
Abstract
Diabetes-related hearing loss (DRHL) is a complication of diabetes mellitus that is drawing more attention currently. DNA methylation has a critical role in the pathogenesis of type 2 diabetes mellitus (T2DM) and its complications. Therefore, we investigated the genome-wide DNA methylation of peripheral blood of T2DM patients with/without hearing loss in order to explore the susceptibility loci of DRHL. Between DRHL group and control group, 113 gene sites were identified to be differentially methylated regions (DMRs). Among 38 DMRs with whole samples, the classification accuracy is up to 90%. With alignment to T2DM susceptibility genes and deafness genes published, KCNJ11 was found to be the only overlapped gene. The DNA methylation level of KCNJ11 was associated with stroke (t = 2.595, p < 0.05), but not with diabetic nephropathy and diabetic retinopathy. The detective rate of distortion product otoacoustic emissions (DPOAE) from low to high frequencies (0.7–6 kHz) on the right ear was significantly correlated with the methylation level of KCNJ11. The auditory brainstem response (ABR) threshold on the right ear was also correlated (r = 0.678, p < 0.05). This DNA methylation profile indicates the susceptibility loci of DRHL. The potassium metabolism may have a critical role in the hearing loss caused by hyperglycemia.
Similar content being viewed by others

Introduction
Diabetes-related hearing loss (DRHL) is an under-recognized complication of diabetes mellitus [1]. The prevalence of DRHL reaches 34–60% according to different studies in developed countries [2, 3]. Diabetic retinopathy ranks as the leading cause to severe visual impairment in diabetics. Likewise, the cochleopathy in addition to the pathological change in spiral ganglions caused by hyperglycemia deteriorate the hearing. DRHL represents similarly as age-related hearing loss (ARHL), but it occurs at an earlier age and develops more rapidly. Some cases have the onset of sudden hearing loss and/or vertigo, normally with poor prognosis. Hearing and vision are the two most important specialized sensory inputs for taking information from the environment. Impairment in hearing and/or vision decreases the quality of life in diabetics remarkably.
Globally, China has become the country with the largest population of diabetes and pre-diabetes. Among the Chinese adults, the estimated standardized prevalence of total diagnosed and undiagnosed diabetes was 10.9%, that of pre-diabetes 35.7% [4]. Taken together, nearly one in two Chinese people suffers from diabetes or pre-diabetes. The direct medical expenditure in diabetics in China was tremendous. The average annual growth rate of direct medical expenditure of diabetes in China is 19.90%, which exceeds the growth rate of gross domestic product and national health expenditure contemporarily [5]. The direct medical cost for an individual with one complication of type 2 diabetes mellitus (T2DM) is 3.71 folds over those who without any complication. The cost increases to 10.35 folds if this T2DM patient has both micro- and macro-vascular complications [6]. The need for early detection and prevention of complications of diabetes mellitus, including DRHL, is urgent.
Our previous study found that the amplitude of distortion products otoacoustic emissions (DPOAEs) decreased significantly in diabetics even though the pure-tone average (PTA) was within normal range, indicating the sub-clinical cochleopathy in the early stage [7]. Further challenge is to identify the vulnerable individuals for DRHL.
DNA methylation has a critical role in the pathogenesis of T2DM and its complications. Multhaup and his colleagues combined three lines of evidence—diet-induced epigenetic dysregulation in mouse, epigenetic conservation in humans, and T2DM clinical risk evidence—to investigate the epigenetics of T2DM. They identified differentially DNA-methylated genomic regions, which overlap with 27 genetic T2DM risk loci [8]. Sapienza and his colleagues identified epigenetic differences between diabetes patients with end stage renal disease (ESRD) and diabetes patients without nephropathy by comparing site-specific DNA methylation levels. They found that a substantial fraction (21%) of the candidate genes have been implicated previously through other genome association or transcription profiling studies, which suggests strongly that DNA methylation difference is associated with disease predisposition [9]. These investigations support the non-Lamarckian theory raised by Feinberg and Irizarry. They proposed that genetic variants that do not change the mean genotype could change the variability of phenotype; and this could be mediated epigenetically [10]. Toperoff and his colleagues [11] found that the odds of belonging to the T2DM group increased by 6.1% for every 1% decrease in methylation. The odds ratio for decrease of 1 standard deviation of methylation was 1.5856 (95% CI: 1.2824-1.9606) and the sensitivity was better than that of the strongest known sequence variant.
A large body of evidence indicates that the change of DNA methylation is a good tool to predispose T2DM and its complications. In order to search for the biomarker of the diabetics and pre-diabetics susceptible of DRHL, we therefore explored the differentially methylated regions (DMRs) in the peripheral blood in patients with DRHL.
Methods
Subjects
The electronic charts of patients in the Endocrine Department in Beijing Tongren Hospital (Tertiary referral hospital) from 2015 to 2017 was reviewed. The PTA hearing test was routinely examined. All the cases in this study were diagnosed of T2DM according to the standard of American Diabetes Association (ADA) [12].
Inclusion criteria: T2DM was diagnosed according to ADA standard. Since the clinical progression of DRHL is similar to ARHL, the classification of human audiometric phenotypes of ARHL was referred [13]. The audiogram within the boundaries of “metabolic” type was categorized into DRHL, within the boundaries of “older-normal” type was categorized into control. The age ranges from 30 to 65 years old.
Exclusion criteria: Otitis media with perforation on tympanic membrane, history of exposure to noise, administration of ototoxic medication, trauma on ear and/or skull, older than 65 years old, severe cognitive deficiency, or mental illness.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Clinical data collection
A questionnaire was filled up for each subject. Basic information (age, sex, occupation, and income) was collected. The history of T2DM, including duration, oral hypoglycemic agent, insulin injection, was documented. The past history, including hypertension, hyperlipidemia, coronary heart disease, intracoronary stent implantation, myocardial infarction, and stroke, was recorded in details. Vital signs in addition to body weight and height were documented. The work-up including blood bio-chemical test, glycated hemoglobin (HbA1c), urinary albumin excretion rates (UAER), and serum creatinine (CCr) was collected from electrical chart. Fundus photograph, staging for diabetic retinopathy (DR), and index for diabetic macular edema (DME) for each subject were documented.
Hearing test
With routine physical examination in otology, we first confirmed the normal condition of external ear canal and tympanic membrane. A battery of hearing test, including pure tune average (0.5, 1, 2, and 4 kHz), impedance, DPOAE and ABR, were performed.
-
1.
Pure-tone audiometry was determined with an audiometer (Otometrics Conera). Bilateral air conduction thresholds between 0.25 and 8 kHz (0.25, 0.5, 1, 2, 4, 8 kHz) and bone conduction thresholds between 0.5 and 4 kHz (0.5, 1, 2, 4 kHz) were obtained through standard audiometric assessment conducted by a qualified audiologist in a sound-proof booth.
-
2.
Tympanograms were recorded utilizing a 226 Hz probe frequency with a middle-ear analyzer (GSI Tympstar Pro). The ear canal air pressure was swept in a positive-to-negative direction (from 400 to −200 dapa) at a rate of 200 daPa/s. The acoustic reflex thresholds were also bilaterally obtained at the frequency of 1 kHz.
-
3.
Distortion product otoacoustic emissions (DPOAEs) were measured using the otoacoustic emission equipment (Otodynamics ILO96) in a sound-proof booth. Two primary brief tones at frequencies f1 and f2 were used in the test procedure. The level and the frequency ratio of the primaries were kept constant, the ratio of the two frequencies f2/f1 = 1.22, and the intensity of L1 = 65 and L2 = 55 dB SPL. The measurements of 2f1–f2 distortion products were made at frequency range of 0.7 k–6 kHz, including 0.7 k, 1 k, 1.5 k, 2 k, 3k, 4 k, 6 kHz were selected.
-
4.
Auditory brainstem response (ABR) was recorded with an evoked potential system (Interacoustics Eclipse). The ABR measurements were performed in an electromagnetic shielding sound-proof booth, using 2000 clicks of alternating polarity and 0.1 millisecond duration. Potentials were evoked by 80 dB hearing level (HL) clicks, presented monaurally at a rate of 20.7 per second. The ABR threshold was also sought by lowering the stimulus intensity until the wave V disappeared. The band-pass filters were set from 0.3 to 3 kHz. The latency of each peak including wave I, III, and V were measured.
Determine which category the recorded DPOAEs fall into:
-
a.
If the recorded DPOAE meets the SNR criteria for detection and falls within the normal range, it would be “present and normal”, marked as “0”.
-
b.
If the recorded DPOAE meets the SNR criteria for detection, but is below the normal range, it would be categorized as “present, but abnormal”, marked as “1”.
-
c.
If the recorded DPOAE does not meet the SNR criteria, it would be categorized as “absent”, marked as “2”.
Blood sample and genome-wide DNA methylation sequencing
DNA extraction
Genomic DNA was isolated from the 2 mL peripheral blood samples taken from individuals by following the manufacturer’s standard procedure using DNeasy Blood & Tissue Kit (QIAGEN, Hilden, Germany). Then DNA Purity is tested by calculating the ratio of absorbance at 260 nm to absorbance at 280 nm using Invitrogen Nanodrop Spectrophotometer.
RRBS (Reduced Representation Bisulfite Sequencing) assay was performed as described previously [14]. Two micrograms of genomic DNA were digested by use of restriction endonuclease MspI (New England Biolabs, USA) overnight before being purified using Ampure XP beads (Beckman Coulter, USA). End repairing, A tailing procedure were then performed by use of Klenow (exo-) (New England Biolabs, USA) and the A-tailed DNA fragments were ligated with methylated-adapter. Adapter-attached DNA fragments were separated on 2% agarose gel and gel slice corresponding to 40–220 bp was manually excised and purified with the Minielute gel extraction kit (Qiagen, USA). The purified size-selected DNA was then bisulfite converted by using EZ DNA Methylation-Gold™ Kit (ZYMO, USA) and then amplified by a 15-cycle PCR with Hotstart Taq (Takara, Japan). After being cleaned up by using AMPure XP beads, PCR-amplified RRBS libraries were quantified using Qubit and library size distribution were checked on bioanalyzer 2100. Finally, 10 G of 2 × 150 bp pair end raw data was generated each sample on the Illumina Hiseq 2500 platform. FastQC (http://www.bioinformatics.babraham.ac.uk/projects/fastqc/) was used for the quality control of the raw data. Using Bismark (http://www.bioinformatics.babraham.ac.uk/projects/bismark/), the adapter-trimmed and quality-filtered clean reads were aligned to the bisulfite converted reference genome hg19 and the methylation level of cytosine in CpG, CHG (where H = A, T, or C) and CHH (where H = A, T, or C) context were calculated separately, through which the methylation levels of CpG island (CPGI), gene (GENE), and transcriptional start site (TSS) regions were also calculated. SeqMonk (http://www.bioinformatics.bbsrc.ac.uk/projects/seqmonk/) was used to calculate the methylation level according to the distribution of CPGI, GENE, and TSS. Genes associated with the cytosine sites and regions with significant methylation difference by t-test were listed and annotated with GO terms and KEGG pathways.
Analysis of DMRs
After removing the NaN data, the detectable regions with the fold-change of DNA methylation ≥2 or ≤0.5, as well as p-value < 0.05 were defined as DMRs. In order to facilitate the gene alignment in the next step, we further defined DMRs in gene regions with significant difference in methylation levels between cases and controls (p < 0.05). The detected DMRs were aligned to two categories of genes, the susceptibility genes of T2DM and deafness genes, respectively. The susceptibility genes of T2DM were referred to recently published GWAS studies [15,16,17,18,19,20,21,22,23]. In all, 138 T2DM susceptibility genes were listed for further analysis.
The deafness genes were referred to the list in the newly updated “Hereditary hearing loss homepage” website http://hereditaryhearingloss.org/ (22nd, Oct. 2017). After removing the repetition, 144 deafness genes were included for further analysis. The loci with unknown gene but with identified location were not included.
Statistical analysis
In order to approve the classification effect of the extracted DMRs, cluster analysis and principal component analysis (PCA) were performed for their DNA methylation profile. All of samples were clustered into two clusters based on Consensus Non-negative Matrix Factorization (CNMF) method. Non-negative matrix factorization (NMF) is an unsupervised, parts-based learning algorithm that has been applied on the analysis of data matrices whose elements are non-negative. NMF is an efficient method for distinct molecular patterns identification and provides a powerful method for class discovery. Here, CancerSubtypes package of R software (http://www.bioconductor.org) was used to implement this analysis. In addition, PCA was used to evaluate the classification performance of the identified DMRs. For the identified DMRs, the first principal component (PC) and the second PC of all samples were used to make the multidimensional scaling graph because these two PCs can explain the larger proportion of variability. The pca3d package of R software (http://www.r-project.org) was used to implement the analysis.
The Pearson correlation analyses were performed between clinical phenotypes (age, DPOAE, HbA1C, UAER and CCr) and the methylation levels at the identified DMRs. Pearson correlations are significant if p < 0.05. The independent t-tests were used to infer the association between KCNJ11 methylation levels and past history, including hypertension, hyperlipidemia, coronary heart disease, intracoronary stent implantation, and myocardial infarction. Statistical analyses were conducted with SPSS 17.0 software (SPSS Inc., Chicago, IL, USA).
Results
DRHL and control group had five cases, respectively. The age ranged from 39 to 63 years old, and the sex ratio was 7:3. BMI ranged from 19.6 to 32.7. The duration of T2DM ranged from 0.5 to 20 years. When compared these basic information between DRHL and control group, no significant difference was found in age, gender, duration of T2DM, and BMI (See Table 1). These results indicated that the basic characteristics of two groups are matched. In order to minimize the effect of compositional difference in blood cells, we compared the white-blood cell counts in the peripheral blood in DRHL cases and controls. No significant difference was found (p = 0.774, see Table 1).
The hearing of DRHL and control subjects
The hearing threshold shifted in the DRHL group, whose audiogram was classified as “metabolic” type. The hearing threshold of PTA in the DRHL and control group displayed significant difference at 0.5–4 kHz (Fig. 1).

The comparison of hearing thresholds of PTA in DRHL and control group in the right ear and in the left ear. (A) For the right ear, the hearing threshold of the DRHL and control group displayed significant difference at 0.5 kHz (p < 0.001), 1 kHz (p = 0.012), 2 kHz (p = 0.030), and 4 kHz (p < 0.001). (B) Similarly, the significant difference of hearing thresholds between DRHL and control was also seen from the left ear at 0.5 kHz (p = 0.019), 1 kHz (p = 0.011), 2 kHz (p = 0.002), and 4 kHz (p < 0.001). One asterisk indicates significant difference (p < 0.05), double asterisks indicate rather significant difference (p < 0.001)
Comparing the detective rate of DPOAE from low to high frequencies (0.7–6 kHz), we found significant difference between the DRHL group and control group (Table 2). On the right ear, except that the difference was significant at 1.5 kHz (p < 0.05), the difference at other frequencies were more remarkable (p < 0.01). The ABR threshold of DRHL group (58.00 ± 13.04 dBHL) differed significantly from that of control group (28.00 ± 4.47 dBHL) in the right ear (p = 0.005 < 0.05). Similarly, in the left ear, the ABR threshold of DRHL group (62.00 ± 8.37 dBHL) was remarkably higher than that of control group (28.00 ± 4.47) (p < 0.001). Since the latencies of wave I in three cases of DRHL were not detectable, I–III or I–V intervals were not comparable.
The identification of DMRs in DRHL
On average, 2 million reads were obtained for each sample, the mapping efficiency were 35.98% and 36.06% for the cases and controls. The mapped reads covered ~636.6 million and ~576.3 million CpG sites from the controls and cases, respectively. A minimum sequencing depth of 30× was applied and CpGs sites covered with at least five reads were used for subsequent analysis. We found the mean level of CpG methylation in controls and cases was 40% and 54.5%, respectively.
The quality control of the raw data was performed with FastQC. The result of FastQC and comprehensive summary of mapping were presented in Supplementary file 1 (“Data statistics.xlsx (31 kb)”).
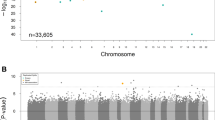
We detected 22,371 CpG island sites. The DNA methylation level in DRHL group and control group differed significantly in 509 CpG sites (2.28%). In gene regions, 40,237 methylation sites were detected. After removing the sites in X-chromosome, 113 gene regions differed significantly in methylation level between DRHL group and control group, which conformed to the definition of DMRs (see Supplementary file 2. “Different_Methylation_Gene.xls” (7550 kb)).
Furthermore, 38 DMRs identified using the whole samples were screened for the analysis of the data quality (See Supplementary file 3. “38 DMR locations.XLS” (34 kb)). Then, cluster analysis was performed to DNA methylation profile of these 38 DMRs. All of samples were clustered into two clusters based on CNMF method. As a powerful classification, all samples were divided into two clusters. Four controls were divided into one cluster whereas five cases and one control were divided into another cluster (Fig. 2a). In another word, the classification accuracy is up to 90%. A higher silhouette score indicates a higher consistency within cluster of data, and we can see that the absolute silhouette scores of two clusters were all more than 0.80 (Fig. 2b). In addition, PCA was used to see the classification performance of the identified differentially DMRs. We can see that the controls and the DRHL patients are separated effectively (Fig. 2c). These results support the effectiveness of the classification based on the DNA methylation profile of 38 identified DMRs.

The classification for samples. a The heatmap for cluster 1 and cluster 2 based on DNA methylation profile of the identified differentially DNA methylation regions. b Silhouette plots for cluster 1 (controls) and cluster 2 (cases). c The classification for samples based on the identified differentially DNA methylation regions using PCA. The yellow circles indicate the DRHL patients whereas the blue snowflakes indicate the control subjects
Alignment to T2DM susceptibility genes and deafness genes
We aligned the 38 DMRs to the 138 T2DM susceptibility genes. After comparing 38 DMRs with 138 T2DM susceptibility genes extracted from literatures, KCNJ11 was found to be the only overlapped gene. No DMRs were aligned to the 144 deafness genes extracted from the newly updated “Hereditary hearing loss homepage” website: http://hereditaryhearingloss.org/.
We can see that KCNJ11 loci showed the higher DNA methylation level in DRHL than in control (p = 0.02, Fig. 3a). The area under curve (AUC) of receiver operating characteristic of KCNJ11 distinguishing DRHL patients from controls is 0.880 (Fig. 3b). It is known that a value of 0.8 for the AUC means that for 80% of the time a random selection from the positive group will have a score greater than a random selection from the negative class. Therefore, the obtained AUC value of 0.880 here indicated that the DNA methylation level of KCNJ11 has a good capability of distinguishing DRHL patients from controls.

The identified differentially methylation site at KCNJ11 which is associated with DRHL. a The DNA methylation level at KCNJ11 in case and control group. b AUC of KCNJ11 to distinguish DRHL patients from controls
Association analysis
At first, we compared the HbA1C between DRHL group and control group. No significant difference was found (p = 0.757). Next, we did association analysis between the methylation level of KCNJ11 and basic information (age, sex, occupation, and income) and the history of T2DM (duration, oral hypoglycemic agent, insulin injection). Age was the risk factor associated with the methylation level of KNJ11 (r = 0.754, p < 0.05).
In order to explore the correlation between methylation level of KCNJ11 and the macro-vascular complication of T2DM, we further analyzed its association with the past history, including hypertension, hyperlipidemia, coronary heart disease, intracoronary stent implantation, myocardial infarction, and stroke. Stroke was associated with the methylation level of KNJ11 (t = 2.595, p < 0.05).
Diabetic nephropathy (DN) and diabetic retinopathy (DR) are the two micro-vascular complications of T2DM. We first compared the level of UAER and CCr, which indicates the severity of DN, between DRHL group and control group. Then we compared the grading of DN and the degree of diabetic macular edema (DME) between DRHL group and control group. No significant difference was found. The methylation level of KCNJ11 was not correlated either to DN or to DR.
Furthermore, we analyzed the correlation between the methylation level of KCNJ11 and the hearing threshold on each ear. Hearing threshold examined with PTA both on the right ear at 0.5, 1, and 2 kHz and on the left ear at 1 and 2 kHz was found to be associated with the methylation level of KCNJ11 (p < 0.05). Particularly, hearing threshold at 2 kHz on both ears was strongly correlated to the methylation level of KCNJ11 (p < 0.01) (Table 3).
Statistically, the detective rate of DPOAE at all detecting frequencies only on the right ear was correlated with the methylation level of KCNJ11 (Table 4). Similarly, the ABR threshold only on the right ear was correlated (r = 0.678, p < 0.05). The latencies of wave I, III, and V were not associated.
Discussions
In our study, the “metabolic” type of hearing loss according to the classification of human audiometric phenotypes of ARHL was referred [13]. We identified 249 CpG sites in which the DNA methylation level in DRHL group and control group differed significantly, namely DMRs.
By clustering the samples with NMF method and analyzing with PCA, 38 DMRs identified with the whole samples were screened for the analysis of the data quality. The phenotype classification accuracy compared to the methylation level is up to 90%. Therefore, the classification of human audiometric phenotypes for “metabolic” type of ARHL is also a good tool to classify the phenotype of DRHL for further analysis.
The precise regulation of DNA methylation is essential for hearing [24]. Klein and his colleagues identified DNA methyltransferase 1 (DNMT1) mutation c.1484A>G(p.Tyr495Cys) in two American and one Japanese kindreds and a triple nucleotide change c.1470-1472TCC>ATA(p.Asp490Glu-Pro491Tyr) in one European kindred, which caused one form of hereditary sensory and autonomic neuropathy (HSAN1) with dementia and hearing loss [25]. In the progressive hearing loss animal model DBA/2J mice, it was found that the expression levels of all three Dnmts (Dnmt1, Dnmt3a, and Dnmt3b) were the highest at postnatal day (P)1 and had decreased by P14. The lowest levels were present at 12 weeks. Treated with l-methionine (MET), a methyl donor, the DBA/2J mice showed a significantly improved hearing [26].
How does hyperglycemia lead to hearing loss via DNA methylation? By aligning the 38 DMRs to the 138 T2DM susceptibility genes, KCNJ11 was found to be the only gene. No DMRs were aligned to the 144 deafness genes (http://hereditaryhearingloss.org/). DRHL is more regarded as a newly-recognized complication of T2DM.
The complications of T2DM are divided into two types: macro-vascular complication and micro-vascular complications. Hence, we did association analysis between the methylation level of KCNJ11 and macro-vascular complications, including hypertension, hyperlipidemia, coronary heart disease, intracoronary stent implantation, myocardial infarction, and stroke in addition to micro-vascular complications, DR and DN. Stroke was the only complication found to be associated with the methylation level of KCNJ11. A larger sample size is required to identify if DRHL belongs to macro- or micro-vascular complication of T2DM.
KCNJ11 (kir6.2) is a member in the inward rectifying potassium (Kir) channels. Assembly of an inward rectifier K+ channel pore (Kir6.1/Kir6.2) and an adenosine triphosphate (ATP)-binding regulatory subunit (SUR1/SUR2A/SUR2B) forms ATP-sensitive K+ (KATP) channel heteromultimers, widely distributed in metabolically active tissues throughout the body. KATP channels are metabolism-gated biosensors functioning as molecular rheostats that adjust membrane potential-dependent functions to match cellular energetic demands. Vital in the adaptive response to (patho)physiological stress, KATP channels serve a homeostatic role ranging from glucose regulation to cardioprotection. Pathogenic mutations in KCNJ11 lead to congenital hyperinsulinism, developmental delay, epilepsy, and neonatal diabetes (DEND) syndrome or transient neonatal diabetes [27]. Beyond neonatal diabetes mellitus, KCNJ11 is also a maturity-onset of the young (MODY) gene (‘MODY13’). MODY is a clinically heterogeneous form of diabetes characterized by an autosomal-dominant mode of inheritance, and onset before the age of 25 years, and a primary defect in the pancreatic beta-cell function [28].
By mapping the sequences of transcripts from a human fetal cochlear cDNA library and a mouse organ of Corti cDNA library, Gabashvili and his colleagues [29] identified KCNJ11 as an ion channel gene expressed in the inner ear with evidence from microarray. The spatial and temporal expression of KCNJ11 in the mammalian inner ear is, however, still unclear.
In the family of the inward rectifying potassium (Kir) channels, KCNJ10 (Kir4.1) is relatively well investigated in the maintenance of the inner ear normal function. Kir4.1 has two distinct aspects of extracellular K+ homeostasis: First, it participates in the generation and maintenance of EP and high K+ concentration in the endolymph inside the scala media. Second, Kir4.1 is the major K+ channel in satellite glial cells surrounding spiral ganglion neurons to sink K+ ions expelled by the ganglion neurons during excitation. Kir4.1 deficiency leads to hearing loss with the absence of EP and spiral ganglion neuron degeneration [30].
Due to homologous sequences of Kir6.2 and Kir4.1, we therefore hypothesize that Kir6.2 is also required to maintain the K+ homeostasis in the mammalian inner ear. Failure to maintain the K+ homeostasis could have a crucial role in the hyperglycemia-induced hearing loss. Jacobs et al. recorded stimulus-frequency otoacoustic emission (SF OAE) for people with T2DM in a glucose tolerance test. Mean SF OAE amplitudes were elevated following glucose consumption, particularly 1 h after glucose consumption [31]. In our previous study, we interpreted that the acute hyperglycemia had caused the metabolism stress on the cells within the cochlea before any pathological change of vascular and/or neural system. In this case, OAE can embody the sub-clinical cochleopathy when PTA is still normal or slightly shifted [7].
There are some limitations of our study for which the explanations should not be avoided. First of all, our study used a relatively small sample size. The five cases of DRHL and five controls, however, were strictly selected out of >1000 hospitalized patients with rigorous inclusion and exclusion criteria. The basic characteristics including age, sex, BMI, duration of T2DM and white-blood cell counts are all well matched (Table 1). High quality of the selected subjects is to ensure the accuracy of phenotype and the following results. The cluster analysis based on the DNA methylation profile indicated that the classification accuracy is up to 90.0% (Fig. 2). Meanwhile, a larger sample size is set in our further investigations. Secondly, age was found to be the risk factor of DRHL in our study. Wolber and his colleagues [32] found that hearing ability was strongly associated with DNA methylation levels in the promoter regions of several genes in the population with age-related hearing impairment. Diabetics over 65 years old were excluded in our study. In addition, the age in DRHL group and control group were matched. The affection of age in our study has been minimized. Age, however, can be a risk factor for the metabolism of inner ear. Thus, it increases the risk of DRHL. A larger sample size is needed to verify this risk factor.
All in all, DNA methylation profile indicates the susceptibility loci of DRHL. The potassium metabolism may have a critical role in the hearing loss caused by hyperglycemia. Further investigation on the underlying mechanism of hearing loss induced by acute and chronic hyperglycemia is required. This study would shed light on the design of new targeted pharmaceuticals for the treatment of DRHL. It is rather promising to study further if glibenclamide, an antidiabetic drug in a class of medications known as sulfonylureas, can protect hearing by blocking the KATP channel composed of SUR1 and Kir6.2 [33].
References
Bainbridge KE, Hoffman HJ, Cowie CC. Diabetes and hearing impairment in the United States: audiometric evidence from the National Health and Nutrition Examination Survey, 1999 to 2004. Ann Intern Med. 2008 ;149:1–10.
Cheng YJ, Gregg EW, Saaddine JB, Imperatore G, Zhang X, Albright AL. Three decade change in the prevalence of hearing impairment and its association with diabetes in the United States. Prev Med. 2009;49:360–4.
Sakuta H, Suzuki T, Yasuda H, Ito T. Type 2 diabetes and hearing loss in personnel of the self-defense forces. Diabetes Res Clin Pract. 2007;75:229–34.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317:2515–23.
Xu GC, Luo Y, Li Q, Wu MF, Zhou ZJ. Standardization of type 2 diabetes outpatient expenditure with bundled payment method in China. Chin Med J. 2016;129:953–9.
Chen XB, Tang L, Chen HY, Zhao LY, Hu SL. Assessing the impact of complications on the costs of type 2 diabetes in urban China. Chinese. J Diabetes. 2003;11:238–41.
Hao J, Fu X, Zhang C, Zhang X, Zhao S, Li Y. Early detection of hearing impairment in patients with diabetes mellitus with otoacoustic emission. A systematic review and meta-analysis. Acta Otolaryngol. 2017;137:179–85.
Multhaup ML, Seldin MM, Jaffe AE, Lei X, Kirchner H, Mondal P, et al. Mouse-human experimental epigenetic analysis unmasks dietary targets and genetic liability for diabetic phenotypes. Cell Metab. 2015;21:138–49.
Sapienza C, Lee J, Powell J, Erinle O, Yafai F, Reichert J, et al. DNA methylation profiling identifies epigenetic differences between diabetes patients with ESRD and diabetes patients without nephropathy. Epigenetics. 2011;6:20–8.
Feinberg AP, Irizarry RA. Evolution in health and medicine Sackler colloquium: stochastic epigenetic variation as a driving force of development, evolutionary adaptation, and disease. Proc Natl Acad Sci USA 2010;107(Suppl 1):1757–64.
Toperoff G, Aran D, Kark JD, Rosenberg M, Dubnikov T, Nissan B, et al. Genome-wide survey reveals predisposing diabetes type 2-related DNA methylation variations in human peripheral blood. Hum Mol Genet. 2012;21:371–83.
American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care. 2017;40(Suppl 1):S11–S24.
Dubno JR, Eckert MA, Lee FS, Matthews LJ, Schmiedt RA. Classifying human audiometric phenotypes of age-related hearing loss from animal models. J Assoc Res Otolaryngol. 2013;14:687–701.
Gu H, Smith ZD, Bock C, Boyle P, Gnirke A, Meissner A. Preparation of reduced representation bisulfite sequencing libraries for genome-scale DNA methylation profiling. Nat Protoc. 2011;6:468–81.
Prokopenko I, McCarthy MI, Lindgren CM. Type 2 diabetes: new genes, new understanding. Trends Genet. 2008;24:613–21.
Voight BF, Scott LJ, Steinthorsdottir V, Morris AP, Dina C, Welch RP, et al. Twelve type 2 diabetes susceptibility loci identified through large-scale association analysis. Nat Genet. 2010;42:579–89.
Bonnefond A, Froguel P, Vaxillaire M. The emerging genetics of type 2 diabetes. Trends Mol Med. 2010;16:407–16.
Ridderstråle M, Groop L. Genetic dissection of type 2 diabetes. Mol Cell Endocrinol. 2009;297:10–7.
Morris AP, Voight BF, Teslovich TM, Ferreira T, Segrè AV, Steinthorsdottir V. et al. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet. 2012;44:981–90.
Cho YS, Chen CH, Hu C, Long J, Ong RT, Sim X, et al. Meta-analysis of genome-wide association studies identifies eight new loci for type 2 diabetes in east Asians. Nat Genet. 2011;44:67–72.
Hara K, Fujita H, Johnson TA, Yamauchi T, Yasuda K, Horikoshi M, et al. Genome-wide association study identifies three novel loci for type 2 diabetes. Hum Mol Genet. 2014;23:239–46.
DIAbetes Genetics Replication And Meta-analysis (DIAGRAM) Consortium; Asian Genetic Epidemiology Network Type 2 Diabetes (AGEN-T2D) Consortium; South Asian Type 2 Diabetes (SAT2D) Consortium; Mexican American Type 2 Diabetes (MAT2D) Consortium; Type 2 Diabetes Genetic Exploration by Nex-generation sequencing in muylti-Ethnic Samples (T2D-GENES) Consortium, Mahajan A, et al. Genome-wide trans-ancestry meta-analysis provides insight into the genetic architecture of type 2 diabetes susceptibility. Nat Genet. 2014;46:234–44.
Ayub Q, Moutsianas L, Chen Y, Panoutsopoulou K, Colonna V, Pagani L, et al. Revisiting the thrifty gene hypothesis via 65 loci associated with susceptibility to type 2 diabetes. Am J Hum Genet. 2014;94:176–85.
Moore LD, Le T, Fan G. DNA methylation and its basic function. Neuropsychopharmacology. 2013;38:23–38.
Klein CJ, Botuyan MV, Wu Y, Ward CJ, Nicholson GA, Hammans S, et al. Mutations in DNMT1 cause hereditary sensory neuropathy with dementia and hearing loss. Nat Genet. 2011;43:595–600.
Mutai H, Miya F, Fujii M, Tsunoda T, Matsunaga T. Attenuation of progressive hearing loss in DBA/2J mice by reagents that affect epigenetic modifications is associated with up-regulation of the zinc importer Zip4. PLoS ONE. 2015;10:e0124301.
Olson TM, Terzic A. Human K(ATP) channelopathies: diseases of metabolic homeostasis. Pflug Arch. 2010;460:295–306.
Bonnefond A, Philippe J, Durand E, Dechaume A, Huyvaert M, Montagne L, et al. Whole-exome sequencing and high throughput genotyping identified KCNJ11 as the thirteenth MODY gene. PLoS ONE. 2012;7:e37423.
Gabashvili IS, Sokolowski BH, Morton CC, Giersch AB. Ion channel gene expression in the inner ear. J Assoc Res Otolaryngol. 2007;8:305–28.
Chen J, Zhao HB. The role of an inwardly rectifying K(+) channel (Kir4.1) in the inner ear and hearing loss. Neuroscience. 2014;265:137–46.
Jacobs PG, Konrad-Martin D, McMillan GP, McDermott D, Fausti SA, Kagen D, et al. Influence of acute hyperglycemia on otoacoustic emissions and the medial olivocochlear reflex. J Acoust Soc Am. 2012;131:1296–306.
Wolber LE, Steves CJ, Tsai PC, Deloukas P, Spector TD, Bell JT, et al. Epigenome-wide DNA methylation in hearing ability: new mechanisms for an old problem. PLoS ONE. 2014;9:e105729.
Martin GM, Yoshioka C, Rex EA, Fay JF, Xie Q, Whorton MR, et al. Cryo-EM structure of the ATP-sensitive potassium channel illuminates mechanisms of assembly and gating. Elife. 2017;6:e24149.
Acknowledgements
We appreciate the support of all the patients and their relatives in our study. Without their understanding and generous contribution, this study cannot be implemented. We also thank HXJ for screening charts in the electrical chart system, which is a tremendous working load. We are grateful that HXL, WMX, CHL and their colleagues have undertaken a great amount of lab work (Genesky Biotechnologies Inc., Shanghai, China, 201315). This work was supported by Basic-Clinical Cooperation Program from Capital Medical University (No. 16JL58) for Dr. Jin Hao.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Co-corresponding author: Yongxin Li
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Hao, J., Hua, L., Fu, X. et al. Genome-wide DNA methylation analysis of human peripheral blood reveals susceptibility loci of diabetes-related hearing loss. J Hum Genet 63, 1241–1250 (2018). https://doi.org/10.1038/s10038-018-0507-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s10038-018-0507-y
This article is cited by
-
Diabetes-induced auditory complications: are they preventable? a comprehensive review of interventions
European Archives of Oto-Rhino-Laryngology (2021)
