
Abstract
Giant cell tumors of the distal radius are challenging for surgeons because they are associated with high recurrence rates and poor functional outcomes. Between June 2005 and October 2015, patients with primary giant cell tumors of the distal radius were recruited from seven orthopedic centers in China. The patients’ clinical features and demographic characteristics were obtained from medical records and reviewed retrospectively. Overall, 48 cases of giant cell tumors of the distal radius were assessed in this study. These patients were more likely to be between 20 and 40 years of age, to have a Campanacci grade of III, and to undergo a surgical style of resection. The prevalence of pathological fractures was 12.5% overall (20.0% in men and 4.3% in women). The prevalence of local recurrence was 30.0% overall (38.1% in men and 21.1% in women) during the average follow-up period of 62.5 months, with a pulmonary metastasis rate of 5.0%. Giant cell tumors of the distal radius were predominant in men and were more likely to recur locally than around the knee. These findings suggest that it is crucial to evaluate the optimal surgical approach for balancing local recurrence control and functional outcomes to reduce the disease burden.
Similar content being viewed by others

Introduction
Giant cell tumors (GCTs) are primary intramedullary bone tumors composed of mononuclear and giant mononuclear cells, resembling osteoclasts1. Mononuclear cells are the primary pathological feature of GCT, and they determine the biological behavior of GCTs. GCTs account for only 3–8% of primary bone tumors in Western populations, compared with 20% in Asian countries2,3,4,5,6,7,8.
GCTs most commonly occur among 20–40-year-olds and are likely to be located at many sites of body. However, they usually involve the end of a long bone, and more than half of them occur around the knee3, 4, 9,10,11,12. About 10% of GCTs undergo malignant transformation, and pulmonary metastases occur in 1% to 4% of cases13. It has been reported that the postoperative recurrence rate is 10–65%14,15,16. Previous studies have indicated that GCTs predominantly occur among women17, 18. However, some studies have shown a male predominance19,20,21,22.
The distal radius is the third most common site for GCTs to occur7, accounting for an average of 10% (8–13%) of GCT occurrences23,24,25,26,27,28. GCTs in this location are more likely to have a higher rate of local recurrence, to metastasize29, 30, and to have poor functional outcomes; thus, they are one of the most controversial bone tumors. The surgical management of GCTs of the distal radius remains controversial due to the epiphyseal nature of distal radius. However, all of the previous studies were performed in single institutions; reports on the epidemiological features of GCTs of the distal radius from multicenter studies are rare.
Thus, in this study, we aimed to assess the epidemiological and clinical characteristics of GCTs of the distal radius in China using data from the Giant Cell Tumor of China (GTOC), a synergistic, multicenter study of GCTs.
Results
Overall demographic and clinical characteristics
Of the 48 patients with GCT of the distal radius, 25 (52.1%) were men and 23 (47.9%) were women, with a male to female ratio of 1.1:1. Of these, 68.8% of cases occurred in patients between 20 and 40 years of age, 79.2% were Campanacci grade III, and 66.7% were treated with resection. The prevalence of pathological fractures was 12.5% (Table 1).
Clinical characteristics by sex
Table 2 shows that the mean ages at first diagnosis of GCT of the distal radius were 30.6 years overall (28.7 years in men and 32.6 years in women). Female patients with GCT of the distal radius were more likely than men to have a GCT that was Campanacci grade III (91.3% vs. 68.0%), on the right (56.5% vs. 44.0%), and treated with resection (73.9% vs. 60.0%), although the differences between women and men did not reach statistical significance (all P > 0.05). Simultaneously, there was higher frequency in men than in women aged ≤40 years (84.0% vs. 73.9%, P = 0.487), with pathological fractures (20.0% vs. 4.3%, P = 0.191), and with dislocation (12.0% vs. 0%, P = 0.235).
Clinical characteristics by age group
There were no remarkable age differences in clinical features, but a slightly higher frequency of GCTs occurred in patients >40 years of age than in patients ≤40 years of age for Campanacci grade III (100% vs. 73%) and pathological fractures (18.2% vs. 10.8%). Conversely, patients ≤40 years of age were more likely than patients aged >40 to have a dislocation (18.1% vs. 0; Table 3).
Recurrence and metastasis
During a median follow-up period of 62.5 months, 12 patients out of 40 who were qualified for follow-up developed a local recurrence, for a rate of 30% overall. The frequency of local recurrence was 38.1% for men and 21.1% for women. Moreover, pulmonary metastasis was observed in two cases (1 man and 1 woman), for an overall rate of 5.0% (4.8% in men and 5.3% in women).
Discussion
This is the first large-sample report of the epidemiological and clinical features of patients with GCT of the distal radius from a multicenter study in China.
GCTs of the distal radius have been established to be the most common type of GCT after that of the distal femur and of the proximal tibia7, 31, 32. A female predominance for GCTs of the distal radius has been reported in previous studies33,34,35; a male-to-female ratio of 0.4:1 was reported in Iran33, of 0.7:1 in Beijing, China34, and of 0.5:1 in Hong Kong, China35. However, an inverse male predominance for GCTs of the distal radius has been observed in other studies, with reported ratios of 1.3:136 and 1.4:137. Consistent with these studies, we found a male predominance in GCT of the distal radius, with a male-to-female ratio of 1.1:1 in this study.
GCTs usually occur in young adults aged 20–40 years, accounting for 70–80% of all GCT patients. The mean age at diagnosis of GCT has been presented as being between 29 years and 40 years33,34,35,36,37,38,39,40. In the present study, 68.8% of patients with primary GCTs of the distal radius were diagnosed between 20 and 40 years of age (68.0% in men and 69.6% in women). Furthermore, a slightly younger age at diagnosis for GCTs of the distal radius was observed in men than in women, with a mean age at diagnosis of 28.7 years for men and of 32.6 years for women. Thus, there was a younger age at diagnosis for men among all patients with GCTs of the distal radius, but a younger age at diagnosis was previously observed in women among patients with GCT around the knee41. Thus, large, multicenter studies are necessary in order to determine the predominant age at GCT diagnosis in different locations in the future.
Previous studies indicated that there was a high frequency of Campanacci grade III among cases of GCT of the distal radius37, 40. In line with these studies, the frequency of Campanacci grade III accounted for 79.2% of cases of GCT of the distal radius in the present study, greater than that previously reported for GCT around the knee41. The delay in diagnosis due to the non-weight bearing location in the distal radius may contribute to the high frequency of Campanacci grade III occurring in GCTs of the distal radius.
Previous studies have indicated a great range for rates of local recurrence GCTs of the distal radius, with a rate of local recurrence between 25% and 89%16, 39, 42,43,44,45. In this study, we found that the prevalence of local recurrence was 30.0% overall, mildly greater in men (38.1%) than in women (21.1%).
The reported rates of pulmonary metastasis for GCTs of the distal radius have been controversial. Several studies reported that there was no pulmonary metastasis related to GCTs of the distal radius33, 46, 47, but a rate of 3% was reported in a different study37. Similar to that study, we found that the rate of pulmonary metastasis was 5.0% overall (4.8% for men and 5.3% for women). Moreover, the prevalence of pathological fractures was 12.5% in this study, and a slightly higher prevalence of fractures was observed in men (20.0%) than in women (4.3%). Compared to the reported rates for GCTs around the knee, the prevalence of fractures is lower for GCTs of the distal radius41.
There are limitations to this study. First, there may have been differences between the identification standards in radiological data and clinical staging at different institutions due to the multicenter retrospective study design. However, this limitation could be overcome by training the investigators from the seven centers. Moreover, all patients were recruited from 2005 to 2015; new techniques were not developed during this 15-year period, and the standard of diagnosis did not change. Second, the limited sample size may have been associated with error, but this could be improved by increasing the number of institutes involved in the GTOC.
Conclusions
To our knowledge, this is the first report of the epidemiological and clinical characteristics of primary GCTs of the distal radius from a multicenter study in China. Consistent with the previous studies, we found a mild male predominance, greater frequency of patients aged 20–40 years and with a Campanacci grade of III, and high rates of local recurrence and pulmonary metastasis. However, we found that there was a younger age at diagnosis for men and a lower prevalence of fracture in this study compared with similar data for GCTs around the knee reported in our previous study. These findings suggest that it is crucial to evaluate and compare the demographic and clinical features of GCT in all locations and design an individualized, optimal surgical approach that balances local recurrence and functional outcome and reduces the overall disease burden of GCTs.
Material and Methods
Patient selection
Patient selection and the study design have been described in previous studies20, 41. The GTOC team is an association of physicians from seven orthopedic oncology centers located in different regions of China. Seven centers established the GTOC in 2005. The aim of the GTOC is to standardize the diagnosis and treatment of GTCs in China. The current standardized procedure was devised by GTOC experts who considered GCTs’ pathological fractures, shifting of the articular surface, Campanacci grade, the growth level of the tumor (i.e., the tumor has grown with or without breaking through the articular surface), and tumor volume.
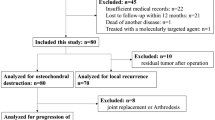
We retrospectively reviewed all qualified patients’ medical records. All patients had received their first histologically confirmed diagnoses of benign GCT and undergone surgical treatment. We excluded all patients with a preoperative diagnosis of GCT that was postoperatively determined to have been incorrect (i.e., patients with a non-GCT postoperative diagnosis). Patients who were not treated surgically did not have their diagnosis of GCT confirmed by a pathological method. Moreover, patients with recurrent GCT received treatment more than once, and the natures of the GCTs changed in these patients due to recurrence. Thus, we further excluded all cases of GCT recurrence and all patients who were not treated surgically. Clinical and imaging data of the primary GCTs in the distal radius were also reviewed retrospectively.
In total, we recruited 51 patients with primary GCTs in the distal radius and analyzed the clinical and epidemiological features of 48 cases after excluding three patients who were <13 years old. We also assessed the rate of local recurrence for 40 cases, with a response rate of 83.3%.
Campanacci grade
All patients with a GCT of the distal radius were stratified according to the Campanacci system, which is based on plain radiography48. Under the Campanacci system, grade I tumors are the least common and show features of latent or slow-growing tumors. The lesion is small, with a mild amount of sclerosis delineating the tumor. The bone contour is not affected, although the cortex can be thinned. The tumor does not extend to the articular cartilage. Symptoms are absent or minimal and of long duration. Grade II tumors show features of an active lesion with ill-defined borders and without sclerosis. The cortex is thinned, if not breached and deformed with expansion, and the periosteum is elevated. The tumor often extends to the articular cartilage from within the marrow. Grade III tumors show features of extreme aggressiveness, with a tumor that has a large volume, destroys bone, and invades the surrounding soft tissues.
Evaluation of clinical features
All patients were routinely evaluated preoperatively with plain radiography, computed tomography (CT), and magnetic resonance imaging (MRI) scans of the involved forearm and CT of the chest, after which they were all classified according to the Campanacci staging system for GCT of bone. Additionally, serum calcium, phosphorus, and alkaline phosphatase concentrations were routinely measured to rule out hyperparathyroidism. Core needle biopsies were then obtained if the lesion was atypical of GCT clinically or radiologically.
Surgical treatment
The surgical approach was chosen on the basis of the location of the tumor and the preference of the treating surgeon according to the GTOC’s predefined plan. The biopsy tract, if present, was removed in the initial incision. En bloc resection of the distal radius was then performed with a safe margin, after which the proximal fibula was excised as previously reported38, 49. The fibular graft was then placed into the forearm and fixed to the proximal radius with a compression plate or one-third tubular plate. K-wires were utilized to stabilize the newly reconstructed joints, if necessary. Next, the remnant fibular collateral ligament was sutured to the radial collateral ligaments to increase the stability of the joints.
All radiographic images of the forearm and chest were reviewed by experienced surgeons and imaging physicians to determine whether bony union, recurrence, tumor metastasis, or complications had occurred.
Denosumab was not used to treat patients postoperatively, as it was not available during the study period (2000–2014). Moreover, it has not been approved in China by the FDA. Thus, there were no additional treatments administered postoperatively.
Follow-up and outcomes
The patients were followed every 3 months for the first 2 years post-operatively, every 6 months until 5 years post-operatively, and every 12 months until 10 years post-operatively. Telephone interviews were allowed only after 5 years of follow-up. Information related to local recurrence and metastases was obtained according to the present mass by face-to-face evaluation. Patients who experienced local recurrence or metastases for which they were treated in another hospital were interviewed by telephone.
Statistical methods
All patient data were analyzed according to sex and age group. Because cases of GCT most commonly occur among patients 20–40 years old, age was categorized into two groups: ≤40 years and >40 years. Continuous variables were summarized in terms of means (standard deviations), and differences in age were compared using Student’s t-test after confirmation of normality. Categorical variables were summarized in terms of number of cases (percentages). The chi-squared test was used to compare differences in the clinical characteristics between sex and age groups. Categorical variables with <5 expected frequencies were compared using Fisher’s exact test. Statistical significance was defined as P < 0.05.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
All investigative protocols were approved by the ethics committee of Tianjin Hospital. The procedures were performed according to approved guidelines, and written informed consent was obtained from each patient.
References
Campanacci, M. Bone and soft tissue tumors: clinical features, imaging, pathology and treatment 2nd ed. New York, Springer (1999).
Ward, W. G. & Li, G. Customized treatment algorithm for giant cell tumor of bone: report of a series. Clin Orthop Relat Res. 397, 259–70 (2002).
van der Heijden, L., Dijkstra, P. D., Campanacci, D. A., Gibbons, C. L. & van de Sande, M. A. Giant cell tumor with pathologic fracture: should we curette or resect? Clin Orthop Relat Res. 471, 820–829 (2013).
Hu, Y., Chen, Y. & Lun, D. The establishing and verification of clinical scoring system for giant cell tumor. Chin J Orthopadics. 3l, 105–112 (2011).
Klenke, F. M., Wenger, D. E., Inwards, C. Y., Rose, P. S. & Sim, F. H. Giant cell tumor of bone: risk factors for recurrence. Clin Onhop Relat Res. 469, 591–599 (2011).
Tureotte, R. E. Giant cell tumor of bone. Onhop Clin Noah Am. 37, 35–51 (2006).
Niu, X. et al. Giant Cell Tumor of the Extremity: Retrospective Analysis of 621 Chinese Patients from One Institution. J Bone Joint Surg Am. 94, 461–467 (2012).
Thomas, D. M. & Skubitz, T. Giant-cell tumour of bone. Curr Opin Oncol. 21, 338–344 (2009).
von Steyern, F. V. et al. Giant-cell tumor of the knee: the condition of the cartilage after treatment by curettage and cementing. J Bone Joint Surg Br. 89, 361–365 (2007).
Puthoor, D. K. & Puthezhath, K. Management of giant cell tumor of bone: computerized tomography based selection strategy and approaching the lesion through the site of cortical break. Orthop Surg. 4, 76–82 (2012).
Ansari, M. T., Prakash, P. K. & Machhindra, M. V. Wrist preserving surgery for multifocal giant cell tumor of carpal bones in a skeletally immature patient: a case report. Orthop Surg. 6, 322–325 (2014).
Xie, M. et al. Giant cell tumor of the tendon sheath of the toe. Orthop Surg. 3, 211–215 (2012).
Dominkus, M. et al. Histologically verified lung metastases in benign giant cell tumours–14 eases from a single institution. Int Orthop. 30, 499–504 (2006).
Karpik, M. Giant cell tumor (tumor gigantocellularis, esteoclastoma): epidemiology, diagnosis, treatment. Ortop Traumatol Rehabil. 12, 207–215 (2010).
Muramatsu, K., Ihara, K. & Taguchi, T. Treatment of Giant Cell Tumor of Long Bones: Clinical Outcome and Reconstructive Strategy for Lower and Upper Limbs. Orthopedics. 32, 491–497 (2009).
Balke, M. et al. Giant cell tumor of bone: treatment and outcome of 214 cases. J Cancer Res Clin Oncol. 134, 969–978 (2008).
Unni, K. K. & Inwards, C. Y. Dahlin’s bone tumors: general aspects and data on 10,165 cases. Philadelphia, PA, Lippincott Williams & Wilkins (2009).
Dahlin, D. C. Caldwell Lecture. Giant cell tumor of bone: highlights of 407 cases. AJR Am J Roentgenol. 144, 955–960 (1985).
Marugame, T. et al. The Japan cancer surveillance report: incidence of childhood, bone, penis and testis cancers. Jpn J Clin Oncol. 37, 319–323 (2007).
Lin, F. et al. The epidemiological and clinical features of primary giant cell tumor around the knee: A report from the multicenter retrospective study in china. J Bone Oncol. 5, 38–42 (2016).
Yanagawa, T., Watanabe, H., Shinozaki, T. & Takagishi, K. Curettage of benign bone tumors without grafts gives sufficient bone strength. Acta Orthop. 80, 9–13 (2009).
Gupta, R. et al. Clinicopathologic profile of 470 giant cell tumors of bone from a cancer hospital in western India. Ann Diagn Pathol. 12, 239–248 (2008).
Campanacci, M., Baldini, N., Boriani, S. & Sudanese, A. Giant-cell tumor of bone. J Bone Joint Surg Am. 69, 106–114 (1987).
Harness, N. G. & Mankin, H. J. Giant-cell tumor of the distal forearm. J Hand Surg Am. 29, 188–193 (2004).
Khan, M. T., Gray, J. M., Carter, S. R., Grimer, R. J. & Tillman, R. M. Management of the giant-cell tumours of the distal radius. Ann R Coll Surg Engl. 86, 18–24 (2004).
McDonald, D. J., Sim, F. H., McLeod, R. A. & Dahlin, D. C. Giant-cell tumor of bone. J Bone Joint Surg Am. 68, 235–242 (1986).
Panchwagh, Y., Puri, A., Agarwal, M., Anchan, C. & Shah, M. Giant cell tumor - distal end radius: do we know the answer? Indian J Orthop. 41, 139–145 (2007).
Prosser, G. H., Baloch, K. G., Tillman, R. M., Carter, S. R. & Grimer, R. J. Does curettage without adjuvant therapy provide low recurrence rates in giant-cell tumors of bone? Clin Orthop Relat Res. 435, 211–218 (2005).
Sheth, D. S., Healey, H., Sobel, M., Lane, J. M. & Marcove, R. C. Giant cell tumor of the distal radius. J Hand Surg. 20A, 432–440 (1995).
Smith, R. J. & Mankin, H. J. Allograft replacement of the distal radius for giant cell tumor. J Hand Surg. 2A, 299–308 (1977).
Unni, K. K. & Inwards, C. Y. Dahlin’s Bone Tumors: General Aspects and Data on 10,165 Cases. Philadelphia PA, Lippincott Williams & Wilkins 225–242 (2010).
Goldenberg, R. R., Campbell, C. J. & Bonfiglio, M. Giant-cell tumor of bone. An analysis of two hundred and eighteen cases. J Bone Joint Surg Am. 52, 619–664 (1970).
Taraz-Jamshidi, M. H., Gharadaghi, M., Mazloumi, S. M., Hallaj-Moghaddam, M. & Ebrahimzadeh, M. H. Clinical outcome of en-block resection and reconstruction with nonvascularized fibular autograft for thetreatment of giant cell tumor of distal radius. J Res Med Sci. 19, 117–121 (2014).
Wang, T., Chan, C. M., Yu, F., Li, Y. & Niu, X. Dose Wrist Arthrodesis With Structural Iliac Crest Bone Graft After Wide Resection of Distal Radius Giant Cell Tumor Result in Satisfactory Function and Local Control? Clin Orthop Relat Res. 2, 1–9 (2016).
Cheng, C. Y., Shih, H. N., Hsu, K. Y. & Hsu, R. W. Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res. 383, 221–228 (2001).
Saini, R. et al. En bloc excision and autogenous fibular reconstruction for aggressive giant cell tumor of distal radius: a report of 12 cases and review of literature. J Orthop Surg Res. 6, 14 (2011).
Wysocki, R. W. et al. Is intralesional treatment of giant cell tumor of the distal radius comparable to resection with respect to localcontrol and functional outcome? Clin Orthop Relat Res. 473, 706–715 (2015).
Chadha, M., Arora, S. S., Singh, A. P., Gulati, D. & Singh, A. P. Autogenous onvascularized fibula for treatment of giant cell tumor of distal end radius. Arch Orthop Trauma Surg. 130, 1467–1463 (2010).
Kang, L., Manoso, M. W., Boland, P. J., Healey, J. H. & Athanasian, E. A. Features of grade 3 giant cell tumors of the distal radius associated with successful intralesional treatment. J Hand Surg Am. 35, 1850–1857 (2010).
Saikia, K. C. et al. Resection-reconstruction arthroplasty for giant cell tumor of distal radius. Indian J Orthop. 44, 327–332 (2010).
Hu, Y. et al. Sex Differences in the Recurrence Rate and Risk Factors for Primary Giant Cell Tumors Around the Knee in China. Sci Rep. 6, 28173 (2016).
Aithal, V. K. & Bhaskaranand, K. Reconstruction of the distal radius by fibula following excision of giant cell tumor. Int Orthop. 27, 110–113 (2003).
Minami, A., Kato, H. & Iwasaki, N. Vascularized fibular graft after excision of giant-cell tumor of the distal radius: wrist arthroplasty versus partial wrist arthrodesis. Plast Reconstr Surg. 110, 112–117 (2002).
Puri, A., Gulia, A., Agarwal, M. G. & Reddy, K. Ulnar translocation after excision of a Campanacci grade-3 giant-cell tumour of the distal radius: an effective method of reconstruction. J Bone Joint Surg Br. 92, 875–879 (2010).
Liu, Y. P., Li, K. H. & Sun, B. H. Which treatment is the best for giant cell tumors of the distal radius? A meta-analysis. Clin Orthop Relat Res. 470, 2886–2894 (2012).
Chadha, M., Arora, S. S., Singh, A. P., Gulati, D. & Singh, A. P. Autogenous non-vascularized fibula for treatment of giant cell tumor of distal end radius. Arch Orthop Trauma Surg. 130, 1467–1473 (2010).
Szabo, R. M., Anderson, K. A. & Chen, J. L. Functional outcome of en bloc excision and osteoarticular allograft replacement with the Sauve-Kapandji procedure for Campanacci grade 3 giant-cell tumor of the distal radius. J Hand Surg Am. 31, 1340–1348 (2006).
O’Donnell, R. J. et al. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg Am. 76, 1827–1833 (1994).
Lin, N., Ye, Z. M., Li, W. X., Tao, H. M. & Yang, D. S. Long-term result of fibula grafting for reconstruction of the distal radius after giant cell tumor excision. Chin J Surg. 47, 1079–1082 (2009).
Acknowledgements
We thank all the participants of this study and the local doctors for their enthusiasm, tireless work, and sustained support.
Author information
Authors and Affiliations
Contributions
H.C. was involved in the data interpretation and drafting of this manuscript. Y.H. was involved in the obtain grant, conception and design, data collection, data interpretation, and critical review of this article. F.L., L.Z., X.Y., Z.W., Z.Y., S.W., S.G., and G.Z. were involved in the data collection, case diagnosis, and approval of this article. J.W. was involved in the conception and design, data analysis, data interpretation, and critical review of this article.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cao, H., Lin, F., Hu, Y. et al. Epidemiological and Clinical Features of Primary Giant Cell Tumors of the Distal Radium: A Multicenter Retrospective Study in China. Sci Rep 7, 9067 (2017). https://doi.org/10.1038/s41598-017-09486-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-09486-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
