
Abstract
Pyrazinamide (PZA) is an important first-line drug in all existing and new tuberculosis (TB) treatment regimens. PZA-resistance in M. tuberculosis is increasing, especially among M/XDR cases. Noted issues with PZA Drug Susceptibility Testing (DST) have driven the search for alternative tests. This study provides a comprehensive assessment of PZA molecular diagnostics in M/XDR TB cases. A set of 296, mostly XDR, clinical M. tuberculosis isolates from four countries were subjected to DST for eight drugs, confirmatory Wayne’s assay, and whole-genome sequencing. Three genes implicated in PZA resistance, pncA, rpsA, and panD were investigated. Assuming all non-synonymous mutations cause resistance, we report 90% sensitivity and 65% specificity for a pncA-based molecular test. The addition of rpsA and panD potentially provides 2% increase in sensitivity. Molecular heterogeneity in pncA was associated with resistance and should be evaluated as a diagnostic tool. Mutations near the N-terminus and C-terminus of PZase were associated with East-Asian and Euro-American lineages, respectively. Finally, Euro-American isolates are most likely to have a wild-type PZase and escape molecular detection. Overall, the 8–10% resistance without markers may point to alternative mechanisms of resistance. Confirmatory mutagenesis may improve the disconcertingly low specificity but reduce sensitivity since not all mutations may cause resistance.
Similar content being viewed by others

Introduction
Pyrazinamide (PZA) is an important first-line drug recommended by the World Health Organization (WHO) for treatment of tuberculosis (TB)1. Although most patients diagnosed with TB are successfully treated with first-line drugs, rifampicin (RIF), isoniazid (INH), ethambutol, and PZA, the incidence of multidrug resistant TB (MDR-TB) (resistant to first-line drugs) is increasing every year1. Along with this rate, the incidence of PZA resistance (PZAR) is also increasing since over 60% of MDR-TB cases globally are also PZAR (rates vary regionally)2. In this manuscript we denote isolates that are resistant or susceptible to PZA by growth-based drug susceptibility testing (DST) as PZAR or PZAS, respectively.
PZA is unique among anti-TB drugs in that, while it demonstrates powerful in vivo sterilizing activity, it exhibits no activity against actively growing Mycobacterium tuberculosis bacilli under normal culture conditions at neutral pH3. The drug appears to preferentially act against non-replicating persisters with low metabolic activity at acid pH in vitro or in vivo 4.
Importantly, most new drug regimens proposed for treatment of drug-resistant TB (DR-TB) show improved outcomes when combined with PZA5,6,7,8,9. Although growth-based PZA susceptibility testing is recommended by the WHO10, the method yields inconsistent results in some cases and suffers from a relatively high false resistance rate11.
While DST is the recommended method for determining resistance to all first- and second-line drugs1, because of PZA-specific challenges, WHO is currently considering pncA-based molecular diagnostics as the recommended approach. In this study we examine the performance of such a platform in detection of PZA resistance among M/XDR TB cases from four high-TB burden countries. We also examine how the inclusion of the other two frequently discussed genes, panD and rpsA, would improve the proposed platform.
The protein commonly associated with PZA resistance is pyrazinamidase/nicotinamidase (PZase) encoded by the gene pncA 12. Mechanistically, PZA is a pro-drug that requires activation by PZase. PZase converts PZA into pyrazinoic acid (POA), where it is actively driven out of the cell, extracellularly protonated, and passively diffused back in, eventually acidifying and killing the bacterium4, 13. Hundreds of mutations distributed across pncA and its promoter have been associated with resistance, however some are also harbored by susceptible strains14, 15. This is unique since resistance to other drugs can usually be explained by a handful of mutations16,17,18. A recent systematic review estimated mutations in pncA and its promoter provide a global sensitivity and specificity of 83% and 90%, respectively14.
While changes in PZase have been associated with PZA resistance, several studies have observed PZAR isolates with a wild-type (WT) pncA 19,20,21,22,23, highlighting the need for discovery of new markers that could be used in molecular diagnostics. Recently, mutations in 30 S ribosomal protein S1 (rpsA) and aspartate 1-decarboxylase precursor (panD) have been reported to be associated with PZA resistance in M. tuberculosis 24, 25.
The gene rpsA encodes a protein involved in trans-translation, a mechanism that rescues stalled ribosomes and tags truncated proteins for degradation24. Zhang et al. demonstrated that overexpression of rpsA in M. tuberculosis confers PZA resistance in vitro 24.
The gene panD converts L-aspartate into β-alanine, a precursor in the anabolism of coenzyme A (CoA)25. Laboratory generated strains of PZAR M. tuberculosis were observed with mutations in panD, yet WT-pncA 25. However, subsequent studies have rebutted rpsA and panD as potential targets of PZA resistance26, 27.
In this study, we considered 296 mostly M/XDR-TB patients from four high-burden TB countries: India, Republic of Moldova, the Philippines, and South Africa. Unlike previous systematic reports, we have ensured standardized phenotyping for eight first and second line drugs, including PZA, using BACTEC MGIT 960 DST28. Additionally, we have performed PZase enzymatic activity testing using Wayne’s assay to confirm DST results. Genotyping was also performed via amplification-free long-read whole-genome sequencing for each isolate. Mutations in pncA, rpsA, and panD and their promoters were investigated for association to phenotypic PZA resistance.
Results
Phenotypic testing
Out of 296 mostly XDR-TB isolates (Table 1), 224 were PZAR and 72 were PZAS by DST. Two isolates were PZA mono-resistant. Table 1 also displays the prevalence of PZA resistance in all phenotypic categories.
In all, 47 (16%) strains (22 PZAR and 25 PZAS) had discordant phenotypic-genotypic results (i.e. PZAS with a mutant pncA or promoter, or PZAR with a WT pncA or promoter—Supplementary Table ST1) and underwent further enzymatic characterization.
Enzymatic activity
Overall, 103 isolates (79 PZAR and 24 PZAS), including 44 (22 PZAR and 22 PZAS) of the 47 phenotypic-genotypic discordant isolates, were tested for enzymatic activity (Table 2). Of the 103 tested isolates, five (5%) (one PZAR and four PZAS) had discordant DST and Wayne’s assay results. The DST results of 41 of the 44 phenotypic-genotypic discordant isolates were confirmed by Wayne’s assay. Only three PZAS isolates had a discordant DST and enzymatic activity results (Table 2).
Mutations in pncA of PZAR Isolates
Of the 224 PZAR isolates, 202 harbored a non-synonymous mutation in pncA and/or its promoter. Of these, 195 isolates (87%) harbored a mutation only in the gene, four (2%) only in its promoter, and 3 (1%) in both. The two PZA mono-resistant isolates belonged to the first group. Synonymous mutations in the coding region were ignored in our analyses. Those isolates that only harbored a synonymous mutation in a gene were labeled as having a WT protein in this study. Supplementary Table ST2 provides a comprehensive list of all mutations harbored by all isolates. Importantly, 22 PZAR isolates (10%) had a WT pncA gene and promoter. All 22 tested negative for PZase activity (Table 2 and Supplementary Table ST2). These 22 isolates were not part of the same clonal expansion (based on the lineage typing) (Supplementary Table ST2).
In 224 PZAR isolates, we observed 136 unique protein-altering polymorphisms in pncA and 6 unique mutations in its promoter. Of these, 40 polymorphisms in the gene and three (all indels) in the promoter had not been previously reported and are referred to here as novel mutations (Supplementary Table ST3)14.
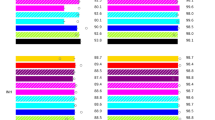
The distribution of mutations across the gene is shown in Fig. 1. The most variable locus was codon 14 (Fig. 1a). Two variants were observed in the codon, Cys14Arg and Cys14STOP. Cys14Arg was the most frequently observed mutation (20 isolates from South Africa). Eighteen had identical MIRU-VNTR and spoligotyping patterns suggesting a clonal expansion (East-Asian, Beijing sublineage). Cys14STOP was observed in one isolate from Moldova and belonged to the Euro-American lineage.

Distribution of pncA mutations in (a) PZAR and (b) PZAS clinical M. tuberculosis isolates. Frequencies labeled as “Heterogeneous” represent calls that had sufficient support for both a variant and the reference, indicative of mixed populations. “Monoclonal” frequencies represent calls that were clearly supportive of a variant. The frequencies presented here are the totals over all the different mutations observed at each codon.
Mutations in pncA of PZAS isolates
Of the 72 susceptible isolates, 25 harbored a mutation in the coding region of pncA and/or in its promoter (Table 3 and Fig. 1b). Twenty-six (22 coding and 4 promoter) unique mutations in pncA of PZAS isolates were observed. Of the coding region mutations, 13 were novel, and of the promoter mutations, 2 were novel (Supplementary Table ST4). The most frequent non-synonymous polymorphism was Thr47Ala, occurring in three PZAS isolates, all of which tested positive for PZase activity (Fig. 1b).
Lineage-based Analysis of pncA mutations
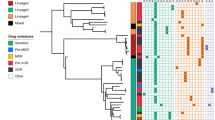
Supplementary Figure SF1 depicts lineage-based stratification of mutations observed in pncA, both in resistant and susceptible isolates. The gene and its promoter were divided into seven “zones” and prevalence of mutations in isolates from each lineage was assessed. The results of this analysis are shown in Supplementary Table ST5. Most notable was the relatively high percentage (15%) of Euro-American PZAR isolates with WT pncA and promoter. Furthermore,”hot spots” were observed in specific lineages: codons 1–30 for East-Asian, 121–150 for Indo-Oceanic, and codons 151 and higher for Euro-American. Similarly, there appears to be “cold spots” (31–60 for East-Asian and codons 91–120 for Euro-American), where very few isolates from these lineages harbored a mutation. Finally, the range between codons 91 and 120 seems to be a cold spot for all lineages, except for East-Asian. These patterns need to be confirmed in larger cohorts.
Mutations in rpsA
Twenty PZAR and eight PZAS isolates harbored a mutation in RpsA (18 PZAR, seven PZAS) or rpsA’s promoter (2 PZAR, 1 PZAS) region (Supplementary Table ST2). Of these 14 PZAR and 4 PZAS isolates only had heterogeneous mutations in the rpsA and its promoter. Of the 22 resistant isolates without a mutation in pncA or its promoter, three had a heterogeneous, non-synonymous mutation in rpsA (deletion of C in nucleotide 660, deletion of a C in nucleotide 1065 [novel], and deletion of a C in nucleotide 1142 [novel]). The three showed no PZase activity on Wayne’s assay and had no mutations in panD. The most frequent rpsA variant was the previously reported synonymous change, Arg212Arg (99 PZAR and 20 PZAS isolates)26. This mutation has been identified as a Lineage 2 (East-Asian) marker. In our set, this mutation was harbored by three Euro-American isolates as well (Supplementary Table ST6)29.
Mutations in panD
Previous studies have reported panD to be a potential target for PZA25, 30. In this study, no monoclonal mutations were found in panD’s promoter or coding region. Of the PZAR isolates without a mutation in pncA, one had a heterogeneous mutation in panD (-G291) (Supplementary Table ST2). This isolate showed no PZase activity.
Resistant Cases with WT promoter and coding regions in the three genes
Eighteen PZAR isolates had no mutations in the promoter or the enzyme of the three genes considered in this study. All tested negative for enzymatic activity. Nine of the 18 belonged to Euro-American lineage, while eight were East-Asian (Beijing), and one was Indo-Oceanic.
Heterogeneous Populations in pncA
The mutation counts reported here also include heterogeneous variants. Mixed populations were detected in pncA (coding and promoter region) of 40 isolates (34 PZAR, 6 PZAS) (Supplementary Tables ST7 and ST2). In 13 of the 34 PZAR isolates, the heterogeneous variant was the only polymorphism in the three genes. Nine heterogeneous variants were observed in the 13 isolates (Supplementary Table ST8). The most frequent of these variants was the novel insertion of C in nucleotide 453 which was observed in five resistant isolates. Three belonged to East-Asian, three belonged to Indo-Oceanic, two belonged to CAS, and one was Euro-American, ruling out the possibility of clonal expansion. In rpsA (coding and promoter region), 21 isolates (16 PZAR, 5 PZAS) had heterogeneous calls, and in panD, 11 isolates (8 PZAR, 3 PZAS) exhibited this behavior. No isolate had heterogeneity in more than one of the studied genes. The frequency of a heterogeneous observation in pncA of PZAR isolates was notably higher than that of PZAS isolates (15% resistant versus 8% susceptible). These frequencies were (7% versus 7%) for rpsA and (4% versus 4%) for panD (Supplementary Table ST7).
Discussion
This multinational study is based on strains collected from pulmonary TB patients in four high burden countries. Our primary objective was to determine the accuracy of a molecular test to diagnose PZA resistance in our set of MDR- and XDR-TB patients from high TB burden regions. Three genes, pncA, rpsA, and panD, were considered in this study. Although each gene has been well-studied independently, a concurrent assessment of all three in MDR- and XDR-TB patients from multiple high-burden countries has been limited.
Correlation with resistance to other drugs
Among our isolates, broader resistance to other drugs directly translated to higher prevalence of PZA resistance. None of our isolates that were susceptible to the other seven drugs were PZAR, while 38% of those mono resistant to one of the other drugs, 69% of MDR isolates, and 86% of XDR isolates were PZAR (Supplementary Figure SF2). While it is known that PZA resistance is associated with MDR status2, such a direct relationship to the breadth of resistance to second line drugs, beyond MDR, is less established and should be investigated further in larger cohorts.
Phenotypic accuracy
Both false resistance and susceptibility have been noted for MGIT PZA DST in literature. The prevalence of false resistance, however, has been reported to be unusually high11. Over-inoculation is a common cause of false resistance and is a frequently the suspected reason for phenotypic-genotypic discordance31, 32. Using orthogonal confirmation (see the Phenotyping section in Methods), we confirmed lack of enzymatic activity in all 22 phenotypic-genotypic discordant PZAR isolates (with WT pncA and promoter) (Table 2). We were also able to establish the presence of enzymatic activity in 19 of the 22 phenotypic-genotypic discordant PZAS isolates (with a mutant pncA) (Table 2). Overall, we observed 95% concordance between DST and enzymatic activity (Cohen’s Kappa = 0.86). (Table 2) Majority of discordant cases (4 out of 5) were susceptible isolates with a mutant pncA. We hypothesize that this relates to mutations that do not cause a disruption in enzymatic activity or do so minimally causing low level resistance undetectable by the current cutoff. (Please see the sections on Sensitivity/Specificity and Causation).
Novel pncA mutations
Overall 43 of the 142 (30%) unique variants observed in pncA of our PZAR isolates were previously not reported. (Supplementary Table ST3) Similarly, 15 of the 26 (58%) variants observed in pncA of our PZAS isolates were novel. The high percentage of novel pncA variants is not unusual. The variable nature of the gene is well documented and hundreds of unique mutations have already been reported2, 14, 23, 33. The notably higher rate of novel variants observed in PZAS isolates is new. This may reflect a bias toward sequencing resistant isolates in the past—a practice that needs to change since an accurate catalog of mutations not associated with resistance is essential for molecular diagnostics. Among others, Whitfield et al. reported 10 pncA mutations that do not confer PZA resistance at the cut off of 100 mg/L34. Here, we add 15 more polymorphisms to the list (Supplemental Table ST4).
Sensitivity/specificity
A wide range of sensitivities have been regionally reported for pncA mutations, ranging from 45.7% in Rio de Janeiro35 to 93% in China36. We report 90.2% (202/224) concordance between pncA genotype and phenotype among our resistant isolates. This is in line with some previous reports11, 26, 37, and higher than the global sensitivity of 83%14. A wide range of specificities has also been reported in the literature. For example, Osman et al. reported a specificity of 63% for pncA mutations38, while, Juréen et al. reported a specificity of 97.3% in China36. We report a specificity of pncA-based diagnostics in our study at 65% (25/72 PZAS isolates had a mutant pncA or promoter) which is notably lower than the global specificity of 90%14, but within the reported regional ranges14, 23, 39. It is known that not all changes affect the function of the enzyme significantly. The lower specificity in our study is due to the large number of novel pncA polymorphisms observed in our PZAS isolates. Since the phenotype has been confirmed by the enzymatic activity, as mentioned, we believe that these mutations either do not change the function of the enzyme or do so minimally causing low levels of resistance below MGIT cutoff.
An important note about the sensitivity and specificity reported here is that these percentages depend on the criteria used for their calculation. Several such criteria have been proposed in the literature. The most common, and one that we have used, employs all pncA promoter or PZase variants as a marker for resistance. This provides the highest sensitivity but low specificity. Alternatively, all mutations observed in susceptible isolates could be excluded, providing 100% specificity but dramatically reducing sensitivity from 90% to 65% (146/224) in our study. Miotto et al.23 propose a few different criteria, all of which would produce percentages between the two extremes calculated here. For instance, excluding mutations over 20 base pairs transcriptionally upstream of the gene would improve specificity from 65% to 70% but reduce sensitivity below 90%. The choice of this criterion will have important implications for molecular diagnostic platforms.
Lineage trends
Several trends can be noted in Supplementary Table ST5. Perhaps the one bearing most significance is that the Euro-American lineage is the most likely to escape molecular diagnostics, as it has the highest percentage (15%) of resistant isolates without a mutation in pncA or its promoter. Furthermore, the hot spot regions identified could indicate regional convergent evolution associated with PZA resistance.
Role of rpsA
The gene rpsA has held a hotly debated position within the literature, as there have been multiple publications both supporting and dismissing the gene’s role in PZA resistance24, 26, 40, 41 While the trans-translational function of rpsA was shown to be inhibited by PZA (thought to explain PZA resistance in isolates without a pncA mutation)24, Alexander et al. were not able to find any phenotypically informative mutations in the gene26. Regardless, due to low prevalence, the predictive value of rpsA as an indicator for PZA resistance tends to be relatively low. In this study, only three heterogeneous frameshifts in rpsA (-C1065, -C1142, and -CA660) could potentially hold the molecular basis for otherwise unexplained resistant cases (Supplementary Table ST2). All three were novel and their causal role in resistance needs to be confirmed. Assuming a causal role for all three mutations, the diagnostic sensitivity of RpsA was around 1% (3/224) in this study.
Role of panD
Similarly, mutations in panD have been associated with PZA resistance in isolates with a WT pncA 25, 30. We only observed one such potential case. Dillon et al. postulated that media supplemented with pantothenate, certain pantothenate analogs, or other metabolites likely explained the PZA resistance of strains with mutations in panD 27. The authors proposed that PZA resistance was independent of mutations in panD.
Causation
Generally, all changes in PZase are associated with PZA resistance4, 12, yet this is not true for all mutations14, 23. Some changes may still render a functional enzyme42, 43, leading to low level resistance. Understanding the effects of these changes on the enzyme is crucial. Furthermore, the prevalence of unexplained resistance cases is currently likely underestimated since laboratory confirmation of the role of most variants in resistance is still lacking. This work could identify polymorphisms that do not play a role in resistance, or cause low levels of resistance well below the cutoff, adding to the number of unexplained resistance cases. As such, the causal role of all pncA, rpsA, and panD mutations in resistance should be experimentally confirmed in M. tuberculosis, similar to studies performed on inhA 44, katG 45, rpoB 46, 47, and gyrA 48, 49.
Alternative mechanisms
In this study, 18 PZAR isolates lacked any polymorphisms in the three genes. Other studies have also reported such resistant cases14, 23. A complementary or alternative mechanism of resistance, other than rpsA and panD, is most frequently suspected. A complementary mechanism regulating expression of PZase would explain the resistant cases with a WT gene. rpsA and panD do not adequately address this problem since both are considered targets of POA (activated form of PZA by PZase)24, 25, 27. Such a mechanism has proven to be elusive in spite of efforts in a number of laboratories around the world.
Heterogeneity
Chemotherapy in a host with mixed bacterial population selects for the resistant subpopulation50. Undetected heterogeneity could be an explanation for unexplained resistant cases. Using our WGS approach, we were able to detect low levels of heteroresistance, closer to the sensitivity of MGIT DST (10%)51. It is still possible that some unexplained resistance cases are due to existence of small resistance subpopulation detectable by DST but not by our WGS. Heterogeneity, as detected by our approach, seemed to be a random event in panD and rpsA with equal frequencies among resistant and sensitive isolates (Supplementary Table ST8). In pncA, however, heterogeneity had a notably higher frequency (nearly two-fold) among resistant as compared to susceptible isolates with a diagnostic specificity of 92% (Supplemental Table ST7). The association of heterogeneity with phenotypic resistance and its utility in diagnostics needs to be investigated in a larger cohort. In this study, we considered resistant cases with heterogeneous pncA mutations as explained cases.
Conclusion
A diagnostic approach, based on all pncA mutations, seems to be more appropriate than any selective criterion suggested in the literature as a diagnostic platform would err more on the false resistance side. While pncA as a whole demonstrated high association with PZA phenotype, rpsA and panD did not among our isolates and elsewhere52. The existence of 18 PZAR isolates lacking PZase activity with WT promoter and coding regions of the three genes may suggest a missing regulatory component in the currently understood mechanism of resistance. The high number of novel variations in PZase of PZAS isolates may suggest an undersampling of PZA-susceptible XDR-TB isolates in sequencing. For a comprehensive picture of the pncA genotype, this needs to be corrected. We also demonstrated that heterogeneity in pncA may not be a random event and that there are lineage-specific patterns among pncA mutations.
Overall, the results of this study demonstrate that a molecular diagnostic platform may suffer from a notable false resistance or false susceptibility error rate among MDR- and XDR-TB cases. In high TB burden countries this would introduce a non-negligible number of misdiagnosed cases.
Materials and Methods
Isolate Selection
M. tuberculosis strains were isolated from patient sputum in four countries (India, Moldova, Philippines, and South Africa). This effort was performed as part of a separate project called the Global Consortium for Drug-resistant tuberculosis Diagnosis (GCDD)53. Details of patient selection and sample collection methodology are described by Garfein et al.28 and in the Supplementary Methods. All sequencing and phenotypic data was downloaded from the publically available repository on NCBI (BioProject: PRJNA353873).
MIRU-VNTR, Spoligotyping, and Lineage Determination
Genotyping using mycobacterial interspersed repetitive units variable number of tandem repeats (MIRU-VNTR) and spoligotyping were described by Garfein et al.28. Lineage determination based on MIRU and spoligo information was also described by Garfein et al.28. A brief summary is provided in the Supplementary Methods.
Phenotyping
All isolates were tested for phenotypic resistance to seven first- and second-line drugs, INH, RIF, three injectable antibiotics (kanamycin, amikacin, capreomycin), and two from the quinolone group of drugs (moxifloxacin and ofloxacin). DST results for these drugs have been previously published by Garfein et al.28. Standard BACTEC MGIT 960 methods were performed using WHO recommended critical concentrations.
PZA susceptibility testing was performed on BACTEC MGIT 960 for this study. Isolates with discrepant phenotypic and pncA genotypic results were further examined for PZase activity54. A brief description of both susceptibility testing and enzyme activity is located in the Supplemental Methods.
To test the validity of our phenotypic results we explored two common validation approaches: parallel and orthogonal testing. Parallel testing would require the DST to be repeated while orthogonal testing would require an independent method with an independent error profile as compared to that of MGIT DST, such as Wayne’s enzymatic assay. Its error profile is the opposite of DST: higher false sensitivity rates but much lower false resistance rates55. Because this study aims to identify molecular markers that can be used for diagnosis of resistance, we chose the orthogonal approach for its lower likelihood of false resistance error. A wide range of rates for false resistance has been reported for PZA DST with some as high as 60%32, 56, 57. Recently this rate was estimated to be at 11.3% by Murray et al.58. The parallel approach with a repeat DST, therefore, would have ~1% false resistance rate (assuming a white noise, nonsystematic, random error event—otherwise higher) when both results agree. Wayne’s assay has a 3% false resistance rate as most of its errors belong to the false sensitivity category55. As such, orthogonal testing has a false resistance rate of 0.3% (1/3 that of the parallel approach) when the results of both tests agree. Additionally, since it has not yet been established whether the false resistance rate of DST is a problem with the method or a characteristic of certain isolates (e.g. “flip-flopping” between multiple DST results), orthogonal testing allows the separation and investigation of the two potential causes.
Whole-Genome Sequencing
Sample and library preparation and post-sequencing analysis are described in the Supplementary Methods. Base calling was performed by consideration of reads supporting major and minor variants. Positions with a minor variant were labeled as “heterogeneous”, otherwise, the position was considered “monoclonal”. Minor variants were called using the criterion suggested by Black et al.59. For genotypic-phenotypic analysis we considered heterogeneous populations (in positions of consequence) as resistant since a mutant subpopulation was detected.
For this study, we considered the promoter (200 base pairs transcriptionally upstream from the annotated start site) and the coding regions of three genes: pncA (rv2043c), rpsA (rv1630), and panD (rv3601c). The genome positions for the six regions based on H37Rv reference (GenBank accession NC_000962.3) are listed in Supplementary Table ST9. These regions were examined for presence of genomic variation using the variant analysis methods described above and in the Supplementary Methods.
References
World Health Organization. Global Tuberculosis Report 2015. 1 (2015).
Whitfield, M. G. et al. A Global Perspective on Pyrazinamide Resistance: Systematic Review and Meta-Analysis. PLoS One 10, e0133869 (2015).
Salfinger, M. & Heifets, L. B. Determination of pyrazinamide MICs for Mycobacterium tuberculosis at different pHs by the radiometric method. Antimicrob. Agents Chemother. 32, 1002–4 (1988).
Zhang, Y. & Mitchison, D. The curious characteristics of pyrazinamide: a review. Int J Tuberc Lung Dis 7, 6–21 (2003).
Andries, K. et al. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science 307, 223–7 (2005).
Rosenthal, I. M. et al. Daily dosing of rifapentine cures tuberculosis in three months or less in the murine model. PLoS Med. 4, e344 (2007).
Tasneen, R., Tyagi, S., Williams, K., Grosset, J. & Nuermberger, E. Enhanced bactericidal activity of rifampin and/or pyrazinamide when combined with PA-824 in a murine model of tuberculosis. Antimicrob. Agents Chemother. 52, 3664–8 (2008).
Nuermberger, E. et al. Powerful bactericidal and sterilizing activity of a regimen containing PA-824, moxifloxacin, and pyrazinamide in a murine model of tuberculosis. Antimicrob. Agents Chemother. 52, 1522–4 (2008).
Leibert, E. & Rom, W. N. New drugs and regimens for treatment of TB. Expert Rev. Anti. Infect. Ther. 8, 801–13 (2010).
World Health Organization. Guidelines for surveillance of drug resistance in tuberculosis– 4th ed. WHO/HTM/TB/2009.422 (2009).
Hoffner, S. et al. Proficiency of drug susceptibility testing of Mycobacterium tuberculosis against pyrazinamide: the Swedish experience. Int. J. Tuberc. Lung Dis. 17, 1486–90 (2013).
Scorpio, A. & Zhang, Y. Mutations in pncA, a gene encoding pyrazinamidase/nicotinamidase, cause resistance to the antituberculous drug pyrazinamide in tubercle bacillus. Nat Med 2, 662–7 (1996).
Zimic, M., Fuentes, P. & Gilman, R. Pyrazinoic acid efflux rate in Mycobacterium tuberculosis is a better proxy of pyrazinamide resistance. Tuberc. 92, 84–91 (2012).
Ramirez-Busby, S. M. & Valafar, F. A Systematic Review of Mutations in Pyrazinamidase Associated with Pyrazinamide Resistance in Mycobacterium tuberculosis Clinical Isolates. Antimicrob. Agents Chemother. 59, 5267–5277 (2015).
Whitfield, M. G. et al. Mycobacterium tuberculosis pncA Polymorphisms That Do Not Confer Pyrazinamide Resistance at a Breakpoint Concentration of 100 Micrograms per Milliliter in MGIT. J. Clin. Microbiol. 53, 3633–5 (2015).
Maruri, F. et al. A systematic review of gyrase mutations associated with fluoroquinolone-resistant Mycobacterium tuberculosis and a proposed gyrase numbering system. J. Antimicrob. Chemother. 67, 819–31 (2012).
Georghiou, S. B. et al. Evaluation of genetic mutations associated with Mycobacterium tuberculosis resistance to amikacin, kanamycin and capreomycin: a systematic review. PLoS One 7, e33275 (2012).
Seifert, M., Catanzaro, D., Catanzaro, A. & Rodwell, T. C. Genetic Mutations Associated with Isoniazid Resistance in Mycobacterium tuberculosis: A Systematic Review. PLoS One 10, e0119628 (2015).
Aono, A., Chikamatsu, K., Yamada, H., Kato, T. & Mitarai, S. Association between pncA gene mutations, pyrazinamidase activity, and pyrazinamide susceptibility testing in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 58, 4928–30 (2014).
Cuevas-Córdoba, B., Xochihua-González, S. O., Cuellar, A., Fuentes-Domínguez, J. & Zenteno-Cuevas, R. Characterization of pncA gene mutations in pyrazinamide-resistant Mycobacterium tuberculosis isolates from Mexico. Infect. Genet. Evol., doi:10.1016/j.meegid.2012.12.013 (2013).
Pholwat, S. et al. Pyrazinamide susceptibility testing of Mycobacterium tuberculosis by high resolution melt analysis. Tuberc. 94, 20–5 (2014).
Jnawali, H. N. et al. Characterization of mutations in multi- and extensive drug resistance among strains of Mycobacterium tuberculosis clinical isolates in Republic of Korea. Diagn Microbiol Infect Dis. 76, 187–96 (2013).
Miotto, P. et al. Mycobacterium tuberculosis Pyrazinamide Resistance Determinants: a Multicenter Study. MBio 5, (2014).
Shi, W. et al. Pyrazinamide inhibits trans-translation in Mycobacterium tuberculosis. Science 333, 1630–2 (2011).
Zhang, S. et al. Mutations in panD encoding aspartate decarboxylase are associated with pyrazinamide resistance in Mycobacterium tuberculosis. Emerg. Microbes Infect. 2, e34 (2013).
Alexander, D. C. et al. Gene sequencing for routine verification of pyrazinamide resistance in Mycobacterium tuberculosis: a role for pncA but not rpsA. J Clin Microbiol. 50, 3726–8 (2012).
Dillon, N. A., Peterson, N. D., Rosen, B. C. & Baughn, A. D. Pantothenate and pantetheine antagonize the antitubercular activity of pyrazinamide. Antimicrob. Agents Chemother. 58, 7258–63 (2014).
Garfein, R. S. et al. Phenotypic and genotypic diversity in a multinational sample of drug-resistant Mycobacterium tuberculosis isolates. Int J Tuberc Lung Dis 19, 420–7 (2015).
Coll, F. et al. A robust SNP barcode for typing Mycobacterium tuberculosis complex strains. Nat. Commun. 5, 4812 (2014).
Shi, W. et al. Aspartate decarboxylase (PanD) as a new target of pyrazinamide in Mycobacterium tuberculosis. Emerg. Microbes Infect. 3, e58 (2014).
Demers, A.-M. et al. Direct Susceptibility Testing of Mycobacterium tuberculosis for Pyrazinamide by Use of the Bactec MGIT 960 System. J. Clin. Microbiol. 54, 1276–81 (2016).
Piersimoni, C. et al. Prevention of false resistance results obtained in testing the susceptibility of Mycobacterium tuberculosis to pyrazinamide with the Bactec MGIT 960 system using a reduced inoculum. J. Clin. Microbiol. 51, 291–4 (2013).
Campbell, P. J. et al. Molecular detection of mutations associated with first- and second-line drug resistance compared with conventional drug susceptibility testing of Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 55, 2032–41 (2011).
Whitfield, M. G. et al. Mycobacterium tuberculosis pncA polymorphisms that do not confer pyrazinamide resistance at a breakpoint concentration of 100 micrograms per milliliter in MGIT. J. Clin. Microbiol. 53, 3633–3635 (2015).
Bhuju, S. et al. Mycobacterium tuberculosis isolates from Rio de Janeiro reveal unusually low correlation between pyrazinamide resistance and mutations in the pncA gene. Infect Genet Evol. 19, 1–6 (2013).
Juréen, P., Werngren, J., Toro, J.-C. & Hoffner, S. Pyrazinamide resistance and pncA gene mutations in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 52, 1852–4 (2008).
Sheen, P. et al. Effect of pyrazinamidase activity on pyrazinamide resistance in Mycobacterium tuberculosis. Tuberc. 89, 109–13 (2009).
Osman, F. et al. High Resolution Melting Curve Analysis for Rapid Detection of Pyrazinamide Resistance in Mycobacterium tuberculosis Clinical Isolates. J. Tuberc. Res. 4, 155–172 (2016).
Ando, H. et al. Pyrazinamide resistance in multidrug-resistant Mycobacterium tuberculosis isolates in Japan. Clin Microbiol Infect 16, 1164–8 (2010).
Simons, S. O., Mulder, A., van Ingen, J., Boeree, M. J. & van Soolingen, D. Role of rpsA gene sequencing in diagnosis of pyrazinamide resistance. J. Clin. Microbiol. 51, 382 (2013).
Alexander, D. C. et al. Reply to ‘role of rpsA gene sequencing in diagnosis of pyrazinamide resistance’. J. Clin. Microbiol. 51, 383 (2013).
Petrella, S. et al. Crystal structure of the pyrazinamidase of Mycobacterium tuberculosis: insights into natural and acquired resistance to pyrazinamide. PLoS One 6, e15785 (2011).
Lemaitre, N., Callebaut, I., Frenois, F., Jarlier, V. & Sougakoff, W. Study of the structure-activity relationships for the pyrazinamidase (PncA) from Mycobacterium tuberculosis. Biochem. J. 353, 453–8 (2001).
Banerjee, A. et al. inhA, a gene encoding a target for isoniazid and ethionamide in Mycobacterium tuberculosis. Science 263, 227–30 (1994).
Rouse, D. A., DeVito, J. A., Li, Z., Byer, H. & Morris, S. L. Site-directed mutagenesis of the katG gene of Mycobacterium tuberculosis: effects on catalase-peroxidase activities and isoniazid resistance. Mol. Microbiol. 22, 583–92 (1996).
Miller, L. P., Crawford, J. T. & Shinnick, T. M. The rpoB gene of Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 38, 805–11 (1994).
Taniguchi, H. et al. Rifampicin resistance and mutation of the rpoB gene in Mycobacterium tuberculosis. FEMS Microbiol. Lett. 144, 103–8 (1996).
Malik, S., Willby, M., Sikes, D., Tsodikov, O. V. & Posey, J. E. New insights into fluoroquinolone resistance in Mycobacterium tuberculosis: functional genetic analysis of gyrA and gyrB mutations. PLoS One 7, e39754 (2012).
Barnard, F. M. & Maxwell, A. Interaction between DNA gyrase and quinolones: effects of alanine mutations at GyrA subunit residues Ser(83) and Asp(87). Antimicrob. Agents Chemother. 45, 1994–2000 (2001).
Liu, Q. et al. Within patient microevolution of Mycobacterium tuberculosis correlates with heterogeneous responses to treatment. Sci. Rep. 5, 17507 (2015).
Glader, M., Hoffner, S. & Werngren, J. Detection of pyrazinamide heteroresistance in Mycobacterium tuberculosis. Int. J. Mycobacteriology 4, 29 (2015).
Gu, Y. et al. Pyrazinamide resistance among multidrug-resistant tuberculosis clinical isolates in a national referral center of China and its correlations with pncA, rpsA, and panD gene mutations. Diagn. Microbiol. Infect. Dis. 84, 207–11 (2016).
Hillery, N. et al. The Global Consortium for Drug-resistant Tuberculosis Diagnostics (GCDD): design of a multi-site, head-to-head study of three rapid tests to detect extensively drug-resistant tuberculosis. Trials 15, 434 (2014).
Wayne, L. G. Simple pyrazinamidase and urease tests for routine identification of mycobacteria. Am Rev Respir Dis. 109, 147–51 (1974).
Chang, K. C., Yew, W. W. & Zhang, Y. Pyrazinamide susceptibility testing in Mycobacterium tuberculosis: a systematic review with meta-analyses. Antimicrob. Agents Chemother. 55, 4499–505 (2011).
Aragón, L. M., Garrigó, M., Moreno, C., Español, M. & Coll, P. Evaluation of the BacT/ALERT PZA kit in comparison with the BACTEC 460TB PZA for testing Mycobacterium tuberculosis susceptibility to pyrazinamide. J Antimicrob Chemother 60, 655–7 (2007).
Aono, A., Hirano, K., Hamasaki, S. & Abe, C. Evaluation of BACTEC MGIT 960 PZA medium for susceptibility testing of Mycobacterium tuberculosis to pyrazinamide (PZA): compared with the results of pyrazinamidase assay and Kyokuto PZA test. Diagn. Microbiol. Infect. Dis. 44, 347–352 (2002).
Velásquez, G. E. et al. Pyrazinamide Resistance Assays and Two-Month Sputum Culture Status in MDR-TB Patients. Antimicrob. Agents Chemother. (Accepted) (2016).
Black, P. A. et al. Whole genome sequencing reveals genomic heterogeneity and antibiotic purification in Mycobacterium tuberculosis isolates. BMC Genomics 16, 857 (2015).
Acknowledgements
We would like to acknowledge Dr. James Posey from the CDC and Dr. Erik Böttger from University of Zurich for their role in defining a procedure combining D.S.T. and enzymatic assay for reliable phenotypic determination. We also would like to acknowledge A. Amallraja, A. Goodmanson, R. Shanmugam, and A. Zlotnicki for assistance in variant calling, synonymy analysis, and mutation counting. We would also like to acknowledge Drs T.C. Victor, C. Rodrigues, M.T. Gler, and V. Crudu, who were in charge of isolate selection at the four study sites for GCDD. This work was supported by a grant from National Institute of Allergy and Infectious Diseases (NIAID Grant No. R01AI105185). S.M. Ramirez-Busby, T.C. Rodwell, L. Fink, R.L. Jackson, M. Pettigrove, A. Catanzaro, T.C. Rodwell, and F. Valafar were supported by this grant. S.M. Ramirez-Busby and L. Fink were also supported by scholarships from a National Science Foundation Grant (no. 0966391).
Author information
Authors and Affiliations
Contributions
F.V., T.R., and A.C. designed the project. S.R.B., L.F., and F.V. wrote the manuscript. S.R.B. and L.F. performed all in silico analysis. R.L.J. and M.P. performed all D.S.T. and enzymatic assays. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ramirez-Busby, S.M., Rodwell, T.C., Fink, L. et al. A Multinational Analysis of Mutations and Heterogeneity in PZase, RpsA, and PanD Associated with Pyrazinamide Resistance in M/XDR Mycobacterium tuberculosis . Sci Rep 7, 3790 (2017). https://doi.org/10.1038/s41598-017-03452-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-03452-y
This article is cited by
-
Fungal-derived compounds and mycogenic nanoparticles with antimycobacterial activity: a review
SN Applied Sciences (2022)
-
Mycobacterium tuberculosis ribosomal protein S1 (RpsA) and variants with truncated C-terminal end show absence of interaction with pyrazinoic acid
Scientific Reports (2020)
-
Migrations do not modify Mycobacterium tuberculosis resistance rates: a 20-year retrospective study
European Journal of Clinical Microbiology & Infectious Diseases (2020)
-
Occurrence of disputed rpoB mutations among Mycobacterium tuberculosis isolates phenotypically susceptible to rifampicin in a country with a low incidence of multidrug-resistant tuberculosis
BMC Infectious Diseases (2019)
-
Molecular characterization of multidrug-resistant Mycobacterium tuberculosis (MDR-TB) isolates identifies local transmission of infection in Kuwait, a country with a low incidence of TB and MDR-TB
European Journal of Medical Research (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
