen’s d 0.94).
Post-dialysis systolic blood pressure among standard-arm patients was 157.5 (±14.3) mmHg, which at the end of the 12-month follow-up was reduced to 156.8 (±11.3) mmHg, giving a difference of 0.7 mmHg. This reduction is post-dialysis blood pressure was statistically non-significant (Cohen’s d 0.17, p 0.42) compared to baseline post-dialysis blood pressure that was 156.34 (SD ± 13.40) and at the end of the 12-month follow-up was 149.73 (SD ± 10.21), so a difference of 6.6 mmHg. This decline in post-dialysis systolic blood pressure was statistically significant (p < 0.001) with a large effect size (Cohen’s d 1.19) among intervention-arm patients (Table 3).
Simple linear regression was applied for factors related to post-dialysis systolic blood pressure among both standard- and intervention-arm study participants. Analysis suggests that diabetes (standard p 0.03, intervention p 0.02) was related to post-dialysis systolic blood pressure among both study arm patients. Diabetes and ex-smokers (p 0.04) were statistically associated with post-dialysis blood pressure among standard arm patients. Similarly, male gender (p 0.02), patients that never smoked (0.04) and patients that were on diuretics (p 0.03) were statistically associated with post-dialysis blood pressure among intervention-arm patients (Table 4).
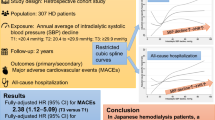
A total of 6 (13.6%) deaths were reported among patients in the standard arm compared to 2 (4.5%) deaths in the intervention arm. The probability of survival of standard-arm patients after 12 months of follow-up was 84% compared to 95% for intervention-arm patients (Fig. 3) However, Kaplan–Meier analysis indicates no significant difference in survival among patients in the standard or treatment arms. The majority of deaths were reported among male patients (n = 6, 13.6%) compared to 2 (4.5%) deaths among female patients. The probability of 1-year survival of men was 84% compared to 95% for women (Fig. 4). However, Kaplan-Meier analysis indicates no statistical difference in the survival of male and female study participants (Table 5).

Study arm based survival analysis of study subjects.

Gender based survival analysis of study subjects.
Adverse events were classified according to K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease. 2 patients in the intervention arm, so receiving losartan, suffered from mild hyperkalemia, as confirmed by the Naranjo scale. Similarly, 4 coughing, 3 dizziness and 1 dyspepsia cases were confirmed from Naranjo scale assessment (Table 6).
Discussion
The analysis of the current study suggests that blood volume and RAAS are two of the main factors contributing to hypertension among haemodialysis patients. Identifying, attaining ideal dry weight, and treating patients with RAAS inhibitors helps in reducing blood pressure significantly compared to non-RAAS antihypertensive therapy. The study findings are in line with preliminary findings that suggest that after 8 weeks of patient follow-up, intervention-arm patients were able to achieve a drop of 2.4 mmHg in post-dialysis systolic blood pressure compared to those in the standard arm (0.3 mmHg post-dialysis systolic blood pressure)22. After 12 months of patient follow-up, losartan 50 mg was able to achieve a difference of 6.6/6.9 mmHg from baseline post-dialysis blood pressure. Our analysis suggests this drop in post-dialyses blood pressure was significantly different (post-dialysis systolic blood pressure Cohen’s d 1.19, p < 0.001) from baseline and as compared to standard-arm patients that were treated with non-RAAS therapy (post-dialysis systolic Cohen’s d 0.17, p 0.42).
Not only was losartan 50 mg (OD) able to achieve a significant decline in post-dialysis blood pressure as compared to standard-arm patients, but patients in the intervention arm also observed a significant decline in pre-dialysis systolic blood pressure (Cohen’s d 0.94, p value < 0.001), pre-dialysis diastolic blood pressure (Cohen’s d 0.45, p 0.01), and intradialysis diastolic blood pressure (Cohen’s d 0.34, p 0.023). Perhaps the most vivid explanation in support of our findings with respect to the importance of volume control and RAAS was noticed among anephric patients, where both of the kidneys have been removed. These patients have no functioning RAAS and consequently have very low levels of aldosterone in their blood. Blood pressure in these patients is entirely dependent upon volume changes and is sensitive to changes in extra-cellular volume, with no response to changes in plasma-renin activity or hypotensive response to saralasin23.
Predictors for blood-pressure control among haemodialysis patients are multi-factorial. However, our analysis suggests that diabetes was the only patient factor that affected post-dialysis systolic blood pressure among both study arms. This finding was in agreement with previous literature that reported that higher mortality rates and uncontrolled blood pressure were common in diabetic patients on haemodialysis24. Moreover, the findings of the HELD trial also reported diabetes as a common predictor (both study arms) associated with post-dialysis high blood pressure. Possible explanation for diabetes as a factor for uncontrolled blood pressure among haemodialysis patients may include: diabetic patients have more comorbidities than non-diabetics; diabetic patients may not tolerate changes in systolic blood pressure as well as patients without diabetes; diabetes is associated with the aging process and patients with diabetes of a given age may experience higher mortality rates associated with changes in systolic blood pressure compared to older patients without diabetes24. Other factors that contributed towards post-dialysis systolic blood pressure were male gender and diuretics, among intervention-arm patients, compared to ex-smokers among standard-arm patients.
RAAS inhibitors are effective in lowering blood pressure and reducing cardiac events in non-haemodialysis patients25, thereby suggesting their role in managing blood pressure among haemodialysis patients. Bilateral nephrectomy was performed in patients with high levels of renin. However, with greater understanding of the blood-pressure mechanism in these renin-dependent individuals, bilateral nephrectomy was abandoned, as drugs that block RAAS activity were effective in controlling it, including ARBs, thereby suggesting they should be used. The results of the current study are an extension of these findings26.
Another important aspect often neglected is defining an optimal blood-pressure range among haemodialysis patients. National 4 kidney foundation guidelines recommend a pre-dialysis blood pressure of <140/90 mmHg and a post-dialysis blood pressure of <130/80 mmHg as targeted BPs for haemodialysis patients. However, there are some concerns regarding the targeted blood pressures, since most of the data is largely manipulated from observational studies from non-ESRD patients. Hence, targeted blood pressures among haemodialysis patients remain unclear27. Davenport et al. reported a higher incidence of intradialytic hypotension in patients achieving post-dialysis BP targets28. In turn, intradialytic hypotension is associated with mortality29,30, thereby raising questions regarding the recommended post-dialysis blood-pressure target range. Similarly, studies indicate a U-shaped or reverse J-shaped relationship between systolic blood pressure and mortality among ESRD patients31,32. Hence, a targeted post-dialysis of <140 mmHg systolic blood pressure was adopted for the current study.
A total of 88 post-dialysis euvolemic hypertensive patients were randomized into standard and intervention arms (44 each). 36 patients in each arm completed one year of follow-up. A total of 6 deaths and 2 transfer cases were reported among standard-arm patients, compared to 2 deaths, 2 drop-outs and 4 patients reaching end points among intervention-arm patients. None of the patients in the standard arm were able to achieve the study’s primary end point (post-dialysis systolic blood pressure <140 mmHg for four weeks). The 2 drop-outs reported in the intervention arm were due to hyperkalemia (>5.5 mEq/L).
Survival analysis among standard and intervention arms suggest higher mortality rates among standard-arm patients compared to intervention-arm patients, though the results are not statistically significant. Similarly, 75% of total deaths were reported in male patients whereas 62.5% of deaths were reported in patients aged >50 years, but neither of these variables were found to be statistically significantly associated with mortality rates after 1 year of follow-up. The literature suggests that the relationship between systolic blood pressure and mortality is not uniform across all age groups among the haemodialysis population, thereby suggesting optimal BP targets with different age groups24. In our study, the majority of mortalities were reported with patients >50 years old. This may be due to the presence of accelerated arthrosclerosis, which is common among haemodialysis patients. Previous studies have demonstrated that hypertension in haemodialysis patients is associated with increased mortality among patients that survive the first three years of dialysis32,33.
ARBs are usually well-tolerated; however hyperkalemia is frequently encountered among haemodialysis patients on RAAS inhibitors. Hence potassium levels and other blood parameters were closely tracked, to avoid any unwanted events. Two cases of hyperkalemia were reported in the current study, which resulted in study drop-outs. On the contrary, none of the study participants in the HELD trials reported any incidence of hyperkalemia22. Four cases of coughing, three cases of dizziness and one case of dyspepsia were recorded during the course of the study. However, they were treated and none of participants concerned dropped out.
Limitations
A small sample size is one of the main limitations of this study. In addition, there could be some concerns about generalizing the results of this study, as the majority of participants were Malays, so the results cannot be generalized for the whole population of Malaysia. Keeping in mind the principle of genetic influence, it might be possible that other ethnic groups, i.e. Chinese or Indians, might have different outcomes to Malays. There is no consensus on an optimal blood-pressure goal among end-stage renal disease patients. Moreover, while an accurate BP measurement is fundamental to clinical practice and research, there is no consensus on which BP method is the best representation of actual blood pressure among haemodialysis patients, as studies indicate that routine pre-dialysis or post-dialysis BP readings may overestimate BP34. A further difference in measuring BP also exists, namely whether to take the BP reading in either the supine or sitting position, though the literature reported no difference between the two. In any case, there is no consensus on the optimal method of BP measurement among haemodialysis patients35.
Conclusion
The current study indicates the importance of accurate assessment of clinical dry weight and treating post-dialysis euvolemic hypertensive patients with losartan, as this resulted in a significant decline in blood pressure. Inhibition of RAAS among post-dialysis euvolemic patients not only resulted in a significant decline in overall blood pressure but also reduced mortality compared to non-RAAS antihypertensive therapy. Reduction in overall blood pressure would not only lead to an increase in overall survival rates but may also improve the quality of life among ESRD patients.
Ethical and Trial registration
The study protocols are approved from the Ethical and Research Committee of the Universiti Sains Malaysia (USM/JEPeM/15050173). The trial is registered under the Australia New Zealand Clinical Trial Registry (ACTRN12615001322527). The trial was registered on 2/12/2015 and the first patient was enrolled on 10/12/2015. The trial was formally initiated on 16/02/2016 and patients were followed up for 12 months.
References
Foley, R. N. et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States medicare population, 1998 to 1999. J Am Soc Nephro 6(2), 489–95 (2005).
Collins, A. J., Foley, R., Herzog, C. et al. Excerpts from the United States Renal Data System 2007 annual data report. Am J Kidney Dis 51(1 suppl 1), S1–320 (2008).
Tozawa, M., Iseki, K., Iseki, C. & Takishita, S. Pulse pressure and risk of total mortality and cardiovascular events in patients on chronic hemodialysis. Kidney Int 61(2), 717–26 (2002).
Agarwal, R. Epidemiology of interdialytic ambulatory hypertension and the role of volume excess. Am J Nephrol 34(4), 381–90 (2011).
D’Amico, M. & Locatelli, F. Hypertension in dialysis: pathophysiology and treatment. J Nephrol 15, 438–45 (2002).
Mailloux, L. U. & Haley, W. E. Hypertension in the ESRD patient: pathophysiology, therapy, outcomes and future directions. Am J Kidney Dis 32, 705–19 (1998).
Igarashi, Y., Suzuki, H., Imafuku, T. et al. Hypertension in patients on chronic hemodialysis: The role of the reninangiotensin system. Jap Circ J 51, 479–84 (1987).
Ventura, J. E. & Sposito, M. Volume sensitivity of blood pressure in end-stage renal disease. Nephrol Dial Transplant 12, 485–91 (1997).
Textor, S. C. et al. Norepinephrine and renin activity in chronic renal failure: evidence for interacting roles in haemodialysis hypertension. Hypertension 3, 294–9 (1981).
Jens, P., Helga, P., Andreas, S., Joachim, L. & Klaus, P. Evaluation of clinical dry weight assessment in haemodialysis patients using bioimpedance spectroscopy: a cross-sectional study. Nephrol Dial Transplant 25, 545–551 (2010).
Chih, Y. Y., Wu, C. Y. & Yao, P. L. Post dialysis blood pressure rise predicts long-term outcomes in chronic hemodialysis patients: a four-year prospective observational cohort study. BMC Nephrology 13, 12 (2012).
Aftab, R. A., Khan, A. H., Syed, S. S. A., Khan, T. M. & Adnan, A. S. Protocol of randomized control trial for effectiveness of angiotensin receptor blockers on blood pressure control among euvolemic hypertensive hemodialysis patients. Medicine 96(14p), e6198 (2017).
National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: update. Am J Kidney Dis 66, 884–930 (2015).
Paul, W. C., Matthias, K., Christiane, R., Wolfgang, K. & Volker, W. A new technique for establishing dry weight in hemodialysis patients via whole body bioimpedance. Kidney International 61, 2250–2258 (2002).
Feifang, H., Yanqing, H., Zhenjun, M. & William, F. R. Adaptive randomization for balancing over covariates. Wiley Interdisciplinary Reviews. Computational Statistics 6, 288–303 (2014).
Hiromichi, S. et al. Effect of Angiotensin Receptor Blockers on Cardiovascular Events in Patients Undergoing Hemodialysis: An Open-Label Randomized Controlled Trial. American Journal of Kidney Diseases 52, 501–506 (2008).
Ikeda, L. S., Harm, S. C., Arcuri, K. E., Goldberg, A. I. & Sweet, C. S. Comparative antihypertensive effects of losartan 50 mg and losartan 50 mg titrated to 100 mg in patients with essential hypertension. Blood pressure 6, 35–43 (1997).
Pamela, S. et al. Efficacy and Tolerability of Losartan in Hypertensive Patients with Renal Impairment. Hypertension 31, 684–691 (1998).
Kevin, E. C. et al. Combined Angiotensin-converting Enzyme Inhibition and Receptor Blockade Associate with Increased Risk of Cardiovascular Death in Hemodialysis Patients. Kidney Int 80, 978–985 (2011).
Minsoo, K., Brian, G. & Jae-Hyeon, P. Issues in Outcomes Research: An Overview of Randomization Techniques for Clinical Trials. Journal of Athletic Training 43, 215–221 (2008).
Baoliang, Z. How to Calculate Sample Size in Randomized Controlled Trial? Journal of Thoracic Disease. 1, 51–54 (2009).
Aftab, R. A., Khan, A. M., Adnan, A. S., Sulaiman, S. A. S. & Khan, T. M. Efficacy of Losartan in the management of Post-Dialysis Euvolemic Hypertension (HELD-Trial): A Single-Blind Randomized Control Trial. Sci Rep 6, 36592 (2016).
De Wardener, H. E., MacGregor, G. A. Blood pressure and in kidney. In: Schrier, R. W., Gottschalk, C. W. (eds.). Diseases of the Kidney. Sixth edition. New York: Little, Brown and Co, 2:1303–26 (1997)
Orrin, B. M., Christopher, A., Mark, R., Rohrscheib, K. et al. Age, Race, Diabetes, Blood Pressure, and Mortality among Hemodialysis Patients. J Am Soc Nephrol 21(11), 1970–1978 (2010).
Fliser, D., Wagner, K. K., Loos, A. et al. Chronic angiotensin II receptor blockade reduces (intra) renal vascular resistance in patients with Type 2 diabetes. J Am Soc Nephrol 4, 1135–1140 (2005).
Doulton, T. W. & MacGregor, G. A. Blood pressure in haemodialysis patients: The importance of the relationship between the renin-angiotensin-aldosterone system, salt intake and extracellular volume. JRAAS 5, 14–22 (2004).
National kidney foundation kidney disease outcome quality initiative (NKF KDOQI) Clinical Practice Guidelines for Cardiovascular Disease in Dialysis Patients Date of access 12/05/2016. Retrieved from http://www2.kidney.org/professionals/kdoqi/guidelines_cvd/guide12.htm (2005).
Davenport, A., Cox, C. & Thuraisingham, R. Achieving blood pressure targets during dialysis improves control but increases intradialytic hypotension. Kidney Int 73, 759–64 (2008).
Shoji, T. et al. Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int 66, 1212–20 (2004).
Tislér, A. et al. The effect of frequent or occasional dialysis-associated hypotension on survival of patients on maintenance haemodialysis. Nephrol Dial Transplant 18, 2601–5 (2003).
Li, Z. et al. The epidemiology of systolic blood pressure and death risk in hemodialysis patients. Am J Kidney Dis 48, 606–15 (2006).
Stidley, C. A. et al. Changing relationship of blood pressure with mortality over time among hemodialysis patients. J Am Soc Nephrol 17, 513–20 (2006).
Mazzuchi, N., Carbonell, E. & Fernandez-Cean, J. Importance of blood pressure control in hemodialysis patient survival. Kidney Int 58, 2147–2154 (2000).
Fagugli, R. M. et al. Blood pressure assessment in haemodialysis patients: comparison between pre-dialysis blood pressure and ambulatory blood pressure measurement. Nephrology 14, 283–90 (2009).
Shoji, T. et al. Hemodialysis-hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int 66, 1212–1220 (2004).
Acknowledgements
The authors would like to acknowledge the Institute of Postgraduate Studies (IPS) at the Universiti Sains Malaysia for providing a fellowship during the course of doctoral studies for Mr Raja Ahsan Aftab. The authors would also express their gratitude to the nursing staff for their contribution to the study. The current study was funded by Research University grant (RUI grant 1001/PPSP/812185) by Universiti Sains Malaysia. The source of funding had influence in the current study, with no role in its design or implementation.
Author information
Authors and Affiliations
Contributions
R.A.A. and A.H.K. have drafted the first version of the manuscript. All authors have been involved in all stages of the study design and have participated in preparing manuscript whereas submission to ethical committee was done by A.S.A. and R.A.A. R.A.A. and T.M.K. were involved in statistical analysis and interpretation. A.S.A. is the Nephrologists for his clinical expertise during the trial. S.A.S.S. critically reviewed the manuscript. All authors approved the final manuscript. Data was accessed by all the authors throughout and after the study
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aftab, R.A., Khan, A.H., Adnan, A.S. et al. Safety and Efficacy of Losartan 50 mg in Reducing Blood Pressure among Patients with Post-Dialysis Euvolemic Hypertension: A Randomized Control Trial. Sci Rep 7, 17741 (2017). https://doi.org/10.1038/s41598-017-17437-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-17437-4
This article is cited by
-
ACEi/ARBs associate with lower incidence of gastrointestinal bleeding in peritoneal dialysis patients
Clinical and Experimental Nephrology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
