
Abstract
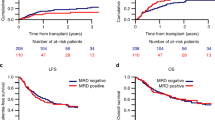
The rarity of mixed phenotype acute leukemia (MPAL) has precluded adequate data to incorporate minimal residual disease (MRD) monitoring into therapy. Fluidity in MPAL classification systems further complicates understanding its biology and outcomes; this includes uncertainty surrounding the impact of shifting diagnostic requirements even between iterations of the World Health Organization (WHO) classification. Our primary objective was to address these knowledge gaps. To do so, we analyzed clinicopathologic features, therapy, MRD, and survival in a centrally-reviewed, multicenter cohort of MPAL uniformly diagnosed by the WHO classification and treated with acute lymphoblastic leukemia (ALL) regimens. ALL induction therapy achieved an EOI MRD negative (<0.01%) remission in most patients (70%). EOI MRD positivity was predictive of 5-year EFS (HR = 6.00, p < 0.001) and OS (HR = 9.57, p = 0.003). Patients who cleared MRD by EOC had worse survival compared with those EOI MRD negative. In contrast to adults with MPAL, ALL therapy without transplantation was adequate to treat most pediatric patients. Earlier MRD clearance was associated with better treatment success and survival. Prospective trials are now necessary to validate and refine MRD thresholds within the pediatric MPAL population and to identify salvage strategies for those with poor predicted survival.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Weinberg OK, Arber DA. Mixed-phenotype acute leukemia: historical overview and a new definition. Leukemia. 2010;24:1844–51.
Bene MC, Porwit A. Acute leukemias of ambiguous lineage. Semin Diagn Pathol. 2012;29:12–8.
Steensma DP. Oddballs: acute leukemias of mixed phenotype and ambiguous origin. Hematol Oncol Clin North Am. 2011;25:1235–53.
Wolach O, Stone RM. Mixed-phenotype acute leukemia: current challenges in diagnosis and therapy. Curr Opin Hematol. 2017;24:139–45.
Maruffi M, Sposto R, Oberley MJ, Kysh L, Orgel E. Therapy for children and adults with mixed phenotype acute leukemia: a systematic review and meta-analysis. Leukemia. 2018;32:1515–28.
van Dongen JJ, Seriu T, Panzer-Grumayer ER, Biondi A, Pongers-Willemse MJ, Corral L, et al. Prognostic value of minimal residual disease in acute lymphoblastic leukaemia in childhood. Lancet. 1998;352:1731–8.
Ciudad J, San Miguel JF, Lopez-Berges MC, Vidriales B, Valverde B, Ocqueteau M, et al. Prognostic value of immunophenotypic detection of minimal residual disease in acute lymphoblastic leukemia. J Clin Oncol. 1998;16:3774–81.
Coustan-Smith E, Sancho J, Hancock ML, Boyett JM, Behm FG, Raimondi SC, et al. Clinical importance of minimal residual disease in childhood acute lymphoblastic leukemia. Blood. 2000;96:2691–6.
San Miguel JF, Vidriales MB, Lopez-Berges C, Diaz-Mediavilla J, Gutierrez N, Canizo C, et al. Early immunophenotypical evaluation of minimal residual disease in acute myeloid leukemia identifies different patient risk groups and may contribute to postinduction treatment stratification. Blood. 2001;98:1746–51.
Rubnitz JE, Inaba H, Dahl G, Ribeiro RC, Bowman WP, Taub J, et al. Minimal residual disease-directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trial. Lancet Oncol. 2010;11:543–52.
Pulsipher MA, Peters C, Pui CH. High-risk pediatric acute lymphoblastic leukemia: to transplant or not to transplant? Biol Blood Marrow Transplant. 2011;17 Suppl 1:S137–48.
Hrusak O, de Haas V, Stancikova J, Vakrmanova B, Janotova I, Mejstrikova E, et al. International cooperative study identifies treatment strategy in childhood ambiguous lineage leukemia. Blood. 2018;132:264–76.
Weinberg OK, Seetharam M, Ren L, Alizadeh A, Arber DA. Mixed phenotype acute leukemia: a study of 61 cases using World Health Organization and European Group for the immunological classification of leukaemias criteria. Am J Clin Pathol. 2014;142:803–8.
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–405.
Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4th ed. vol. 2. Lyon, France: IARC/WHO Press; 2017, p. 585.
Pomerantz A, Rodriguez-Rodriguez S, Demichelis-Gomez R, Barrera-Lumbreras G, Barrales-Benitez O, Lopez-Karpovitch X, et al. Mixed-phenotype acute leukemia: suboptimal treatment when the 2008/2016 WHO classification is used. Blood Res. 2016;51:233–41.
Oberley MJ, Li S, Orgel E, Phei Wee C, Hagiya A, O’Gorman MRG. Clinical significance of isolated myeloperoxidase expression in pediatric B-lymphoblastic leukemia. Am J Clin Pathol. 2017;147:374–81.
Raikar SS, Park SI, Leong T, Jaye DL, Keller FG, Horan JT, et al. Isolated myeloperoxidase expression in pediatric B/myeloid mixed phenotype acute leukemia is linked with better survival. Blood. 2018;131:573–7.
Hunger SP, Loh ML, Whitlock JA, Winick NJ, Carroll WL, Devidas M, et al. Children’s oncology group’s 2013 blueprint for research: acute lymphoblastic leukemia. Pediatr Blood Cancer. 2013;60:957–63.
Matutes E, Pickl WF, Van’t Veer M, Morilla R, Swansbury J, Strobl H, et al. Mixed-phenotype acute leukemia: clinical and laboratory features and outcome in 100 patients defined according to the WHO 2008 classification. Blood. 2011;117:3163–71.
Gerr H, Zimmermann M, Schrappe M, Dworzak M, Ludwig WD, Bradtke J, et al. Acute leukaemias of ambiguous lineage in children: characterization, prognosis and therapy recommendations. Br J Haematol. 2010;149:84–92.
Schrappe M, Valsecchi MG, Bartram CR, Schrauder A, Panzer-Grumayer R, Moricke A, et al. Late MRD response determines relapse risk overall and in subsets of childhood T-cell ALL: results of the AIEOP-BFM-ALL 2000 study. Blood. 2011;118:2077–84.
Alexander TB, Gu Z, Iacobucci I, Dickerson K, Choi JK, Xu B, et al. The genetic basis and cell of origin of mixed phenotype acute leukaemia. Nature. 2018;562:373–9.
Morita K, Wang F, Patel K, Bueso-Ramos CE, Zahr AA, Gumbs C, et al. Genomic landscape of adult mixed phenotype acute leukemia (MPAL). J Clin Oncol. 2017;35(Suppl 15):7023–7023.
Takahashi K, Wang F, Morita K, Yan Y, Hu P, Zhao P, et al. Integrative genomic analysis of adult mixed phenotype acute leukemia delineates lineage associated molecular subtypes. Nat Commun. 2018;9:2670.
Wolach O, Stone RM. How I treat mixed-phenotype acute leukemia. Blood. 2015;125:2477–85.
Shimizu H, Saitoh T, Machida S, Kako S, Doki N, Mori T, et al. Allogeneic hematopoietic stem cell transplantation for adult patients with mixed phenotype acute leukemia: results of a matched-pair analysis. Eur J Haematol. 2015;95:455–60.
Munker R, Labopin M, Esteve J, Schmid C, Mohty M, Nagler A. Mixed phenotype acute leukemia: outcomes with allogeneic stem cell transplantation. A retrospective study from the Acute Leukemia Working Party of the EBMT. Haematologica. 2017;102:2134–40.
Acknowledgements
Data were collated using the REDCAP database supported by NIH/NCATS, UL1TR001855, and UL1TR000130. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author information
Authors and Affiliations
Contributions
EO performed study conception and research design; MJO and GW conducted the hematopathology central review; JM and RS performed the statistical analysis; MJO, SSR, and EO wrote the paper first draft; All authors contributed case data, interpreted the analysis, and reviewed/edited paper.
Corresponding author
Ethics declarations
Conflict of interest
MJO is currently employed at Caris Life Sciences. There are no other conflicts of interest to report.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Oberley, M.J., Raikar, S.S., Wertheim, G.B. et al. Significance of minimal residual disease in pediatric mixed phenotype acute leukemia: a multicenter cohort study. Leukemia 34, 1741–1750 (2020). https://doi.org/10.1038/s41375-020-0741-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41375-020-0741-0
This article is cited by
-
Single-cell RNA sequencing distinctly characterizes the wide heterogeneity in pediatric mixed phenotype acute leukemia
Genome Medicine (2023)
-
Mixed Phenotype Acute Leukemia: Current Approaches to Diagnosis and Treatment
Current Oncology Reports (2021)
