
Abstract
Health systems are essential for suicide risk detection. Most efforts target people with mental health (MH) diagnoses, but this only represents half of the people who die by suicide. This study seeks to discover and validate health indicators of suicide death among those with, and without, MH diagnoses. This case-control study used statistical modeling with health record data on diagnoses, procedures, and encounters. The study included 3,195 individuals who died by suicide from 2000 to 2015 and 249,092 randomly selected matched controls, who were age 18+ and affiliated with nine Mental Health Research Network affiliated health systems. Of the 202 indicators studied, 170 (84%) were associated with suicide in the discovery cohort, with 148 (86%) of those in the validation cohort. Malignant cancer diagnoses were risk factors for suicide in those without MH diagnoses, and multiple individual psychiatric-related indicators were unique to the MH subgroup. Protective effects across MH-stratified models included diagnoses of benign neoplasms, respiratory infections, and utilization of reproductive services. MH-stratified latent class models validated five subgroups with distinct patterns of indicators in both those with and without MH. The highest risk groups were characterized via high utilization with multiple healthcare concerns in both groups. The lowest risk groups were characterized as predominantly young, female, and high utilizers of preventive services. Healthcare data include many indicators of suicide risk for those with and without MH diagnoses, which may be used to support the identification and understanding of risk as well as targeting of prevention in health systems.
Similar content being viewed by others

Introduction
Suicide is a major public health concern. In the United States (US), > 47,000 individuals died by suicide in 2019 [1] – a 25% increase since 2000 [2]. There is an urgent need to develop and implement effective strategies to prevent suicide using timely and accurate data to detect individuals at risk and to inform clinical outreach [3]. According to the most recent US National Strategy for Suicide Prevention, healthcare settings are important for suicide prevention [4,5,6], where they often target interventions to patients ‘known’ to be at-risk. The first step in the US suicide research strategy is to determine how to best detect individuals at-risk to strategically target suicide prevention [4].
Several innovative statistical models leveraging electronic health records (EHR) or claims data have been developed to better detect suicide risk in health systems [3], but there remain important gaps. First, most US-based studies have examined suicide ideation or attempt outcomes, and there remains an unmet need to understand risk of suicide death. Second, most of the known risk factors associated with suicide are mental health (MH) diagnoses (including MH, substance use disorders, and prior suicide attempts) [7,8,9,10,11]. Nonetheless, recent data show that while over 83% of individuals make a healthcare visit before suicide, 50% do not have a MH diagnosis [12]. Furthermore, approximately 15% of the total US population has a MH diagnosis, and half of all suicides occur among these individuals [13, 14]. However, the other half of all US suicides occur among the 85% of the population without a MH diagnosis [2, 12]. Thus, suicide risk detection and prevention directed primarily towards individuals with a known MH diagnosis can only reach half of all individuals before their death. More information is needed to identify and understand suicide risk among those without known suicide risk factors.
While two-thirds of healthcare visits before suicide occur in outpatient primary care, medical specialty settings, or the emergency department without a documented MH diagnosis [12, 15, 16], there is limited information on non-MH risk factors that may support risk detection [15, 17,18,19,20]. Clinical data may provide a solution.
This study fills major gaps by leveraging standard EHR and claims data to detect indicators of suicide risk and protection in the largest case-control study of suicide mortality among individuals receiving care in US health systems to date. Importantly, this study compares models for both those with and without MH diagnoses to juxtapose associated clinical exposures in these groups.
Methods
This case-control study was conducted within the Mental Health Research Network (MHRN). MHRN is a NIMH-funded consortium of health systems serving 30 million individuals per year. The 9 systems participating in this study are Essentia Health (Minnesota), Harvard Pilgrim Healthcare (Massachusetts), HealthPartners (Minnesota), Henry Ford Health System (Michigan), and the Colorado, Georgia, Hawaii, Northwest, and Washington state regions of Kaiser Permanente. The institutional review boards at each system approved data use for this study.
Cases were defined as individuals who died by suicide from January 1, 2000, through September 30, 2015, and were members of the participating health systems for at least 10 months of the year before death. The 10-month period is selected as individuals are often disenrolled from their health plan during the month of their death. Suicide deaths were identified by ICD-10 codes documented within official State government mortality records, which are the State-level data that comprise the National Death Index [21]. For each case, the date of death was used as a reference date to select matched controls, which were individuals affiliated with the same institution who did not die from suicide during that year. A total of 100 control individuals were randomly selected to match each case. The case-control study included 339,360 individuals—3,360 cases and 336,000 controls. Data were extracted for the 365-day period prior to the reference date for each matched set to focus on near-term indicators. Childhood (<18 years old) cases composed a minority of the sample (n = 165, 4.9%) and were excluded from the analysis. The sample after exclusions was 252,287 adults —3,195 cases and 249,092 controls. Before performing analyses, case-control sets were randomly split into discovery (2/3) and validation (1/3) samples. The sample was also annotated by those with and without a MH diagnosis (defined by those with a past year ICD 9 mental health diagnosis 290–319 or suicide attempt diagnosis E950-E959).
MHRN utilizes a virtual data warehouse to facilitate data sharing across sites [22]. Healthcare indicators for analysis included diagnoses summarized at the ICD-9 sub-chapter level, procedures at the Current Procedural Terminology (CPT) category level, and encounters at the subtype level, including hospitalizations, emergency department visits, and both outpatient visits to primary care and medical specialty settings. Visits to medical specialty settings were subdivided by clinical specialty.
For analysis, each healthcare indicator was treated as binary (“ever” = 1 or “never” = 0). Those indicators with less than 10 observations were excluded from subsequent analyses. All data collected at day 0 (the reference day), as well as emergency encounters on day 1 were excluded to avoid including data from the actual suicide. After exclusions, the analysis included 107 diagnosis sub-chapters, 67 procedure categories, and 28 encounter types.
Statistical Analysis
Supplementary Fig. 1 displays the analytical goals of the study (identification of 1. healthcare indicators associated with suicide and 2) sub-groups of at-risk patients) in the context of the methods and the corresponding sample sizes. To account for the matched design, conditional logistic regression models were used to test associations between suicide and indicators. All models were adjusted for age and sex. Differential effects by MH status were evaluated through the inclusion of a multiplicative interaction term between MH diagnosis and each indicator, with significance assessed using a likelihood ratio test. To account for multiple testing, indicators with false discovery rate adjusted p-values (FDR) < 0.05 were considered significant in the discovery sample, and those with unadjusted p-values <0.05 in the validation sample were considered validated.
Following single indicator analyses that demonstrated heterogeneity by MH status, two approaches were taken to assess multi-indicator associations with suicide. First, separate multi-indicator models were constructed for those with and without a MH diagnosis using conditional logistic models fit with a lasso penalty. These analyses were conducted using the R package clogitL1 [23], with the lasso shrinkage parameter (λ) determined using 10-fold cross-validation. For each stratum, discovery and validation models were fit using all indicators. For those indicators retained in both models, a standard conditional logistic regression model was fit to calculate 95% confidence intervals (95% CI) and tests for statistical significance in the full sample. The second approach was patient-centric, utilizing latent class analysis (LCA) to determine the existence of distinct risk sub-groups. LCA was stratified by MH status using the indicators retained in both the stratum-specific discovery and validation multi-indicator penalized models. For each LCA model, the number of classes was determined based on the Bayesian information criterion (BIC) and class interpretability in the corresponding discovery samples, and confirmatory LCA was performed to assess consistency of case percentages and utilization profiles in the corresponding validation samples. LCA was performed using MPlus v8.3. All other analyses were performed using R v3.6.1. The program and statistical code, data codebook, and dataset are available upon request and approval by the study team.
Results
Study sample description
Summary statistics for demographic variables are shown in Table 1. Overall, cases were older (mean age for cases was 51.4 years and 48.1 years for controls) and more likely to be male (cases 77.5% and controls 46.2%). Cases were less likely to have commercial insurance (cases 62.8% and controls 72.5%), more likely to live in areas with lower education levels (cases 39.1% and controls 36.9%), and had lower neighborhood household incomes (case median = $65,567 and control median = $67,694). Table 1 also shows that case/control summary statistics were consistent between discovery and validation samples.
Single healthcare indicator associations with suicide death and heterogeneity by MH status
The single indicator association results are included in Supplementary Table 1. Overall, of the 202 indicators tested in the discovery sample, 170 were significantly associated with suicide death (FDR < 0.05), and of these, 146 (86%) were also significant in the validation sample, including 78 diagnoses (77 increased/1 decreased risk), 45 procedures (44/1), and 21 encounter types (21/0). The top ten most significant, validated associations for each indicator type are summarized in Table 2.
All indicators were evaluated for differential suicide risk by MH status (Supplementary Table 2). Of the 202 individual healthcare indicators, 44 had significant interactions (FDR < 0.05) with MH status in the discovery set, with 7 (16%) also significant in the validation (p < 0.05), with MH-stratified results displayed in Table 3. Of note, malignant neoplasms were associated with >twofold higher risk among those without MH diagnoses. Given these differences, subsequent multi-indicator analyses were stratified by MH status.
Multi-indicator associations with suicide by MH status
The results from the discovery/validation penalized conditional logistic regression models stratified by MH status are displayed in Supplementary Table 3. The MH model retained 87 indicators (46 diagnoses, 30 procedures, and 11 encounters), and in the validation model, 49 indicators (24 diagnoses, 19 procedures, and 6 encounters) were retained. Increased/decreased risk of suicide was significantly associated with 7/8 diagnoses, 9/2 procedures, and 2/0 encounters. The non-MH discovery model retained 98 indicators (56 diagnoses, 29 procedures, and 13 encounters), and in the corresponding validation model, 51 indicators (25 diagnoses, 8 procedures, and 18 encounters) were retained. Increased/decreased risk was significantly associated with 7/4 diagnoses, 5/4 procedures, and 2/2 encounters.
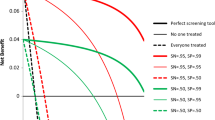
The full MH and non-MH samples were used to estimate 95% CIs and significance for indicators retained in the respective validation models, and the results for those indicators that remained statistically significant are displayed in Fig. 1. For diagnoses, several individual MH conditions increased risk, including Other Psychoses (OR = 4.00, 95% CI 3.50–4.58) and Personality Disorders and Other Nonpsychotic Mental Disorders (OR = 3.58, 95% CI 3.00–4.29). In comparison, cancer diagnoses had a unique increased risk among non-MH individuals, including Malignant Neoplasms of Other and Unspecified Sites (OR = 4.29, 95% CI 2.95–6.23) and Malignant Neoplasm of Respiratory and Intrathoracic Organs (OR = 2.90, 95% CI 1.66–5.06). In contrast, Benign Neoplasms had protective effects for both non-MH (OR = 0.65, 95% CI 0.50–0.85) and MH (OR = 0.68, 95% CI 0.55–0.84) individuals. The services related to Reproduction and Development were protective in both models, although the effect was more extreme in the non-MH (OR = 0.37, 95% CI 0.24–0.58) relative to the MH (OR = 0.60, 95% CI 0.45–0.81) model.

Results in both panels are taken from conditional logistic regression models fit to the full sample of those individual with and without mental health diagnoses. For each model, indicators were selected from those that were retained in both the discovery and validation penalized regression models, and only those that were statistically significant (p < 0.05) in the full sample were included in these figures.
For procedures, increased risk among MH individuals was distinguished by procedures related to the Respiratory System (OR = 1.95, 95% CI 1.50–2.52) and Psychiatry (OR = 1.24, 95% CI 1.08–1.43). In comparison, Radiology procedures (OR = 1.54, 95% CI 1.14–2.08) were significant for the non-MH model. The MH sample had a unique protective effect of Nursing Facility Services (OR = 0.54, 95% CI 0.36–0.81). Non-MH individuals had unique protective effects of Immunization Administration for Vaccines/Toxoids (OR = 0.82, 95% CI 0.68–0.98), Preventive Medicine Services (OR = 0.74, 95% CI 0.62–0.88), and Ophthalmology (OR = 0.76, 95% CI 0.64–0.90).
For encounters, increased risk among MH individuals was distinguished by Non-Face-to-Face Non-physician Services (OR = 1.53, 95% CI 1.13–2.07), Acute Inpatient (OR = 1.47, 95% CI 1.21–1.79), and Ambulatory - Rehab (OR = 1.53, 95% CI 1.16–2.02). For non-MH individuals, Other Non-overnight - Home Health (OR = 1.53, 95% CI 1.16–2.00) and Radiology Only - Outpatient Clinic (OR = 1.54, 95% CI 1.14–2.08) were associated with increased risk. MH individuals had no encounter types with protective effects, and non-MH individuals had protective effects for Emergency - Hospital Ambulatory (OR = 0.53, 95% CI 0.40–0.70) and Email - Other Non-hospital (OR = 0.68, 95% CI 0.52–0.88).
Latent class analysis discovery and validation of distinct patient suicide risk sub-groups
The top indicators that differentiate the LCA identified sub-groups for both MH and non-MH samples are displayed in Fig. 2. For both the MH and non-MH samples, the number of latent subgroups was identified as five, based on lowest value past the inflection point in the BIC curve (Supplementary Fig. 2) that also identified a low-risk group. For the MH sample, the groups are labelled in order of decreasing case percentage: Group 1 (10.0% of the sample, 13.8% cases), Group 2 (16.1% of the sample, 11.0% cases), Group 3 (26.0% of the sample, 4.1% cases), Group 4 (24.1% of the sample, 3.6% cases), and Group 5 (23.8% of the sample, 1.9% cases). Based on these values, Groups 1 and 2 were identified as high-risk groups for suicide. Specifically, Group 1 had higher proportions of many diagnosis sub-chapters, procedure types, and encounter types, signifying a high utilization group with multiple healthcare concerns. Group 2 had a similar but less extreme profile, and these individuals were also younger (39 years) and more likely to be female. Group 5 had the lowest case prevalence. This group was one of the youngest on average (44 years old), had the lowest proportion of males, and the highest proportion of routine/preventive health visits. Confirmatory LCA of the five-group solution in the validation sample yielded groups with similar case percentages and healthcare indicator profiles (Fig. 3).

For each mental health stratum, latent class analysis (LCA) was performed based on health care indicators identified in the respective penalized regression models in the discovery sample. LCA was performed in the discovery sample (D), followed by confirmatory LCA in the validation sample (V). The frequency of cases is displayed overall and for each LCA sub-group for both D and V samples. Within each stratum, the LCA sub-group-specific frequency are displayed for those health care indicators where at least 9 of the 10 ratios of the pairwise group frequencies were >1.5 (ie. sub-group distinguishing indicators).
For non-MH individuals, he resulting groups and their corresponding case proportions were: Group 1 (14.1% of the sample, 2.7% cases), Group 2 (21.8% of the sample, 1.7% cases), Group 3 (25.6% of the sample, 1.5% cases), Group 4 (25.3% of the sample, 1.3% cases), and Group 5 (13.3% of the sample, 0.3% cases). The noticeably high-risk Group 1 was the second oldest (59 years old) and contained much higher percentages of most healthcare indicators with multiple concerns, similar to Groups 1 and 2 from the MH sample. Further, while Groups 3 and 4 where at intermediate risk and had similar but less extreme healthcare profiles, there was an additional disengaged, high risk group (Group 2) unique to the non-MH sample. The lowest-risk Group 5 was the youngest (39 years), contained a low proportion of males (5.6%), and displayed higher proportions of routine/preventive visits – similar to Group 5 from the MH model. Confirmatory LCA of the five-group solution resulted in both similar case proportions and healthcare indicator profiles.
Discussion
Clinical data can be used to better differentiate the structure of suicide risk as well as to identify subgroups and service settings that require additional attention for suicide prevention in health systems. Importantly, this study employed multiple methods to identify and validate individual clinical indicators and patterns of those indicators, to better distinguish risk in not only those with MH diagnoses, but also among those with previously unknown risk factors. The insights into these groups with respective high and low population suicide incidence can inform clinical outreach and assessment strategies, and as such, this study adds multiple clinically and methodologically significant findings to the literature. The findings from the multi-indicator models and LCA may be most relevant and can help inform future work to determine how these complex indicators of risk can inform clinical outreach.
First, this study confirms prior research indicating that those who die by suicide often have multiple chronic or complex conditions [17, 24]. In both the MH and non-MH analyses, individuals with the highest healthcare utilization had the greatest risk for suicide, indicating an opportunity for intervention. Prior studies have focused analyses on single clinical risk factors for suicide [19, 25,26,27], but this study suggests that future research should also consider comorbidities to better distinguish risk. Suicide prevention in health systems should focus on those individuals who are frequent utilizers of services, potentially indicating higher severity of multiple conditions.
Second, older individuals with MH conditions who have low utilization may be at elevated risk. In contrast, younger females who are more engaged in routine healthcare are at lower risk. The Interpersonal Theory of Suicide indicates that isolation and burdensomeness may be important indicators of suicide [28]. These findings collectively indicate that engagement or connectedness with health systems, particularly for regular routine care, may be protective. This emphasizes the importance of clinical or community outreach in suicide prevention, especially for older individuals or males who have become disconnected from care.
Third, while suicide prevention has traditionally focused on individuals with MH conditions, we found many non-MH medical indicators associated with suicide. This supports the importance of ensuring use of low-intensity suicide risk detection methods such as the implementation of EHR-based statistical models or routine clinical screening and assessment [3, 29, 30] in primary care and other non-behavioral health settings. Brief interventions, such as safety or crisis response planning [31, 32], can be immediately offered to those at higher risk in addition to the connection with appropriate levels of follow-up specialty care.
Fourth, there were several novel protective factors for suicide identified in the study. Past studies have found few clinical protective factors for suicide. Benign cancer diagnoses were associated with reduced risk and may indicate a positive life event that contrasts other life stressors. Receipt of preventive services and vaccinations, also associated with lower risk, may suggest that those more engaged in overall health promotion and prevention have lower risk. These factors deserve more in-depth study in future research.
Fifth, the modeling plan implemented in this study was particularly innovative. Risk detection models require prespecification of exposure variables. Thus, recent predictive modeling studies have focused primarily on behavioral health factors as primary exposures [33,34,35,36,37]. MH conditions were the primary factors used in risk detection in prior studies. This was important and valuable given that health systems, including the Veterans Health Administration, have begun implementing these models to stimulate clinical action [3, 38]. However, the current study uniquely identified non-MH clinical risk profiles that can help detect risk among those without MH diagnoses and differentiate risk among those with MH risk factors. The new models developed and validated in this study can also provide guidance to improve future models, including non-MH indicators.
These findings must be viewed in the context of limitations. First, the study was conducted in large health systems among individuals with health insurance. While the results are generalizable to those with many insurance types (public and commercial), individuals without insurance were not included. Second, this study used ICD-9 diagnosis codes. Future studies should replicate findings using ICD-10 codes recently implemented in practice. Third, this study used a case-control design, which is efficient for the estimation of indictor effects. Future studies may leverage these findings to inform absolute risk estimates using prospective cohorts. Fourth, race/ethnicity was not included, as it was not ascertained by health systems prior to 2009. While the participating systems are diverse, this may be important to include in future models. Fifth, while the validation hold-out sample did not overlap with those in the discovery, it was not possible to perform the confirmatory LCA in a separate set of health care systems. Finally, all healthcare utilization occurring on the date of, or day prior to, death were excluded to account for potential utilization that may have been part of the suicide death.
Clinical data include a range of health indicators, both risk and protective, which can be used to better detect suicide risk among those without known MH diagnoses and to better distinguish risk among those with MH diagnoses. These data can also inform targeted clinical outreach, assessment, and follow-up to those at highest risk. This may be particularly important for those with multiple conditions and those disengaged from healthcare. Suicide prevention efforts should span across the entire health system.
References
Stone DM, Jones CM, Mack KA. Changes in Suicide Rates - United States, 2018–2019. MMWR Morb Mortal Wkly Rep. 2021;70:261–268.
Stone DM, Simon TR, Fowler KA, Kegler SR, Yuan K, Holland KM, et al. Vital Signs: Trends in State Suicide Rates - United States, 1999-2016 and Circumstances Contributing to Suicide - 27 States, 2015. MMWR Morb Mortal Wkly Rep. 2018;67:617–24.
Simon GE, Matarazzo BB, Walsh CG, Smoller JW, Boudreaux ED, Yarborough BJH, et al. Reconciling Statistical and Clinicians’ Predictions of Suicide Risk. Psychiatr Serv. 2021:72:555–62.
National Action Alliance for Suicide Prevention, Research Prioritization Task Force. A Prioritized Research Agenda for Suicide Prevention: An Action Plan to Save Lives. Rockville, MD, 2014.
National Action Alliance for Suicide Prevention and Office of the Surgeon General. 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action. Washington, D.C. 2012.
Pringle B, Colpe LJ, Heinssen RK, Schoenbaum M, Sherrill J, Claassen C, et al. A strategic approach for prioritizing research and action to prevent suicide. PsychiatrServ. 2013;64:71–75.
Yeh HH, Westphal J, Hu Y, Peterson EL, Williams LK, Prabhakar D, et al. Diagnosed Mental Health Conditions and Risk of Suicide Mortality. Psychiatr Serv. 2019;70:750–7.
Ilgen MA, Bohnert AS, Ignacio RV, McCarthy JF, Valenstein MM, Kim HM, et al. Psychiatric diagnoses and risk of suicide in veterans. Arch Gen Psychiatry. 2010;67:1152–8.
Ilgen MA, Conner KR, Roeder KM, Blow FC, Austin K, Valenstein M. Patterns of treatment utilization before suicide among male veterans with substance use disorders. Am J Public Health. 2012;102(Suppl 1):S88–S92.
Prabhakar D, Peterson EL, Hu Y, Chawa S, Rossom RC, Lynch FL, et al. Serious Suicide Attempts and Risk of Suicide Death. Crisis. 2020:1–8.
Lynch FL, Peterson EL, Lu CY, Hu Y, Rossom RC, Waitzfelder BE, et al. Substance use disorders and risk of suicide in a general US population: a case control study. Addiction Sci Clin Pract. 2020;15:14.
Ahmedani BK, Simon GE, Stewart C, Beck A, Waitzfelder BE, Rossom R, et al. Health care contacts in the year before suicide death. J Gen Intern Med. 2014;29:870–7.
Mental Health Research Network. Mental Health Research Network. Health Care Systems Research Network. Published 2022. Accessed via https://mhresearchnetwork.org/.
Coleman KJ, Stewart C, Waitzfelder BE, Zeber JE, Morales LS, Ahmed AT, et al. Racial-Ethnic Differences in Psychiatric Diagnoses and Treatment Across 11 Health Care Systems in the Mental Health Research Network. Psychiatr Serv. 2016;67:749–57.
Ahmedani BK, Westphal J, Autio K, Elsiss F, Peterson EL, Beck A, et al. Variation in patterns of health care before suicide: A population case-control study. Prev Med. 2019;127:105796.
Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. 2002;159:909–16.
Ahmedani BK, Peterson EL, Hu Y, Rossom RC, Lynch F, Lu CY, et al. Major Physical Health Conditions and Risk of Suicide. Am J Prev Med. 2017;53:308–15.
Webb RT, Kontopantelis E, Doran T, Qin P, Creed F, Kapur N. Suicide risk in primary care patients with major physical diseases: a case-control study. Arch Gen Psychiatry. 2012;69:256–64.
Ilgen MA, Kleinberg F, Ignacio RV, Bohnert ASB, Valenstein M, McCarthy JF, et al. Noncancer Pain Conditions and Risk of Suicide. JAMA Psychiatry 2013;70:692–7.
Bohnert ASB, Ilgen MA. Understanding Links among Opioid Use, Overdose, and Suicide. N. Engl J Med. 2019;380:71–79.
Centers for Disease Control and Prevention. ICD framework: External cause of injury mortality matrix. http://www.cdc.gov/nchs/injury/ice/matrix10.htm. Published 2010.
Ross TR, Ng D, Brown JS, Pardee R, Hornbrook MC, Hart G, et al. The HMO Research Network Virtual Data Warehouse: A Public Data Model to Support Collaboration. eGEMS 2014;2:2.
Reid S, Tibshirani R. Regularization Paths for Conditional Logistic Regression: The clogitL1 Package. J Stat Softw. 2014;58:12.
Owen-Smith AA, Ahmedani BK, Peterson E, Simon GE, Rossom RC, Lynch FL, et al. The Mediating Effect of Sleep Disturbance on the Relationship Between Nonmalignant Chronic Pain and Suicide Death. Pain Pr. 2019;19:382–9.
Kuo CJ, Chen VC, Lee WC, Chen WJ, Ferri CP, Stewart R, et al. Asthma and suicide mortality in young people: a 12-year follow-up study. Am J Psychiatry. 2010;167:1092–9.
Breslau N, Schultz L, Lipton R, Peterson E, Welch KM. Migraine headaches and suicide attempt. Headache. 2012;52:723–31.
Lund-Sorensen H, Benros ME, Madsen T, Sørensen HJ, Eaton WW, Postolache TT, et al. A Nationwide Cohort Study of the Association Between Hospitalization With Infection and Risk of Death by Suicide. JAMA Psychiatry. 2016;73:912–9.
Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE Jr. The interpersonal theory of suicide. Psychol Rev. 2010;117:575–600.
Simon GE, Coleman KJ, Rossom RC, Beck A, Oliver M, Johnson E, et al. Risk of suicide attempt and suicide death following completion of the Patient Health Questionnaire depression module in community practice. J Clin Psychiatry. 2016;77:221–7.
Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266–77.
Stanley B, Brown GK. Safety Planning Intervention: A Brief Intervention to Mitigate Suicide Risk. Cogn Behav Pract. 2012;19:256–64.
Stanley B, Brown GK, Brenner LA, Galfalvy HC, Currier GW, Knox KL, et al. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department. JAMA Psychiatry. 2018;75:894–900.
Barak-Corren Y, Castro VM, Javitt S, Hoffnagle AG, Dai Y, Perlis RH, et al. Predicting Suicidal Behavior From Longitudinal Electronic Health Records. Am J Psychiatry. 2017;174:154–62.
Barak-Corren Y, Castro VM, Nock MK, Mandl KD, Madsen EM, Seiger A, et al. Validation of an Electronic Health Record-Based Suicide Risk Prediction Modeling Approach Across Multiple Health Care Systems. JAMA Netw Open 2020;3:e201262.
Walsh CG, Johnson KB, Ripperger M, Sperry S, Harris J, Clark N, et al. Prospective Validation of an Electronic Health Record-Based, Real-Time Suicide Risk Model. JAMA Netw Open. 2021;4:e211428.
Simon GE, Johnson E, Lawrence JM, Rossom RC, Ahmedani B, Lynch FL, et al. Predicting Suicide Attempts and Suicide Deaths Following Outpatient Visits Using Electronic Health Records. Am J Psychiatry. 2018;175:951–60.
Coley RY, Johnson E, Simon GE, Cruz M, Shortreed SM. Racial/Ethnic Disparities in the Performance of Prediction Models for Death by Suicide After Mental Health Visits. JAMA Psychiatry. 2021;78:726–34.
McCarthy JF, Bossarte RM, Katz IR, Thompson C, Kemp J, Hannemann CM, et al. Predictive Modeling and Concentration of the Risk of Suicide: Implications for Preventive Interventions in the US Department of Veterans Affairs. Am J Public Health. 2015;105:1935–42.
Acknowledgements
This project was supported by Award Numbers R01MH103539 and U19MH092201 from the National Institute of Mental Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. All authors have contributed to and have approved the final submitted manuscript.
Author information
Authors and Affiliations
Contributions
Authors contribued to study concept and design (BA, AL), acquisition of data (BA, GS, AB, RR, FL, CL, AO, YD, SW), analysis and interpretation of data (BA, CC, HY, AL), and preparation and review of manuscript (BA, CC, HY, JW, GS, AB, RR, FL, CL, AO, KS, CF, EA, GB, CB, JB, YD, SW, HG, AL).
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests. IRB approval was obtained at each participating site.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ahmedani, B.K., Cannella, C.E., Yeh, HH. et al. Detecting and distinguishing indicators of risk for suicide using clinical records. Transl Psychiatry 12, 280 (2022). https://doi.org/10.1038/s41398-022-02051-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-022-02051-4
