
Abstract
We compared three benidipine-based regimens—that is, benidipine plus angiotensin receptor blocker (ARB), β-blocker (BB) or thiazide—and found that the benidipine–BB combination was less beneficial in reducing the risk of stroke than the benidipine–thiazide combination. This sub-analysis sought to compare the effects of reaching a target blood pressure (BP) (<140/90 mm Hg) on the cardiovascular outcomes among the three benidipine-based treatment groups in the Combination Therapy of Hypertension to Prevent Cardiovascular Events trial. This sub-analysis included 3001 subjects to evaluate the achievement of target BP at a minimum of three points at 6-month intervals of clinical BP measurements during the study period. After randomization, the patients were categorized into two groups on the basis of achieved on-treatment target BP: a good control (GC) group achieving a BP⩾66.7% of the target and a poor control (PC) group with a BP <66.6% of the target. For each of the two control groups, outcomes were compared among the three treatment groups. The event rates for cardiovascular composite endpoints, stroke and hard cardiovascular events were higher in the PC group than the GC group (P=0.041, P=0.042 and P=0.038, respectively). Within the PC group, hazard ratios for the incidence of cardiovascular events were lower in the benidipine–thiazide group than in the benidipine–BB group (composite cardiovascular events: 2.04, P=0.033; stroke: 4.14, P=0.005; and hard cardiovascular events: 3.52, P=0.009). Within the GC group, the incidence of cardiovascular events was not different among the three treatment regimens. The benidipine–thiazide combination may provide better cardiovascular outcomes than the benidipine–BB combination even in patients with poor BP control.
Similar content being viewed by others


Introduction
Previous meta-analyses have shown that anti-hypertensive agents are effective in lowering blood pressure (BP) and preventing cardiovascular events,1, 2, 3, 4, 5, 6 but two or more agents are often required to achieve the target BP,7, 8 and recent clinical guidelines have recommended combination therapy to control BP levels.9, 10, 11 Although the adverse cardiovascular consequences of hypertension largely depend on the absolute BP values,12 current guidelines recommend <140/90 mm Hg as the target level of BP control based on the results of comparative studies.9, 10, 11
The Combination Therapy of Hypertension to Prevent Cardiovascular Events (COPE) trial was the first clinical trial to examine combination therapy with a potent and long-acting dihydropyridine calcium channel blocker (CCB), benidipine, which inhibits not only L-type and N-type calcium channels but also T-type calcium channels,13 for the treatment of hypertension. In this trial, although the percentages of subjects achieving the target BP (<140/90 mm Hg) and the incidences of primary composite cardiovascular endpoints, including the reduction in BP from baseline over the course of the trial, were similar among the benidipine–thiazide diuretic (thiazide), benidipine–angiotensin receptor blocker (ARB) and benidipine–β-blocker (BB) groups, secondary analyses suggested that benidipine combined with a BB was less effective at reducing the risk of stroke compared with the benidipine–thiazide combination.14, 15, 16, 17, 18
Many clinical trials have directly compared the effects of anti-hypertensive medications on BP reduction and cardiovascular outcomes,2, 3, 4, 5, 6 but there is little evidence concerning the effects of anti-hypertensive medications on these indices in patients with hypertension who do not achieve the target BP. Further, there are no data on the cardiovascular outcome of combination therapy in patients who do not achieve the target BP. In the present study, therefore, we analyzed the data on patients with hypertension who were enrolled in the COPE trial and who did not achieve the target BP following monotherapy with benidipine at a dose of 4 mg per day. We categorized these patients on the basis of their on-treatment BPs to assess the impact of not achieving the target BP (⩾140 mm Hg) compared with achieving the target BP (<140/90 mm Hg) on cardiovascular outcome among the three benidipine-based treatment groups in the COPE trial.
Methods
Study design
The COPE trial was an investigator-initiated multi-center study with a prospective, randomized, open-label, blinded-endpoint design that compared cardiovascular effects and the achievement of a target BP (<140/90 mm Hg) between three dihydropyridine-type CCB benidipine-based regimens (ARB, BB or thiazide) in 3501 hypertensive patients who had not achieved the target BP with benidipine alone at a dose of 4 mg per day. The BP management titration algorithm, together with other details of the study design, and the results of the COPE trial have already been reported.14, 15 In brief, participants aged 40–85 years with a sitting systolic BP of 140 mm Hg or more and/or a diastolic BP of 90 mm Hg or more, whether untreated or treated, who did not achieve the target BP at our clinic following monotherapy with benidipine at a dose of 4 mg per day during the run-in phase (4–8 weeks) were included in the study. These patients were randomly assigned to receive benidipine combined with an ARB, a BB or a thiazide. After the randomization, all patients were followed every 6 months for at least 36 months (BP measurement phase). The BP was measured at randomization (baseline), at monthly intervals to achieve the target BP after randomization (drug titration phase), and every 6 months thereafter according to the guidelines for the management of hypertension.19 Mean on-treatment BP measurements were obtained at 6-month intervals from 6 months of the study treatment onwards.
The primary composite cardiovascular events consisted of the following groups: subjects with sudden death, fatal or non-fatal stroke, fatal or non-fatal myocardial infarction, hospitalization due to unstable angina, new onset of heart failure (New York Heart Association class II–IV), new onset or worsening of peripheral arterial disease, and renal events (defined as serum creatinine level doubled to over 2 mg dl−1, serum creatinine ⩾4.0 mg dl−1 or renal dialysis). The secondary endpoints were defined as all-cause mortality, death from cardiovascular events, hard composite cardiovascular events (cardiovascular death, non-fatal myocardial infarction and non-fatal stroke excluding transient ischemic attack) and new onset of diabetes.
Data analysis
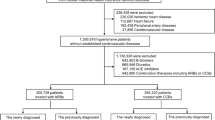
A total of 3293 patients who were prescribed a combination treatment (1110, benidipine–ARB; 1089, benidipine–BB; 1094, benidipine–thiazide) were compared using full set analysis to specifically evaluate the effects of benidipine-based combination therapy for hypertension in the COPE trial.15 BP measured on six occasions from 6 to 36 months after randomization was used to determine the achievement of target BP during the 3-year BP measurement phase from 6-month interval clinic BP measurements during the study period. After excluding 292 patients who were missing BP values for at least four out of the six measurement time points, 3001 patients (1031, benidipine–ARB; 975, benidipine–BB; 995, benidipine–thiazide) were eligible for the present study. The median percentage of target BP achieved in the subjects in this sub-analysis was 66.7%, and the previous results on the visit-to-visit BP variability in the post-hoc analysis of the COPE trial showed that lower visit-to-visit BP variability may be important for better outcomes.18 In consideration of all of these results on the BP control, we categorized the sub-analysis subjects into two groups based on whether they achieved on-treatment target BP of at least four points of the mean on-treatment BPs obtained at 6-month intervals from 6 months of study treatment onwards: the good control (GC) group was defined as patients who achieved a target BP⩾66.7%, and the poor control (PC) group was defined as patients who achieved target BP<66.6% from 6 months of study treatment onwards (Figure 1). The median follow-up period was 3.67 years after randomization, and 3.1 years after the 6-month visit.

Flow diagram of the study participants. ARB, angiotensin receptor blocker; BB, β-blocker; TD, thiazide diuretic.
Statistical analysis
Patient characteristics were reported as the mean±s.d. or percentage. Continuous variables were compared with Student’s t-tests or one-way analysis of variance, as appropriate. Categorical variables were compared with the χ2-test. Survival curves were generated by the Kaplan–Meier method for primary composite cardiovascular events and secondary cardiovascular events among the three treatment groups. Survival curves were compared using the log-rank test. Hazard ratios (HRs) and confidence intervals were calculated using the Cox proportional hazards model. All data were analyzed using SAS System Release 9.1 (SAS Institute, Cary, NC, USA). All reported P-values are two-sided.
Results
Data on the demographic and baseline characteristics showed that the body mass index, systolic and diastolic BPs, diabetes, total anti-hypertensive agents, benidipine, ARB and anti-diabetic agents were significantly higher in the PC group than the GC group (Table 1). Others characteristics were well-matched between the two groups in this sub-analysis of the COPE trial. In addition, within the GC group all of the demographic and baseline characteristics were well-matched among the three randomized groups, with the exception that the percentage of angiotensin-converting enzymes was significantly higher in the benidipine–BB group than the other two groups (Table 2).
The reduction in BP from baseline was similar among the three treatment groups in both the GC and PC groups over the course of the trial (Figure 2). At the end of the BP measurement phase, the mean average BPs in the GC and PC groups were ~128/74 mm Hg and 142/80 mm Hg, respectively. The average BP did not differ among the three treatment groups in either the GC or PC subjects. Moreover, the percentage of patients who achieved the target BP did not differ among the three treatment groups in either the GC or PC subjects, whereas the percentage of patients who achieved the target BP was higher in the GC group than in the PC group (85.9 vs. 36.1%).

Effects of treatment on mean systolic and diastolic BP and achievements of target BP. ARB, angiotensin receptor blocker; BB, β-blocker; BP, blood pressure; TD, thiazide diuretic. Data of the proportions of target blood pressure are shown as percentage of patients. Achievement rate is the proportion of patients achieving target BP (systolic BP<140 mm Hg and diastolic BP<90 mm Hg).
Trends in the concomitant medications did not appear to differ among the three treatment groups in either the GC or PC subjects (Supplementary Table S1). However, at the 36-month follow-up, the concomitant use of lipid-lowering agents and statins was significantly higher in the PC group than the GC group (Supplementary Table S2).
Hazzard ratios
The event rates for the primary composite cardiovascular events, hard composite cardiovascular events and stroke were significantly higher in the PC group than in the GC group (Table 3): the HRs of primary composite cardiovascular events, hard composite cardiovascular events, and stroke were significantly higher in the benidipine–BB group than in the benidipine–thiazide group of the PC group, whereas they did not differ among the three treatment groups of the GC group. We further calculated the HRs by the multi-adjusted and adjusted with the systolic BP with time-dependent covariates in this sub-analysis for the primary composite cardiovascular events, hard composite cardiovascular events and stroke (Supplementary Table S3), demonstrating that the results of this sub-analysis of the COPE trial confirmed that the influence of the BP difference among the three treatment groups in the PC group on outcomes was negligible. In contrast, compared with the benidipine–ARB group, the HR of the incidence of new-onset diabetes was significantly higher in the benidipine–BB group than in the other two treatment groups in the GC group, whereas it did not differ among the three treatment groups of the PC group (Figure 3). In contrast, the HRs of cardiac events and all-cause mortality were not different among the three treatment groups in both the GC and PC groups.

Hazard ratios for primary and secondary endpoints. A primary composite cardiovascular events consisted of the following groups: sudden death; fatal or non-fatal stroke; fatal or non-fatal myocardial infarction; hospitalization due to unstable angina; new onset of heart failure (New York Heart Association class II–IV); new onset or worsening of peripheral arterial disease; and renal events (defined as serum creatinine level doubled to over 2 mg dl−1, serum creatinine ⩾4.0 mg dl−1 or renal dialysis). Hard composite cardiovascular events consist of cardiovascular death, fatal or non-fatal myocardial infarction and stroke excluding TIA. ARB, angiotensin receptor blocker; BB, β-blocker; CI, confidence interval; CV, cardiovascular; TD, thiazide diuretic; TIA, transient ischemic attack.
Primary and secondary outcomes
The survival curves for time to first composite cardiovascular endpoints, hard composite endpoints and stroke in both the PC and GC groups (Figure 4) showed that compared with the benidipine–thiazide group of the PC group, primary composite cardiovascular endpoints (Figure 4a), hard composite cardiovascular events (Figure 4b) and stroke (Figure 4c) were significantly higher only in the benidipine–BB group, whereas the difference in these endpoints among the three treatment groups did not differ in the GC group. The incidence of the primary composite cardiovascular endpoints, hard composite cardiovascular events and stroke in the benidipine–ARB group was higher than in the benidipine–thiazide group and lower than the benidipine–BB group, but the incidence of these endpoints in the benidipine–ARB regimen did not differ from the benidipine–thiazide or the benidipine–BB group in both the PC and GC groups (Figure 4).

Kaplan–Meier curves for time to first primary and secondary endpoint. Primary composite cardiovascular events: sudden death, fatal or non-fatal stroke, fatal or non-fatal myocardial infarction, hospitalization due to unstable angina, new onset of heart failure (New York Heart Association class II–IV), new onset or worsening of peripheral arterial disease, and renal events (defined as serum creatinine level doubled to over 2 mg dl−1, serum creatinine ⩾4.0 mg dl−1, or renal dialysis). Hard composite cardiovascular events; cardiovascular death, non-fatal myocardial infarction and non-fatal stroke excluding transient ischemic attack. ARB, angiotensin receptor blocker; BB, β-blocker; CV, cardiovascular; TD, thiazide diuretic; TIA, transient ischemic attack.
Adverse events
The percentage of total adverse events was similar in both the PC and GC groups: 613 (48.3%) and 613 (48.3%) patients reported adverse events, respectively (Supplementary Table S4). In addition, the percentage of total adverse events was also similar among the three treatment groups in both the PC and GC groups (Supplementary Table S4). In the PC group, the following adverse events were more frequent than in the GC group: increased glycosylated hemoglobin (1.6 and 0.6%; P<0.012); proteinuria (1.5 and 0.7%; P=0.031); cardiac failure (0.9 and 0.2%; P<0.006); and thrombotic stroke (0.7 and 0.1%; P=0.008), as shown in Supplementary Table S4.
Discussion
The most important and surprising findings in this sub-analysis from the COPE trial were that the benidipine–thiazide combination may provide better cardiovascular outcome than the benidipine–BB combination even in patients with poor BP control, whereas no significant differences on cardiovascular outcome were observed among the three benidipine-based combinations in the patients with good BP control.
Current guidelines for the management of hypertension9, 11, 20 recommend a BP<140/90 mm Hg as a target BP to reduce the incidence of cardiovascular disease. In this sub-analysis, we confirm that the achievement of this target BP is important and that the three allocated classes of anti-hypertensive agents used in the COPE trial are suitable for the CCB, benidipine-based combination to reduce the incidence of cardiovascular disease when sufficiently achieving the target BP. In contrast, when the target BP is insufficiently achieved throughout the BP measurement phase by the benidipine-based combinations, the benidipine–thiazide regimen may be better to prevent the incidence of cardiovascular outcome than the benidipine–BB regimen even if the mean BPs are higher than the target BP. We recently reported that the benidipine–thiazide combination may reduce intra-individual visit-to-visit BP variability more than the benidipine–BB combination,18 suggesting that visit-to-visit BP variability is greater when mean BP is higher.21 These findings indicate that even when target BP is insufficiently achieved, the reduction of intra-individual visit-to-visit BP variability may be important to reduce cardiovascular events in patients with hypertension.
In this sub-analysis of the COPE trial, the mean average BPs at the end of the BP measurement phase in the GC and PC groups were ~128/74 mm Hg and 142/80 mm Hg, respectively. In addition, the cardiovascular event rates for the benidipine–thiazide combination in the PC group were similar to the cardiovascular event rates for this combination in the GC group (Figure 4). Recently, the SPRINT Research Group22 reported that among patients at high risk for cardiovascular events but without diabetes, targeting a systolic BP <120 mm Hg, compared with <140 mm Hg, resulted in lower rates of fatal and non-fatal major cardiovascular events and death from any cause, although significantly higher rates of some adverse events were observed in the intensive-treatment group. In their study, the drugs were mainly dihydropyridine-type CCBs, angiotensin-converting enzyme inhibitors or ARBs, and diuretics and the mean systolic BP at 1 year was 121.4 mm Hg in the intensive-treatment group and 136.2 mm Hg in the standard-treatment group. Although the COPE trial15 mainly included lower-risk patients with fewer cardiovascular complications compared with those in the SPRINT research,22 the SPRINT sub-analysis also showed lower rates of fatal and non-fatal major cardiovascular events in the GC group, indicating that the results of our sub-analysis may support the results of the SPRINT research.22 Moreover, the benidipine–thiazide combination may result in better cardiovascular outcomes in hypertensive patients compared with the benidipine–BB combination, when the target BP was insufficiently achieved.
Study limitations
We adopted the prospective, randomized, open-label, blinded-endpoint design and the sample size and cardiovascular events of this sub-analysis of the COPE trial were relatively small,15, 16, 17, 23 which could have induced a bias and led to chance findings. Because combination therapies are often needed for high-risk patients,21 the optimal combination in mildly to moderately hypertensive patients should be investigated in future clinical trials. In addition, this sub-analysis of a randomized trial was not specifically designed to test various BP targets. Moreover, the results are applicable only to hypertensive patients 40–85 years of age with a BP of ⩾140/90 after benidipine-based monotherapy at entry. In addition, the number of visits in the COPE trial varied among patients (a minimum of three visits was required), although the mean number of BP measurements per patient did not differ significantly between the 3 treatment groups during the 36-month BP measurement phase.
Conclusions
In this sub-analysis of the COPE trial, the benidipine–thiazide combination provided better cardiovascular outcome than the benidipine–BB combination even in subjects with poor BP control. Indeed, we demonstrated that this combination may be better not only for lowering the BP level but also for reducing stroke and other cardiovascular events compared with the benidipine–BB combination. This may be true even in patients who have insufficiently achieved the target BP (⩾140/90 mm Hg). Hence, this combination may provide better cardiovascular outcomes, especially in terms of stroke incidence, in hypertensive patients. However, the reduction of BP and the achievement of target BP and cardiovascular outcomes in the benidipine–ARB combination group did not differ from those of the other two treatment regimens. Although recent guidelines recommend the combination of CCBs and thiazide diuretics,9, 11, 20 this combination is not widely used in current clinical practice. In fact, only four studies on this combination have been reported,15, 24, 25, 26 and a meta-analysis of the results showed a significant risk reduction for myocardial infarction and stroke compared with other combinations, whereas the effectiveness of this therapy was similar to that of other combinations in terms of reducing the risk of all-cause and cardiovascular mortality.27 Further studies to evaluate the CCB-thiazide combination and the incidence of stroke in comparison with other drug combinations will be needed to confirm the results of the present study.
References
Lindholm LH, Carlberg B, Samuelsson O . Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. Lancet 2005; 366: 1545–1553.
Staessen JA, Li Y, Thijs L, Wang JG . Blood pressure reduction and cardiovascular prevention: an update including the 2003-2004 secondary prevention trials. Hypertens Res 2005; 28: 385–407.
Sundstrom J, Arima H, Jackson R, Turnbull F, Rahimi K, Chalmers J, Woodward M, Neal B, Blood Pressure Lowering Treatment Trialists C. Effects of blood pressure reduction in mild hypertension: a systematic review and meta-analysis. Ann Intern Med 2015; 162: 184–191.
Czernichow S, Zanchetti A, Turnbull F, Barzi F, Ninomiya T, Kengne AP, Lambers Heerspink HJ, Perkovic V, Huxley R, Arima H, Patel A, Chalmers J, Woodward M, MacMahon S, Neal B, Blood Pressure Lowering Treatment Trialists C. The effects of blood pressure reduction and of different blood pressure-lowering regimens on major cardiovascular events according to baseline blood pressure: meta-analysis of randomized trials. J Hypertens 2011; 29: 4–16.
Turnbull F, Neal B, Ninomiya T, Algert C, Arima H, Barzi F, Bulpitt C, Chalmers J, Fagard R, Gleason A, Heritier S, Li N, Perkovic V, Woodward M, MacMahon S, Blood Pressure Lowering Treatment Trialists C. Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomised trials. BMJ 2008; 336: 1121–1123.
Sundstrom J, Arima H, Woodward M, Jackson R, Karmali K, Lloyd-Jones D, Baigent C, Emberson J, Rahimi K, MacMahon S, Patel A, Perkovic V, Turnbull F, Neal B, Blood Pressure Lowering Treatment Trialists C. Blood pressure-lowering treatment based on cardiovascular risk: a meta-analysis of individual patient data. Lancet 2014; 384: 591–598.
Koshy S, Bakris GL . Therapeutic approaches to achieve desired blood pressure goals: focus on calcium channel blockers. Cardiovasc Drugs Ther 2000; 14: 295–301.
Sever PS, Messerli FH . Hypertension management 2011: optimal combination therapy. Eur Heart J 2011; 32: 2499–2506.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ishimitsu T, Ito M, Ito S, Itoh H, Iwao H, Kai H, Kario K, Kashihara N, Kawano Y, Kim-Mitsuyama S, Kimura G, Kohara K, Komuro I, Kumagai H, Matsuura H, Miura K, Morishita R, Naruse M, Node K, Ohya Y, Rakugi H, Saito I, Saitoh S, Shimada K, Shimosawa T, Suzuki H, Tamura K, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Umemura S, Japanese Society of Hypertension Committee for Guidelines for the Management of H. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens Res 2014; 37: 253–387.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F, Redon J, Dominiczak A, Narkiewicz K, Nilsson PM, Burnier M, Viigimaa M, Ambrosioni E, Caufield M, Coca A, Olsen MH, Schmieder RE, Tsioufis C, van de Borne P, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Clement DL, Coca A, Gillebert TC, Tendera M, Rosei EA, Ambrosioni E, Anker SD, Bauersachs J, Hitij JB, Caulfield M, De Buyzere M, De Geest S, Derumeaux GA, Erdine S, Farsang C, Funck-Brentano C, Gerc V, Germano G, Gielen S, Haller H, Hoes AW, Jordan J, Kahan T, Komajda M, Lovic D, Mahrholdt H, Olsen MH, Ostergren J, Parati G, Perk J, Polonia J, Popescu BA, Reiner Z, Ryden L, Sirenko Y, Stanton A, Struijker-Boudier H, Tsioufis C, van de Borne P, Vlachopoulos C, Volpe M, Wood DA . 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013; 34: 2159–2219.
Go AS, Bauman MA, Coleman King SM, Fonarow GC, Lawrence W, Williams KA, Sanchez E . An effective approach to high blood pressure control: a science advisory from the American Heart Association, the American College of Cardiology, and the Centers for Disease Control and Prevention. J Am Coll Cardiol 2014; 63: 1230–1238.
Turnbull F, Blood Pressure Lowering Treatment Trialists C. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet 2003; 362: 1527–1535.
Yao K, Nagashima K, Miki H . Pharmacological, pharmacokinetic, and clinical properties of benidipine hydrochloride, a novel, long-acting calcium channel blocker. J Pharmacol Sci 2006; 100: 243–261.
Ogihara T, Matsuzaki M, Matsuoka H, Shimamoto K, Shimada K, Rakugi H, Umemoto S, Kamiya A, Suzuki N, Kumagai H, Ohashi Y, Takishita S, Abe K, Saruta T . The combination therapy of hypertension to prevent cardiovascular events (COPE) trial: rationale and design. Hypertens Res 2005; 28: 331–338.
Matsuzaki M, Ogihara T, Umemoto S, Rakugi H, Matsuoka H, Shimada K, Abe K, Suzuki N, Eto T, Higaki J, Ito S, Kamiya A, Kikuchi K, Suzuki H, Tei C, Ohashi Y, Saruta T, Combination Therapy of Hypertension to Prevent Cardiovascular Events Trial G. Prevention of cardiovascular events with calcium channel blocker-based combination therapies in patients with hypertension: a randomized controlled trial. J Hypertens 2011; 29: 1649–1659.
Ogihara T, Matsuzaki M, Umemoto S, Rakugi H, Matsuoka H, Shimada K, Higaki J, Ito S, Kamiya A, Suzuki H, Ohashi Y, Shimamoto K, Saruta T, Combination Therapy of Hypertension to Prevent Cardiovascular Events Trial G. Combination therapy for hypertension in the elderly: a sub-analysis of the Combination Therapy of Hypertension to Prevent Cardiovascular Events (COPE) Trial. Hypertens Res 2012; 35: 441–448.
Umemoto S, Ogihara T, Rakugi H, Matsumoto M, Kitagawa K, Shimada K, Higaki J, Ito S, Suzuki H, Ohashi Y, Saruta T, Matsuzaki M . Effects of a benidipine-based combination therapy on the risk of stroke according to stroke subtype: the COPE trial. Hypertens Res 2013; 36: 1088–1095.
Umemoto S, Ogihara T, Matsuzaki M, Rakugi H, Ohashi Y, Saruta T, Combination Therapy of Hypertension to Prevent Cardiovascular Events CTG. Effects of calcium channel blocker-based combinations on intra-individual blood pressure variability: post hoc analysis of the COPE trial. Hypertens Res 2016; 39: 46–53.
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H, Japanese Society of Hypertension C. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res 2009; 32: 3–107.
Working Group on the Summit on Combination Therapy for CVD Working Group on the Summit on Combination Therapy for CVD Yusuf S Working Group on the Summit on Combination Therapy for CVD Attaran A Working Group on the Summit on Combination Therapy for CVD Bosch J Working Group on the Summit on Combination Therapy for CVD Joseph P Working Group on the Summit on Combination Therapy for CVD Lonn E Working Group on the Summit on Combination Therapy for CVD McCready T Working Group on the Summit on Combination Therapy for CVD Mente A Working Group on the Summit on Combination Therapy for CVD Nieuwlaat R Working Group on the Summit on Combination Therapy for CVD Pais P Working Group on the Summit on Combination Therapy for CVD Rodgers A Working Group on the Summit on Combination Therapy for CVD Schwalm JD Working Group on the Summit on Combination Therapy for CVD Smith R Working Group on the Summit on Combination Therapy for CVD Teo K Working Group on the Summit on Combination Therapy for CVD Xavier D . Combination pharmacotherapy to prevent cardiovascular disease: present status and challenges. Eur Heart J 2014; 35: 353–364.
Parati G, Ochoa JE, Lombardi C, Bilo G . Assessment and management of blood-pressure variability. Nat Rev Cardiol 2013; 10: 143–155.
SPRINT Research Group SPRINT Research Group Wright JT Jr SPRINT Research Group Williamson JD SPRINT Research Group Whelton PK SPRINT Research Group Snyder JK SPRINT Research Group Sink KM SPRINT Research Group Rocco MV SPRINT Research Group Reboussin DM SPRINT Research Group Rahman M SPRINT Research Group Oparil S SPRINT Research Group Lewis CE SPRINT Research Group Kimmel PL SPRINT Research Group Johnson KC SPRINT Research Group Goff DC Jr SPRINT Research Group Fine LJ SPRINT Research Group Cutler JA SPRINT Research Group Cushman WC SPRINT Research Group Cheung AK SPRINT Research Group Ambrosius WT . A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373: 2103–2116.
Rakugi H, Ogihara T, Umemoto S, Matsuzaki M, Matsuoka H, Shimada K, Higaki J, Ito S, Kamiya A, Suzuki H, Ohashi Y, Shimamoto K, Saruta T, Combination Therapy of Hypertension to Prevent Cardiovascular Events Trial G. Combination therapy for hypertension in patients with CKD: a subanalysis of the Combination Therapy of Hypertension to Prevent Cardiovascular Events trial. Hypertens Res 2013; 36: 947–958.
Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B, Zanchetti A, group Vt. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004; 363: 2022–2031.
Zanchetti A, Bond MG, Hennig M, Neiss A, Mancia G, Dal Palu C, Hansson L, Magnani B, Rahn KH, Reid JL, Rodicio J, Safar M, Eckes L, Rizzini P, European Lacidipine Study on Atherosclerosis i. Calcium antagonist lacidipine slows down progression of asymptomatic carotid atherosclerosis: principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002; 106: 2422–2427.
Liu LZY, Liu G, Li W, Zhang X, Zanchetti A, FEVER Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005; 23: 2157–2172.
Rimoldi SF, Messerli FH, Chavez P, Stefanini GG, Scherrer U . Efficacy and safety of calcium channel blocker/diuretics combination therapy in hypertensive patients: a meta-analysis. J Clin Hypertens (Greenwich) 2015; 17: 193–199.
Acknowledgements
The COPE trial was supported by the Japanese Society of Hypertension. Trial registration: http://clinicaltrials.gov (identifier NCT00135551) and http://www.umin.ac.jp/ctr/index-j.htm (UMIN000001152). The COPE trial was conducted as a collaborative research effort between Yamaguchi University and the sponsor Kyowa Hakko Kirin (KHK). Publication of this sub-analysis was financially supported by KHK. KHK had no role in the design, data collection, performance, interpretation or writing of this sub-analysis.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
Dr SU was supported by research grants from Yamaguchi Prefecture, Japan, and KHK. Dr HR was supported by research grants from Daiichi Sankyo, Astellas Pharma, Dainippon Sumitomo Pharma, Eisai, Kowa Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, MSD, Nippon Boehringer Ingelheim, Novartis Pharma, Otsuka Pharmaceutical, Pfizer Japan, Sanofi, Shionogi and Takeda Pharmaceutical. Dr SU received honoraria from Boehringer Ingelheim, Mochida Pharmaceutical, Takeda Pharmaceutical, Kowa Pharmaceutical, Novartis Pharma, Bayer Yakuhin and Daiichi Sankyo. Dr HR received honoraria from KHK, Astellas Pharma, Daiichi Sankyo, Dainippon Sumitomo Pharma, Takeda Pharmaceutical, Eisai, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, MSD, Nippon Boehringer Ingelheim, Novartis Pharma, Pfizer Japan, Shionogi, Taisho Toyama Pharmaceutical, and Bayer Yakuhin. Dr SU serves on an ad-hoc advisory board for Nippon Boehringer Ingelheim. The remaining authors declare no conflict of interest.
Additional information
Combination therapy of hypertension to prevent cardiovascular events trial group Principal study coordinator: T Ogihara. Study adviser: T Saruta. Steering committee: RM Matsuzaki (Chairperson), T Eto, T Fujita, J Higaki, S Ito, A Kamiya, K Kikuchi, H Matsuoka, H Suzuki, C Tei. Protocol committee: RH Matsuoka (Chairperson), H Kumagai, Y Ohashi, H Rakugi, K Shimamoto, S Takishita, S Umemoto. Endpoint classification committee: RK Shimada (Chairperson), K Hayashi, K Kario, M Kawana, K Kitagawa, H Makino, M Matsumoto, J Yoshikawa. Independent data monitoring committee: RK Abe (Chairperson), H Matsuura, Y Ohashi, K Otsuka, K Tanabe. Safety committee: RN Suzuki (Chairperson), S Nogawa, K Utsunomiya, T Yoshikawa, W Yumura. Study statistician: RY Ohashi. Coordinating center: RS Umemoto (EBM Office, Center for Clinical Research, Yamaguchi University Hospital). Investigators: Hokkaido district: K Kikuchi, N Hasebe, M Bunya, W Fujii, N Funayama, M Gima, K Hashizume, Y Hirayama, H Matsuhashi, H Morimoto, T Myojo, K Ohori, H Omiya, T Ota, A Sato, T Shiokoshi, H Tanaka, K Yamazaki, H Yoshie, K Shimamoto, M Abiru, M Adachi, Y Fujise, K Hanawa, K Ishii, Y Kadono, T Kaku, S Kaneta, M Kato, N Kato, H Kobayashi, T Komakine, T Matsumoto, T Mita, N Miura, H Mukai, K Nagao, H Nakagawa, M Nakagawa, N Nakajima, T Nishimiya, Y Nishino, A Nunokawa, J Ohata, H Ooiwa, R Sato, S Satoh, S Shibata, M Takada, Y Takagawa, Y Takagi, S Takeichi, S Tanaka, N Togashi, N Ura, C Wakabayashi, D Yoshida, H Yoshida, K Yoshida, A Kitabatake, H Tsutsui, M Akutsu, S Fujii, T Furumoto, S Kakinoki, H Kawasaki, T Kimura, M Makiguchi, H Matsuo, H Okamoto, Y Oyama, J Shimokawa, N Tsuzuki; Tohoku district: S Ito, Y Imai, R Domon, H Ebina, S Egawa, T Haruyama, H Hashimoto, T Hayakawa, H Inomata, Y Katahira, T Katakura, R Kikuchi, H Kimura, S Kyogoku, Y Kyogoku, K Matsuo, H Nakazawa, H Odakura, F Okuguchi, E Ohtomo, H Ouchi, M Seino, M Tadokoro, Y Tanno, N Uchida, T Yamanaka, K Yunomura, K Okumura, T Hatayama, Y Kanehira, H Kaneko, M Kimura, N Maeda, A Mikuniya, H Narita, M Ono, T Osanai, M Sato; Tokyo district: H Yoshino, S Momomura, M Ono, M Inoue, T Iwase, K Miyazaki, M Taki, T Aizawa, Y Hasunuma, H Makino, H Okabayashi, S Hosoda, T Sumiyoshi, M Abe, Y Kira, M Nagayama, K Sakai, O Yoshikawa, M Ide, N Kimura, S Matsuzaka, Y Miyajima, K Sawai, T Sumi, R Takada, M Toma, Y Yamada, K Yoda, T Yokokawa, S Yokoyama, K Kanmatsuse, T Kushiro, T Anazawa, T Ebuchi, H Fujita, N Katsumata, K Masubuchi, T Migita, T Osada, Y Otsuka, F Saito, S Shimoda, K Sugino, A Takahashi, S Tani, K Yumi, H Daida, T Arino, T Iesaki, Y Inomata, H Nakahara, H Shiraishi, H Sudo, T Degawa, T Araki, H Itaya, H Komatsu, H Kuwana, T Mikawa, H Nomoto, N Ogawa, H Sato, H Takase, H Toyoda, M Yamamoto, K Obayashi, I Akabane, H Hamamoto, R Kanbara, H Kato, H Kimura, N Mori, K Yamada, M Yamamuro, M Isobe, H Emoto, O Inaba, T Inazawa, H Inomata, K Isobe, Y Ito, M Komura, H Kosuge, Y Maejima, N Miwa, T Nishimori, K Otomo, K Sakurai, M Sawada, M Seya, M Shimizu, T Takagi, M Tamura, K Tanaka, D Tezuka, T Tokunaga, A Yagishita, A Yamashina, T Hara, S Hayashi, Y Hirayama, Y Hirooka, M Iitaka, T Ishiyama, F Kijima, H Kobayashi, Y Kobayashi, K Kondo, T Kuwabara, M Mugishima, Y Nakayama, Y Nishizato, Y Osamura, Y Sakomura, S Saneshige, N Shindo, N Takao, Y Takata, H Tomiyama, S Ishimaru, Y Obitsu, H Shigematsu, T Baba, H Fukushima, T Hirayama, K Magari, S Makimura, T Nagae, K Osada, T Osada, T Shimizu, H Suesada, K Tamura, T Yamazaki, A Hirai, T Fukasawa, H Ono, M Yamakado, T Shiba, S Otomi, A Uehata, K Takazawa, A Aizawa, T Iketani, M Kino, H Kobayashi, T Morishima, N Sakamoto, T Sakamoto, H Yamakawa, H Kasanuki, R Nagai, T Kadowaki, J Tanaka, T Yamazaki, M Takagi, S Ui, S Baba, K Fujita, T Hasegawa, K Tajima, M Tanaka, N Yamato, I Kuwajima, K Harada, H Miyata, S Mizuno, S Ueda, K Sugi, H Ando, K Mishima, M Moroi, S Nishizawa, S Suzuki, J Yamazaki, R Nakanishi, H Nakano, K Tokuyasu, T Aoyagi, M Fujioka, N Kobayakawa, K Nakajima, A Hirayama, K Tsukamoto, Y Araki, H Hara, K Hara, T Saruya; Kanagawa district: S Umemura, M Arima, T Endo, K Furumi, Y Hatori, Y Ikeda, Y Ikeya, T Kaneda, T Kawada, T Kawano, T Kawashima, M Kihara, M Kikuta, A Kitamura, H Kobayashi, S Kobayashi, T Kuji, S Masuda, Y Minamimoto, K Minamisawa, T Mitsuhashi, N Miyazaki, Z Nagashima, T Nakatogawa, R Nakayama, N Nyui, M Ogawa, T Onishi, K Saka, T Sano, A Sato, K Shiba, F Shionoiri, H Sugiyama, H Suzuki, I Takasaki, K Tamura, Y Tokita, M Umemura, S Yamaguchi, G Yasuda; Chiba-Saitama district: S Nakamura, K Takayanagi, T Hayashi, M Ichihara, S Kobayashi, Y Sakai, T Uchida, I Yaguchi, I Komuro, S Aoki, Y Hashimoto, C Ibuki, Y Isobe, R Kumasaka, M Matsuda, K Mizuno, D Murakami, S Nakamura, M Nakatani, T Ohba, T Ohara, T Okumura, A Saito, T Sakurai, S Sato, W Sato, K Seimiya, Y Seino, K Shimizu, M Takano, K Tokuyama, D Uchida, K Yodogawa; Kitakanto-Koshinetsu district: S Oshima, M Kurabayashi, N Baba, Y Furushima, T Goto, T Hosoi, T Iijima, K Ito, Y Iwata, H Kubo, M Matsumoto, M Miyazaki, F Naganuma, K Nakada, M Tokushima, K Tsunoda, S Wakamatsu, Y Yagihara, Y Aizawa, M Aizawa, M Aizawa, N Hayashi, T Hori, H Kobayashi, M Kodama, K Maeda, K Miura, K Okada, Y Okura, Y Sasagawa, S Takizawa, M Tamura, T Yamamoto; Tokai district: T Murohara, Y Awaji, H Funahashi, D Hayashi, M Iida, D Ishihara, S Ishikawa, S Kamide, M Kanashiro, N Kurebayashi, S Kyo, H Matsui, K Matsuo, M Morishima, H Noda, T Noda, N Okumura, T Ota, S Shimizu, F Somura, Y Takada, Y Takeichi, H Takezawa, T Uchikawa, D Yoshikawa, G Kimura, Y Ando, M Hoshiai, N Okuda, S Suzuki, K Takada, N Takada, K Yamada, H Hishida, T Furuta, H Hayashi, K Ito, K Kato, M Nomura, T Ota, M Ohtsuki, T Tabata, S Taga, R Tateishi, T Ito, M Fukuda, T Iwa, Y Wakida, T Yonemoto, M Watarai, M Ito, H Kawai, Y Murata, S Nomoto, K Takemoto, N Tsuboi, Y Yoshida, N Inoue, M Ishikawa, M Matsumoto, T Muramatsu, R Yoshida, M Ono, Y Hanaki, H Sano, Y Shibata, K Sakai, M Ajioka, H Asano, R Okamoto, H Osanai, Y Uemura, K Yokoi, T Tanaka, H Kamiya, K Miki, M Niwa, H Fujiwara, S Minatoguchi, T Arai, S Kato, H Kobayashi, T Minagawa, N Mori, K Nakahara, Y Shimizu, M Tadokoro, N Takahashi, T Shigemasa, I Kobayashi, T Nakano, M Ito, A Fukui, Y Higashi, T Ito, U Kano, K Makino, K Nakai, M Nakajima, T Nakajima, K Sekoguchi, T Tanaka, T Tanigawa; Hokuriku district: N Takekoshi, H Enyama, T Hirakawa, J Ito, T Ito, H Kakuda, T Kigoshi, K Kondo, K Masuya, M Matoba, A Nakagawa, T Nakahashi, H Nakato, H Okada, M Okuro, Y Takeuchi, H Tsugawa, T Urata, M Yasuhara, M Shimizu, H Ino, T Araki, N Fujino, T Haraki, K Hayashi, S Hifumi, T Konno, M Minamoto, S Miyamoto, M Mori, C Nakanishi, Y Sakamoto, K Sakata, S Takeda, K Ueda, K Uchiyama, S Takata, S Kaneko, I Aburadani, I Inoki, K Kitano, D Kobayashi, K Kontani, M Maekawa, M Maruyama, K Matsunuma, Y Nagai, Y Nagata, M Okajima, K Otowa, Y Sekiguchi, K Shinmura, S Usui, H Yokoyama, M Yonejima; Kinki district: K Nakao, N Hiraiwa, T Ko, I Masuda, T Nagae, K Nishino, M Sakamoto, T Kita, Y Nakagawa, T Kimura, T Doi, H Horiuchi, M Kinoshita, M Mizuno, M Ohnishi, K Shigemoto, A Wada, T Yamada, H Yoshida, M Nakagawa, H Matsubara, K Furukawa, T Hatta, A Inoue, H Katsume, A Masui, S Matsumoto, T Seki, K Takeda, Y Taniguchi, H Tsuji, Y Saito, Y Fukuoka, M Iwano, T Katsuyama, A Nakatani, Y Sakaguchi, T Konishi, T Izumi, I Toda, A Kamimoto, Y Nagai, E Matsuwaka, R Matsuwaka, K Takei, R Ueda, N Wakaki, T Iwasaka, H Hamada, S Hamada, H Koga, H Koito, K Kono, H Kurihara, J Maeda, S Morimoto, Y Takayama, T Aoyama, M Imai, T Ii, S Kashii, M Maenaka, H Ohashi, T Suyama, M Matsuda, Y Aoyagi, K Kunisada, T Mori, T Mori, J Uemura, Y Yokoi, N Morioka, T Ozaki, K Kanamasa, K Ishikawa, S Miyazaki, S Arima, T Kai, A Kurooka, I Shimada, M Takewa, M Taniguchi, R Hattori, K Haba, R Yokota, H Matsui, E Tone, H Yamahira, T Kawarabayashi, H Inaba, Y Sakaguchi, Y Yamamoto, H Ito, M Date, M Dodo, K Fujii, M Imai, K Inoue, Y Kanoh, N Komura, S Senpuku, M Takeda, H Tateyama, K Yasui, R Yoneda, H Morita, M Kawanami, A Tahara, T Sado, T Takamura, M Taniwa, Y Kitaura, M Fukuda, H Hanada, K Nakamura, K Sawada, M Yamaguchi, K Kodama, T Higo, A Hirata, M Kanzaki, S Komatsu, K Matsuo, T Murakawa, H Nakanishi, T Nemoto, M Nishio, N Ogasawara, Y Okuyama, Y Ueda, M Imanishi, Y Kitamura, T Sakakibara, H Yoshida, H Yoshimi, T Ogihara, H Rakugi, M Akiyama, Y Ikuno, N Imai, Y Imamura, T Inoyama, K Kamide, K Katahira, S Katsuya, T Katsuya, Y Kurokawa, O Matsuki, M Matsuo, T Nakamura, E Ogura, M Ohishi, R Sasaki, K Sugimoto, J Tachi, H Tanaka, H Tanaka, T Tsunetoshi, M Yoshino, M Hori, N Awata, T Fukukawa, Y Iimori, S Iwamoto, K Sawami, M Okamura, Y Kanayama, F Nagano, H Nakayama, H Suzuki, T Amano, K Tachibana, Y Arita, M Kirino, K Sakuyama, M Shukawa, Y Nishida, T Sakamoto, S Yanagi, K Hirota, T Majima, T Ota, T Tanaka, R Nohara, T Funauchi, O Isogai, S Takashima, H Koike, M Nishimoto, Y Kawase, O Tojo, Y Chimori, H Harada, H Takeoka, S Kishi, M Yokoyama, K Hirata, J Ejiri, R Emoto, Y Furuta, K Hattori, R Kuroda, N Maehashi, H Monnaka, Y Ohashi, T Okada, H Suzuki, M Takeuchi, M Ohyanagi, M Masai, T Masuyama, M Kawabata, T Kajiya, N Daito, T Fujisawa, S Fujita, M Hasegawa, M Hirakoba, T Hirano, Y Ikeda, N Imai, K Marumoto, S Masuda, T Miki, M Mitsunaga, H Mitsuoka, Y Miyachi, N Mukohara, T Nagao, K Nakada, K Nishian, S Nishioka, T Ogura, Y Onishi, K Sakaguchi, I Sano, W Sano, M Shigenobu, A Tabuchi, J Takashima, Y Taniguchi, H Uchida, T Ueda, N Urabe; Chugoku district: H Makino, S Harada, S Hirakawa, H Hirata, J Ishii, K Koten, Y Nagake, T Nakajima, Y Nakamura, T Terami, K Mitsudo, M Fujii, K Fujita, E Iwano, K Kadota, Y Nishihara, Y Takaya, H Yamamoto, T Yamamoto, C Shigemasa, I Hisatome, T Kato, H Miyakoda, M Sakamoto, M Shimoyama, T Shimada, K Tanabe, Y Goto, Y Hanada, K Kawakami, J Kitamura, K Kitamura, H Nakata, N Oyake, H Sugiura, H Tsukihashi, M Matsuzaki, S Umemoto, S Aoyagi, H Aoyama, T Fujino, S Fukuta, N Hiroyama, Y Ikeda, Y Inamoto, R Kametani, A Kamiya, Y Kanamaru, S Kotoku, A Matsushima, J Morita, Y Murano, M Nakatsuka, S Nishimura, Y Nisnimura, T Okamura, F Okuda, U Onaka, M Ozaki, A Shimizu, C Takata, M Tamitani, T Watada, T Watada, K Yamamoto, M Yamauchi, T Yorozu, H Yoshikane, F Yoshino; Shikoku district: J Higaki, J Doiuchi, T Fukuoka, H Hashimoto, M Igase, H Kadota, H Kaneko, S Komatsu, Y Matsubara, K Miyoshi, K Murakami, S Murao, T Niiya, T Ochi, A Satoh, T Seki, H Takahashi, T Yamashita, T Yoshino, M Kohno, N Fujita, T Fukui, T Hamamoto, K Hasegawa, H Hitomi, K Ihara, H Kiyomoto, H Masugata, I Matsumoto, N Takahashi, K Yoshikawa, Y Doi, M Arisawa, T Egawa, M Fukuda, Y Kawada, H Kusunose, T Maeda, N Minami, M Nishinaga, T Noguchi, K Okabayashi, K Sato, T Satomi, J Takada, S Tamura, T Usui, M Yamada, M Irahara, H Azuma, M Fujimura, H Fujino, M Fujino, E Harada, S Harada, Y Hiasa, S Hosokawa, K Kawahara, K Koshiba, M Murakami, Y Nakaya, H Nii, S Nozaki, A Ota, T Ozaki, K Sone, Y Tsutsui, S Ueta; Kyushu district: M Nobuyoshi, Y Fujishima, K Hisano, H Ikezono, R Imawatari, Y Izumi, H Kanai, T Nakamura, T Nakamura, T Noda, E Ono, S Tanaka, T Tsuiki, T Yanai, T Sasaguri, S Akimitsu, K Dohmen, K Fujisawa, K Fukuyo, S Harashima, T Hayashi, M Hirata, Y Hirata, N Ikeda, H Ikematsu, W Ikematsu, W Kajiyama, Y Kawakami, I Kawasaki, H Kondo, H Kusuhara, N Maeda, H Miyahara, A Motomura, K Nakamura, T Noguchi, T Okinaga, M Sato, I Shimada, H Shin, K Soejima, K Sugi, T Taniguchi, T Uwatoku, S Yamaga, K Yamaji, J Yanagi, H Yano, K Saku, M Enomoto, T Hiratsuka, K Imoto, R Kamei, H Kanaya, M Kohara, M Kusuda, H Nishikawa, H Sako, T Imaizumi, K Yano, K Maemura, N Ashizawa, M Hazama, Y Ishida, T Ito, M Kanda, M Kimura, T Noguchi, Y Oku, S Seto, S Suzuki, H Ogawa, K Goto, K Honjio, Y Horio, H Jinnouchi, Y Kaku, S Kawano, T Kimura, Y Kiyohara, A Maki, N Matsumoto, K Misumi, T Sakamoto, K Sasaki, S Sugiyama, E Tanaka, S Uemura, C Tei, K Arima, Y Daitoku, H Eto, T Hashino, K Ichinari, Y Ikeda, A Iriki, K Kiyonaga, K Kubota, Y Makise, S Masuzaki, M Miyata, H Mizoguchi, T Niiyama, Y Samejima, S Yonezawa.
Supplementary Information accompanies the paper on Hypertension Research website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Umemoto, S., Ogihara, T., Matsuzaki, M. et al. Effects of calcium channel blocker benidipine-based combination therapy on target blood pressure control and cardiovascular outcome: a sub-analysis of the COPE trial. Hypertens Res 40, 376–384 (2017). https://doi.org/10.1038/hr.2016.158
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2016.158
Keywords
This article is cited by
-
Anti-inflammatory activity of benidipine hydrochloride in LPS-activated mammalian macrophages
Naunyn-Schmiedeberg's Archives of Pharmacology (2024)
-
Analysis of antihypertensive treatment using real-world Japanese data—the retrospective study of antihypertensives for lowering blood pressure (REAL) study
Hypertension Research (2019)
