
Abstract
Objective
To report a newly recognized adverse effect of oral moxifloxacin.
Design
Observational case reports.
Participants
Five patients who used oral moxifloxacin therapy.
Main outcome measures
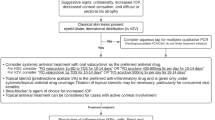
In five patients, a uveitis-like episode followed oral moxifloxacin therapy, afterwards they experienced photophobia. At slitlamp investigation, the patients showed almost complete iris transillumination, not restricted to one sector, and persistent mydriasis of the pupil, with no reaction to light and no near reflex. Follow-up of 3 years in one of the patients showed no change of symptoms. Only in one patient, with a history of anterior uveitis, an anterior chamber tap was positive for herpes simplex genome. Only after the use of moxifloxacin did she experience continuous photophobia.
Conclusions
Iris transillumination and sphincter paralysis is a newly recognized adverse effect of oral moxifloxacin therapy.
Similar content being viewed by others

Introduction
Moxifloxacin, 8-methoxyquinolone, is a synthetic broad-spectrum antibacterial agent. Pharmacokinetic studies have shown high tissue affinity. Whole-body scinti-radiography in rats after administration of radioactive-labeled moxifloxacin showed high concentrations in most organs, tissues, and melanin-containing structures in the eye, meninges, and hair follicles of the pigmented skin.1
Moxifloxacin is indicated for the treatment of acute exacerbations of chronic bronchitis, community-acquired pneumonia, and acute bacterial sinusitis. Recent studies have investigated intra-ocular concentrations of topically administered moxifloxacin ophthalmic solutions for prophylaxis against and treatment of intra-ocular infections.2
Numbers of prescriptions are rapidly rising in the Netherlands and in Belgium. We report five patients, who showed Iris transillumination and persistent mydriasis 3–4 weeks after oral moxifloxacin therapy.
To our knowledge, the extensive iris transillumination (with variable sphincter paralysis) as an adverse effect of oral use of moxifloxacin has not yet been previously reported.
Case reports
Five patients experienced a uveitis-like episode after the use of oral moxifloxacin with painful eyes; in the two patients seen in the acute stage, there was no severe anterior chamber reaction, only a few pigmented cells were observed. After 10–14 days, they developed a severe persistent photophobia, which interfered with their normal outdoor activities.
The first three patients were all referred to The Rotterdam Eye Hospital after the acute stage for evaluation of their uveitis and severe photophobia.
History revealed a uveitis-like episode 10–14 days after the use of oral moxifloxacin. Only the second patient (32-year-old female) had two earlier episodes of anterior uveitis in each eye in 2004. Examination of the iris in 2004 did not reveal any iris transillumination. In all three patients, a severe iris transillumination was visible (Figure 1).

Patient 1.
Gonioscopy showed normal findings with mild pigmentation of the trabecular meshwork. Aqueous taps were performed, and were positive for herpes simplex genome only in the patient who had a former history of uveitis.
The fourth patient was referred to the university hospital of Gent, for evaluation of her photophobia and painful eyes. History revealed oral use of moxifloxacin, and aqueous tap showed no herpes simplex genome or serological evidence of herpes infection.
The fifth patient (74-year-old male) was referred to the university Hospital of Brussels for evaluation of a first episode of bilateral acute anterior uveitis. He presented with hyperaemic, painful eyes. Symptoms occurred 12 days after intake of oral moxifloxacin.
All patients used recommended doses (5–10 days 1 tablet).
Initial slitlamp examination showed bilateral aqueous cells, endothelial dusting, posterior synechia, segmental transillumination, and miotic, light-responsive pupils. Gonioscopy showed normal pigmentation of the trabecular meshwork. After treatment with topical prednisone, uveitis signs resolved and evolved into permanent diffuse iris transillumination and mydriasis (Figure 2).

Patient 4.
In all patients, visual acuity remained unaltered. Elaborate work-up revealed no other cause of uveitis (see Table 1 for details of all patients). There were no signs of pseudoexfoliation syndrome. The iris transillumination and mydriasis showed the same pattern, without pigment dispersion on the surface of the iris or pigment accumulation in the chamber angle.
Discussion
We report five patients who showed severe photophobia due to almost complete iris transillumination and persisting mydriasis after a uveitis-like period after the use of moxifloxacin in otherwise healthy patients.
One case of bilateral uveitis and pigment dispersion after the use of moxifloxacin has been reported in literature.3 In this case, pigment was dispersed over all the structures in the anterior chamber. In our patients, the pigment could no longer be detected.
Although herpetic infection is not completely ruled out by the negative aqueous taps by PCR (66% sensitivity),4 the clinical pattern differs with herpetic uveitis, which generally shows a sectorial pattern of iris transillumination and unilaterality.
Herpetic genome was positive in the aqueous tap only in the patient with a previous history of anterior uveitis, but she only developed photophobia 3 weeks after the use of oral moxifloxacin.
In all patients, all other causes of uveitis were excluded.
The high tissue affinity of moxifloxacin, especially in melanin-containing structures of the eye,1 might induce phototoxicity in the iris pigment in susceptible patients when compared with photosensitive dermatitis caused by quinolones.5
Two of our patients used moxifloxacin during holidays abroad, where more light exposure is expected than in their home country. The other three had no extra light exposure.
We cannot exclude phototoxicity, but it is not likely the only cause. Extended use of sunglasses is, therefore, not yet recommended by us during and after the use of oral moxifloxacin.
Retinal pigment epithelium could be affected,6 but none of our patients showed any visible changes in the retinal pigment epithelium.
We are aware of the fact that there may be a multifactorial aetiology of this adverse effect, but we are convinced that the use of oral moxifloxacin is one of these factors.
We expect a rise in the number of reports of this particular adverse effect after recognition of this condition.

Conflict of interest
The authors declare no conflict of interest.
References
Siefert HM, Kohlsdorfer C, Steinke W, Witt A . Pharmacokinetics of the 8-methoxyquinolone, moxifloxacin: tissue distribution in male rats. J Antimicrob Chemother 1999; 43 (suppl B): 61–67.
Hariprasad SM, Blinder KJ, Shah GK, Apte RS, Rosenblatt B, Holekamp NM et al. Penetration pharmacokinetics of topically administered 0.5% moxifloxacin ophthalmic solution in human aqueous and vitreous. Arch Ophthalmol 2005; 123: 39–44.
Bringas Calvo R, Iglesias Cortinas D . Acute and bilateral uveitis secondary to moxifloxacin. Arch Soc Esp Oftalmol 2004; 79: 357–359.
de Groot-Mijnes JD, Rothova A, van Loon AM, Schuller M, Ten Dam-Van Loon NH, De Boer JH et al. Polymerase chain reaction and Goldmann–Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am J Ophthalmol 2006; 141: 313–318.
Hamanaka H, Mizutani H, Asahig K, Shimizu M . Melanocyte melanin augments sparfloxacin-induced phototoxicity. J Dermatol Sci 1999; 21: 27–33.
Dayhaw-Barker P . Retinal pigment epithelium melanin and ocular toxicity. Int J Tox 2002; 21 (6): 451–454.
Author information
Authors and Affiliations
Corresponding author
Additional information
The first patient is shown as a case report poster at the Conference of the Dutch Ophthalmological Society in 2004
Rights and permissions
About this article
Cite this article
Wefers Bettink-Remeijer, M., Brouwers, K., van Langenhove, L. et al. Uveitis-like syndrome and iris transillumination after the use of oral moxifloxacin. Eye 23, 2260–2262 (2009). https://doi.org/10.1038/eye.2009.234
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.234
Keywords
This article is cited by
-
Severe sequelae in bilateral acute iris transillumination syndrome secondary to the use of oral moxifloxacin: a case report
Journal of Medical Case Reports (2021)
-
Bilateral acute iris transillumination following systemic administration of antibiotics
Eye (2018)
-
Drug-induced uveitis
Journal of Ophthalmic Inflammation and Infection (2013)
-
Uveitis-like syndrome and iris transillumination after the use of oral moxifloxacin
Eye (2010)
-
Responding letter
Eye (2010)
