
Abstract
Public smoke-free legislation has been in place since July 2016 in a small city (Bibai) in Hokkaido (Japan); the effects of public smoke-free legislation in small cities in Japan on cardiovascular and cerebrovascular events have not been fully investigated. Monthly numbers of acute myocardial infarctions (AMIs) and stroke admissions were obtained from medical records, and the adjacent area, Naka-Sorachi, was used as a control region. According to the results of the Poisson regression, significant direct outcomes after the enactment of smoke-free legislation in Bibai city were not observed. After the implementation of the smoke-free legislation, the average monthly admission rates per population and risk ratios for AMI, stroke, and the combined outcome (AMI plus stroke) decreased in the Bibai region but increased in the control region (Naka-Sorachi), although there was no statistically significant difference between the two regions. However, significant interactions between the region (Bibai or Naka-Sorachi) and period (before or after the legislation) for stroke and the combined outcome were noted. Although a direct admission effect was not observed, the significant interaction indicated that Bibai had a decreasing trend in emergency admissions compared with the control region (Naka-Sorachi). Public smoke-free legislation in small cities may also decrease cardiovascular events.
Similar content being viewed by others

Introduction
Men have a relatively high prevalence of tobacco use in Japan compared with other developed countries [1], and smoking tobacco is the strongest risk factor for adult mortality due to noncommunicable diseases and injuries in Japan [2]. Moreover, secondhand smoke leads to fatal diseases, including cardiovascular and cancers [3,4,5,6,7], and affects fetuses, newborns, and children [8, 9]. Owing to the inadequate control of secondhand smoking in Japan, the revised Health Promotion Law will ban smoking in public facilities in April 2020, although smoking will be banned inside only those bars and restaurants with floor space greater than 100 m2 [10].
Decreasing trends in cardiovascular and cerebrovascular events after the enactment of public smoke-free legislation have been reported [11,12,13,14,15,16], and a recent meta-analysis showed a 14% reduction in coronary events in locations that implemented comprehensive legislation and an 8% decrease in locations that only had partial restrictions [17]. In Japan, a study conducted in Hyogo Prefecture, which is the second prefecture in Japan to enact public smoke-free legislation, showed a significant decrease in acute coronary syndrome in Kobe, the main city in the prefecture, but not in the whole prefecture [18]. It was speculated that a lower adherence to the smoke-free legislation in areas other than Kobe City caused the different results in the whole prefecture.
Bibai city is a small city (population: ~20,000) in Hokkaido, the northern island of Japan, and it has implemented public smoke-free legislation since July 2016. As mentioned above, the relationship between public smoke-free legislation and a decrease in the incidence of cardiovascular disease has been mainly reported in North American and European countries, and those reports targeted areas with relatively large populations, such as countries, states, or megacities. However, the effects of public smoke-free legislation in small cities in Japan on cardiovascular and cerebrovascular diseases have not been fully investigated. The aim of this study was to determine whether the public smoke-free legislation in Bibai city was associated with decreases in the numbers of acute myocardial infarctions (AMIs), stroke hospital admissions and ambulance transports.
Methods
Public smoke-free legislation in Bibai city
Bibai city is located in Hokkaido, and its average population during the study period was 23,013. Its population density was 83.0 persons per km2 in 2015 (Japan: 340.8 persons per km2). The city is a former coalfield, and its present main industry is agriculture. “Bibai City Ordinance on Prevention of Exposure to Secondhand Smoke” was adopted in December 2015 and was enacted in July 2016 to prevent citizens’ (especially pregnant women and children) health problems from secondhand smoke. The ordinance requires a total ban on smoking in buildings and affiliated places and vehicles such as kindergartens, schools, hospitals, public transport facilities, buses, trains, public institutions, facilities for the elderly, and facilities for the handicapped. On the other hand, there are different prohibitory rules for stores, banks, post offices, energy service offices, facilities for other services, common areas in buildings containing two or more stores or services; it requires a total ban on smoking outside of the designated partitioned area, while it allows smoking within the designated partitioned smoking area (room). However, it does not regulate smoking in restaurants, bars, and taverns.
Outcomes in Bibai city
Japan is divided into 341 secondary medical care areas that are designated by the government, and each of these areas manages and provides comprehensive primary and secondary healthcare services. Bibai city is located in the Minami-Sorachi secondary medical care area (Supplementary Fig. 1), and according to the Hokkaido Regional Medical Care Plan, there are a number of hospitals, including an emergency hospital for AMI (Hokkaido Chuo Rosai Hospital), one for stroke (Iwamizawa Cranial Nerve Surgery Hospital), and one for both AMI and stroke (Iwamizawa Municipal General Hospital) in the Minami-Sorachi secondary medical area [19]. The monthly admission numbers of Bibai citizens who experienced AMI and stroke (cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage) from July 2014 to June 2018 were collected from those three emergency hospitals. Moreover, AMI and stroke patients were also admitted to Sunagawa City Medical Center, which is an advanced and expert medical care center in the region. Both Iwamizawa Municipal General Hospital and Sunagawa City Medical Center are relatively close to the downtown area of Bibai city. Therefore, the admission numbers of Bibai citizens were also collected from Sunagawa City Medical Center. Since there are no national AMI and stroke registry procedures, although the National Cancer Registry System has been in place since 2018, the actual admission rates for AMI and stroke have remained unknown. According to the claims data of the national insurance system (mainly for unemployed citizens <75 years old) and the Medical Care System for Older Senior Citizens, ~16% of Bibai’s citizens were admitted to hospitals in Naka-Sorachi in the fiscal year 2016 [20]. Moreover, monthly emergency transport numbers for AMI and stroke in Bibai city were collected from a database of the Bibai city fire stations.
Outcomes in Naka-Sorachi as a control region
Naka-Sorachi, which includes five cities and five towns, is adjacent to Bibai city, and its average population during the study period was 108,564. Its population density was 50.4 persons per km2 in 2015. The region is also a former coalfield, and its present main industry is agriculture. Thus, because Naka-Sorachi is a former coalfield like Bibai, and it was easy to collect its admission data, we selected it as a control region. Monthly admission numbers for AMI and stroke with the exclusion of Bibai citizens from July 2014 to June 2018 were collected from Sunagawa City Medical Center. Naka-Sorachi also had one emergency hospital for AMI and one for stroke in Takikawa city [19]. However, the admission numbers were not collected from the two emergency hospitals in Takikawa; thus, we assumed that the admission numbers in Sunagawa City Medical Center represented the entire Naka-Sorachi admission trend.
Statistical analysis
The monthly AMI, stroke, and combination of AMI and stroke (combined outcome) numbers of emergency admissions (in both Bibai and Naka-Sorachi) and emergency transportations (Bibai city) were the outcomes. The average monthly admissions and transportation rates per population before and after the smoke-free legislation was enacted were calculated. In the risk ratio analysis, first, using the monthly population as an offset variable, a Poisson regression with before the smoke-free legislation (or the former period for Naka-Sorachi = 0) and after smoke-free legislation (or the later period for Naka-Sorachi = 1) as a predictor was calculated. Next, a Poisson regression was calculated with the smoke-free legislation and time (month) elapsed since the start of the study as predictors. Then, using before and after the smoke-free legislation, a Poisson regression with Bibai [1] or Naka-Sorachi (0) was conducted. Finally, a Poisson regression with the smoke-free legislation (before = 0, after = 1), Bibai [1] or Naka-Sorachi (0), and an interaction term of those was calculated. The latter two regression analyses were conducted with emergency admission data due to a lack of ambulance transportation data from Naka-Sorachi.
P values < 0.05 were considered statistically significant. All calculations were conducted using Stata 15.1 software (Stata Corp, College Station, TX, USA).
This study was approved by the Institutional Review Board of Asahikawa Medical University (approval no. 18160).
Results
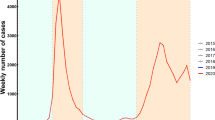
The monthly numbers of emergency admissions in Bibai and Naka-Sorachi, as well as the monthly numbers of emergency transportations in Bibai, are shown in Fig. 1. The average monthly rates per 100,000 population for emergency admissions and transportations for each group before and after the smoke-free period are also shown in Supplementary Table 1. All mean rates for after the smoke-free legislation was enacted in Bibai were smaller than those before the smoke-free legislation was enacted. On the other hand, those after the smoke-free legislation was enacted (later period) in Naka-Sorachi (control) were larger than those before the smoke-free legislation was enacted (former period).

The monthly number of emergency admissions and transportations. a Emergency admissions in Bibai. b Emergency admissions in Naka-Sorachi (control). c Emergency transportations in Bibai
Table 1 shows the risk ratios (RRs) of the smoke-free legislation for emergency admissions and transportations. In model 1 for emergency admissions in Naka-Sorachi, the combined outcome after the smoke-free legislation was enacted (later period) had a significantly higher RR (1.15, 95% confidence interval (95%CI): 1.01–1.30), and AMI admissions after the smoke-free legislation was enacted (later period) had a marginally significantly higher RR (1.24, 95%CI: 0.96 to 1.59) compared with before the smoke-free legislation was enacted. In model 1 of emergency transport in Bibai, the combined outcome after the smoke-free legislation was enacted had a marginally significantly lower RR (0.83, 95%CI: 0.67–1.03) compared with before the smoke-free legislation was enacted. However, in model 2 with both Bibai and Naka-Sorachi, no significant RRs were found.
In each period, the RRs in Bibai (reference: Naka-Sorachi) for emergency admissions are shown in Table 2. The interaction term between region (Bibai or Naka-Sorachi) and whether the smoke-free legislation had been enacted was established, and the interactions with the combined outcome and stroke showed significant differences.
Discussion
In this study, using emergency admissions and transportation count data, direct significant outcomes of the enactment of smoke-free legislation in Bibai were not observed. However, the average monthly admissions and transportation rates and RRs for AMI, stroke, and the combined outcome after the enactment of smoke-free legislation were lower, while they were higher in the control region (Naka-Sorachi), although the differences were not significant. The significant interaction terms between region (Bibai or Naka-Sorachi) and period for stroke and the combined outcome indicated that in Bibai, where the smoke-free legislation was enacted, there was a decreasing trend in emergency admissions compared with in Naka-Sorachi, which did not have a smoke-free legislation enacted. We believe the significant interaction terms indicate that the decrease in admission in Bibai was meaningful.
As mentioned above, in the meta-analysis, comprehensive smoke-free legislation reduced coronary events by 14%, and partial restrictions decreased them by 8% [17]. The earlier meta-analysis including cerebrovascular outcomes reported that comprehensive smoke-free legislation notably reduced cerebrovascular events with a RR = 0.84. Because the smoke-free legislation in Bibai was classified as a partial restriction, and the population was relatively low, our results regarding direct RR comparisons between before and after the smoke-free legislation was enacted had no statistical significance, although all RR estimations ranged from 0.82 to 0.88, reflecting a reduction of 12–18% [21].
Although no direct results with regard to event reduction after the smoke-free legislation was enacted were obtained in our study, the interaction terms between region (Bibai or Naka-Sorachi) and period for stroke and the combined outcome had statistical significance. The Japanese population has been aging rapidly, especially in nonurban areas such as Bibai and Naka-Sorachi, and the Poisson regression analyses were not adjusted for age, although they adjusted for the population size. Thus, during after period, after the smoke-free legislation was enacted in Bibai or the corresponding later period in Naka-Sorachi, those populations were aging, and the point estimations of the RRs were consistently more than one, although they had no statistical significance. However, because the point estimate RRs were consistently lower in Bibai and the interaction terms had significance, we believe that the reductions in events rates in Bibai, despite the aging of the population, indicate that the smoke-free legislation is effective.
The study period after the smoke-free legislation was enacted was 24 months long, similar to the period in the previous Hyogo study [18]. Helena study reported a 40% reduction in myocardial infarction admissions during the first 6 months after the public smoking ban law was enforced [11]. However, because larger reductions in cardiovascular events with increasing time were reported [17], further studies of the long-term effects of smoking ban legislation are needed in Japan.
The smoke-free legislation reduced not only secondhand smoke exposure but also the prevalence of active smoking [22]. These impacts can be linked to reduced cardiovascular events. However, we did not observe the actual prevalence of active smoking or data on secondhand smoke exposure. In a previous study on partial smoking bans in Japanese prefectures, the reason for the lack of a significant reduction in acute coronary events in the entire Hyogo prefecture while there was a statistically significant reduction in the main city in the prefecture (Kobe City) was thought to be worse adherence to the legislation in the prefecture, except for in the main city [18]. On the other hand, a comprehensive smoking ban (without exceptions for bars and restaurants) resulted in greater reductions [17, 22]. Therefore, we should proceed with enacting comprehensive smoke-free legislation and enhancing the adherence to the legislation for public health purposes.
The average monthly number of emergency admissions per 100,000 population in Bibai was larger than that in Naka-Sorachi. As previously mentioned, the admission numbers in all emergency hospitals in Bibai were obtained, but only the number in the largest emergency hospital in Naka-Sorachi was obtained because we assumed that the admission number in that hospital represented the trend in all of Naka-Sorachi. Therefore, this was thought to be the main reason for the larger admission number in Bibai.
Because secondhand smoke is also a risk factor for respiratory diseases, it has been reported that smoke-free legislation reduces the incidence of respiratory diseases [23, 24]. However, we did not obtain the number of admissions for respiratory disease.
There were several limitations in this study. First, because this was an ecological study, cardiovascular risk factor adjustment could not be performed, and a cause-effect relationship could not be established. In addition, the outcome definitions were not standardized, although all the emergency hospitals were able to perform coronary angiography for patients with AMI and cerebral angiography, computed tomography, and magnetic resonance imaging for stroke patients. Second, Bibai has a smaller population compared with those in previous studies conducted at the prefecture or city level. Therefore, the statistical power was not adequate, and only the interaction terms had significance. Third, we used hospital count data because there are no AMI and stroke registries. Because some patients visited remote hospitals or died suddenly without visiting the emergency hospital, we could not obtain all relevant data in the study areas. However, because the roles of the four hospitals in this study did not change during the study period, we believe the admission trend in our study reflected the whole admission trend to a large extent. We also used the emergency transport numbers for patients with AMI and stroke; the identification of patients transported by the ambulance who suffered from AMI or stroke was based on the diagnosis made by doctors after admission, although the accuracy of the diagnoses was not validated. However, because we were interested in the change over time at a single station, we believe the emergency transport trend in our study reflected the whole admission trend. Fourth, because we did not obtain the ages of the patients, we were not able to perform age-adjusted analyses. However, we used the time variable that indicated the months elapsed since the start of the study to partially reflect the aging trend. Furthermore, cardiovascular risk factors and regional differences were not adjusted for in the statistical analyses. However, many previous studies of cardiovascular events before and after the enactment of smoke-free legislation also did not adjust for cardiovascular risk factors and geographic background [17, 18]. Moreover, there seemed to be no regional events that could have affected the cardiovascular risk factors. Fifth, bars and restaurants were excluded from the smoke-free legislation, and the level of adherence to the legislation is unknown. Sixth, as previously mentioned, the actual active smoking prevalence and secondhand smoke exposure data were not obtained as in the previous Hyogo study [18]. However, many previous studies did not have information on changes in the prevalence of active smoking and secondhand smoke exposure, and it is difficult to determine what portion of the observed reduction in cardiovascular events could be attributed to reduced exposure to secondhand tobacco smoke in nonsmokers as opposed to a reduction in or elimination of smoking among smokers [17].
Conclusions
In this study in a small city in Hokkaido, no direct significant reduction in admissions was observed after the enactment of smoke-free legislation, but the admissions and transportation rates for AMI, stroke, and the combined outcome steadily decreased after the smoke-free legislation was enacted. These trends differed from the increasing trends in the outcomes in the control region (Naka-Sorachi). Significant interactions between the region (Bibai or Naka-Sorachi) and the period (before or after the smoke-free legislation was enacted) for stroke and the combined outcome were obtained, and the significant interactions indicated that Bibai, where the smoke-free legislation was enacted, had a decrease in emergency admissions compared with the control region (Naka-Sorachi), where the smoke-free legislation was not enacted. We confirmed that the smoke-free legislation reduced the number of cardiovascular events, even in a small city.
References
World Health organaization. Global Health Observatory data repository 2015. http://apps.who.int/gho/data/view.main.GDO2102v. Accessed 31 May 2019.
Ikeda N, Inoue M, Iso H, Ikeda S, Satoh T, Noda M, et al. Adult mortality attributable to preventable risk factors for non-communicable diseases and injuries in Japan: a comparative risk assessment. PLoS Med. 2012;9:e1001160.
Taylor R, Najafi F, Dobson A. Meta-analysis of studies of passive smoking and lung cancer: effects of study type and continent. Int J Epidemiol. 2007;36:1048–59.
Johnson KC, Miller AB, Collishaw NE, Palmer JR, Hammond SK, Salmon AG, et al. Active smoking and secondhand smoke increase breast cancer risk: the report of the Canadian Expert Panel on Tobacco Smoke and Breast Cancer Risk (2009). Tob Control. 2011;20:e2.
Llewellyn DJ, Lang IA, Langa KM, Naughton F, Matthews FE. Exposure to secondhand smoke and cognitive impairment in non-smokers: national cross sectional study with cotinine measurement. BMJ. 2009;338:b462.
Li J, Cui R, Eshak ES, Yamagishi K, Imano H, Muraki I, et al. Association of cigarette smoking with radial augmentation index: the Circulatory Risk in Communities Study (CIRCS). Hypertens Res. 2018;41:1054–62.
Tanaka K, Nishigori H, Watanabe Z, Iwama N, Satoh M, Murakami T, et al. Higher prevalence of hypertensive disorders of pregnancy in women who smoke: the Japan environment and children’s study. Hypertens Res. 2019;42:558–66.
Dick S, Friend A, Dynes K, AlKandari F, Doust E, Cowie H, et al. A systematic review of associations between environmental exposures and development of asthma in children aged up to 9 years. BMJ Open. 2014;4:e006554.
Zhou S, Rosenthal DG, Sherman S, Zelikoff J, Gordon T, Weitzman M. Physical, behavioral, and cognitive effects of prenatal tobacco and postnatal secondhand smoke exposure. Curr Probl Pediatr Adolesc Health Care. 2014;44:219–41.
Kokubo Y, Padmanabhan S. Necessity of Preventing Cardiovascular Disease by Smoke-Free Policies. J Am Heart Assoc. 2018;7:e011120.
Sargent RP, Shepard RM, Glantz SA. Reduced incidence of admissions for myocardial infarction associated with public smoking ban: before and after study. BMJ. 2004;328:977–80.
Basel P, Bartelson BB, Le Lait MC, Krantz MJ. The effect of a statewide smoking ordinance on acute myocardial infarction rates. Am J Med. 2014;127:94.e91–6.
Bruintjes G, Bartelson BB, Hurst P, Levinson AH, Hokanson JE, Krantz MJ. Reduction in acute myocardial infarction hospitalization after implementation of a smoking ordinance. Am J Med. 2011;124:647–54.
Christensen TM, Moller L, Jorgensen T, Pisinger C. The impact of the Danish smoking ban on hospital admissions for acute myocardial infarction. Eur J Prev Cardiol. 2014;21:65–73.
Herman PM, Walsh ME. Hospital admissions for acute myocardial infarction, angina, stroke, and asthma after implementation of Arizona’s comprehensive statewide smoking ban. Am J Public Health. 2011;101:491–6.
Stallings-Smith S, Zeka A, Goodman P, Kabir Z, Clancy L. Reductions in cardiovascular, cerebrovascular, and respiratory mortality following the national irish smoking ban: interrupted time-series analysis. PLoS ONE. 2013;8:e62063.
Jones MR, Barnoya J, Stranges S, Losonczy L, Navas-Acien A. Cardiovascular Events Following Smoke-Free Legislations: an Updated Systematic Review and Meta-Analysis. Curr Environ Health Rep. 2014;1:239–49.
Sato Y, Minatoguchi S, Nishigaki K, Hirata KI, Masuyama T, Furukawa Y, et al. Results of a prospective study of acute coronary syndrome hospitalization after enactment of a smoking ban in public places in hyogo prefecture- comparison with gifu, a prefecture without a public smoking ban. Circ J 2016;80:2528–32.
Hokkaido Regional Medical Care Plan. Hokkaido Government 2018. http://www.pref.hokkaido.lg.jp/hf/cis/iryokeikaku/aratanairyoukeikaku.htm. Accessed 31 May 2019.
Minami-sorachi Promotion Plan of Hokkaido Regional Medical Care Plan. Hokkaido Government 2018. http://www.sorachi.pref.hokkaido.lg.jp/hk/hgc/kikaku/iryosuisin/suisinhousinn.htm. Accessed 31 May 2019.
Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: a meta-analysis. Circulation. 2012;126:2177–83.
Frazer K, Callinan JE, McHugh J, van Baarsel S, Clarke A, Doherty K, et al. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst Rev. 2016;2:Cd005992.
Moraros J, Bird Y, Chen S, Buckingham R, Meltzer RS, Prapasiri S, et al. The impact of the 2002 Delaware smoking ordinance on heart attack and asthma. Int J Environ Res Public Health. 2010;7:4169–78.
Been JV, Millett C, Lee JT, van Schayck CP, Sheikh A. Smoke-free legislation and childhood hospitalisations for respiratory tract infections. Eur Respir J. 2015;46:697–706.
Acknowledgements
We thank the Bibai municipal government, Sunagawa City Medical Center, Iwamizawa Municipal General Hospital, Iwamizawa Cranial Nerve Surgery Hospital, and Hokkaido Chuo Rosai Hospital for collecting data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Saijo, Y., Ido, A., Sato, Y. et al. Acute myocardial infarction and stoke after the enactment of smoke-free legislation in public places in Bibai city: data analysis of hospital admissions and ambulance transports. Hypertens Res 42, 1801–1807 (2019). https://doi.org/10.1038/s41440-019-0299-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-019-0299-2
Keywords
This article is cited by
-
Health advocacy for reducing smoking rates in Hamamatsu, Japan
Hypertension Research (2020)
