
Abstract
The identification of glaucomatous damage and monitoring of disease progression require the measurement of both structural and functional changes. Ongoing research is focused on the relationship between these two types of changes. The purpose of this paper is to examine four aspects of the association between structural and functional changes of the optic nerve head (ONH)—the spatial relationship between changes in the ONH and visual field, the quantitative relationship between these changes, the difficulties of using summary statistics to quantify damage, and a comparison of how structure and function measurements allow us to detect progression and how these measurements agree with each other. Dissociation between structural and functional measurements may occur—it is possible that some structural change does not relate to ganglion cell loss, and some functional loss does not relate to cell loss but to dysfunction. Current data suggest that both structural and functional measurements are necessary to monitor disease progression, which is important for making clinical decisions.
Similar content being viewed by others
Introduction
The identification of glaucomatous damage and monitoring of disease progression require the measurement of both structural and functional changes. Ongoing research is focused on the relationship between these two types of changes. The purpose of this paper is to examine four aspects of the correlation between structural and functional changes of the optic nerve head (ONH)—the spatial relationship between changes in the ONH and visual field (VF), the quantitative relationship between these changes, the difficulties of using summary statistics to quantify damage, and a comparison of how structure and function measurements allow us to detect progression and how these measurements agree with each other.
Spatial relationship between changes in the nerve and the visual field
In 2000, we examined the relationship between the VF test points in the Humphrey 24-2 test pattern and sectors of the ONH.1 The VF grid was appropriately scaled and overlaid onto retinal nerve fibre layer photographs. We centred the VF on the fovea, with a circle marking the ONH, and then followed the margins of defects or prominent nerve fibre bundles to see where individual VF test points would be related at the ONH. A clinically useful map was produced, which relates VF field test points to regions of the ONH (Figure 1). This map, however, provides only an anatomical description, and does not relate function to structure.

A division of the visual field (a) and optic nerve head (b) into mapped sectors according to the results of a study of defects in 69 normal-tension glaucoma or glaucoma suspect patients. (Reproduced from Garway-Heath et al1 with permission of Ophthalmology, Copyright 2000, with permission from Elsevier.)
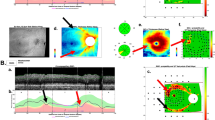
Gardiner et al2 produced a different type of map, a topographical map of the relationship between sectors of the ONH and locations in the VF (Figure 2). Specifically, they looked at the correlation between Heidelberg retina tomograph (HRT) neuroretinal rim area (NRA) and VF sensitivity at each point in the VF. For most points in the VF, there was a fairly good correspondence between the actual structure/function correlations in glaucoma patients and those from the anatomical map (Figure 1). However, there were exceptions where correspondence was less good, particularly in the more peripheral VF and in the temporal VF. It is difficult to be certain why those exceptions occurred, but the possibilities include a limited range of sensitivity values, which would make correlations less strong, the fact that the HRT-NRA values include blood vessels (which confounds the true NRA measurement more in some parts of the ONH than others), the greater inter-individual variability of NRA in some sectors and of some VF test points, and the fact that VF test points (and NRA sectors) are not independent of each other. Nevertheless, at least some functional/structural correlation is possible.

Topographical map of the relationship between sectors of the ONH and locations in the visual field, using empirical cross-sectional patient data; the shade of grey in the sectors indicates the strength of correlation. The red bar indicates the location of expected strongest correlation on the basis of the map given in Figure 1. (Reproduced from Gardiner et al2 with permission of Invest Ophthalmol Vis Sci via Copyright Clearance Center.) ONH, optic nerve head.
Quantitative relationship
In a 1985 paper by Airaksinen et al,3 magnification-corrected measurements of the NRA were found to be highly significantly associated with VF sensitivity in a nonlinear manner. A similar nonlinear association was found in a study by Bartz-Schmidt et al,4 in which the NRA was measured with the HRT.
A study was conducted in 1999 to investigate the relationship between electrophysiological, psychophysical, and anatomical measurements in glaucoma.5 The parameters measured were VF sensitivity, the pattern electroretinogram amplitude (believed to reflect function in the inner retina6), and the NRA in the temporal half of the ONH using the HRT. The association between variables was investigated by linear and quadratic regression analysis. The quadratic (nonlinear) regression fits were stronger than the linear. The findings of a nonlinear fit suggest that, at all stages of disease, loss of ganglion cells is associated with a loss of function, albeit with a changing structure/function slope at different stages of disease (a shallow structure/function slope in early disease and a steep structure/function slope in later disease). This supports the hypothesis that there is no RGC reserve that has to be lost before functional deficits manifest but, instead, there is a continuous structure/function relationship and any loss in RGCs will manifest in reduced VF sensitivity. The pattern of the structure/function association suggested by this research is that, in early disease, VF changes, scaled in dB loss, occur relatively slowly compared with structural changes. Later in the disease, functional changes are more marked than structural changes. It may be that, if the VF were tested and quantified on a linear (rather than dB) scale,7 functional and structural measures may have a more linear association and change similarly, regardless of stage of disease.
Summary statistics
There is some difficulty in using summary statistics to relate structure and function arising from differences in the way in which RGCs are quantified. If the ONH is divided into equal sectors, and the sectors are related to the VF map (Figure 1), there is considerable variation in the number of VF test points examined in each ONH sector. In some 30° sectors, there may be nine test points (such as an infero-temporal ONH sector), whereas in others there may only be two, or none. Therefore, an average of VF test point sensitivity will be weighted towards certain parts of the ONH. Another problem is the relationship between density of VF test points and RGC density. The VF has a regular grid of test points, whereas RGC density is much greater near the fovea than peripherally. If mean deviation is used as a summary statistic, there is disproportionate weighting in favour of the peripheral field compared with the central field. The implication is that estimates of disease severity and progression rate may differ between investigations (structural and functional), because of differences in sampling of the VF and in scaling.
Detection of progression
There is conflicting evidence as to how imaging compares with VF testing in detecting progression. In the Ocular Hypertension Treatment Study,8 a large proportion of patients whose disease progressed were picked up by imaging, whereas virtually none was identified in the Early Manifest Glaucoma Trial.9 However, it is difficult to compare the two studies, because of differences in methodology and criteria applied, and a lack of external validation of change criteria.
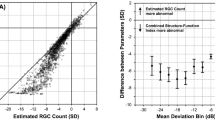
A study that specifically compared estimates of progression from series of HRT images and VF tests found that a much greater number of patients with established glaucomatous VF loss were identified as progressing from the HRT images series.10 Again, the results are criterion-dependent and without an estimate of specificity for the chosen criteria. It is difficult to determine, therefore, whether the HRT and VF change criteria were located at a different part of a similar receiver operating characteristic (ROC) curve (with differing levels of specificity) or were located at similar parts of a differently shaped ROC curve (with similar levels of specificity) (Figure 3).

Poor correlation between imaging and visual fields: progression was detected by both techniques in few eyes.
This issue was partly addressed in a later study of the same group of glaucoma patients and normal controls, who were followed up prospectively for 7 years for evidence of the relationship between VF and ONH changes using standard automated perimetry (SAP) and HRT.10 Three different sets of criteria were compared—most conservative, intermediate, and least conservative. The analysis was balanced so that roughly the same number of subjects would be progressing by structure and function criteria at each stringency level. Although SAP and HRT detected roughly equal numbers, the overlap was poor; different eyes progressed by one modality or the other, and few by both (Figure 4).

Venn diagram of the classifications with least conservative, intermediate and most conservative criteria, based on EOC criteria. (Reproduced from Artes and Chauhan.11 with permission of Prog Retinal Res from Elsevier.)
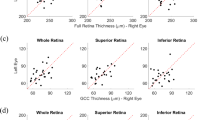
A similar study12 considered HRT and VF data over time for 192 ocular hypertensive patients, some of whom had developed VF loss during the observation period, and for 21 normal subjects. Linear regression analysis was used to define HRT-NRA and VF progression, and change criteria were adjusted to obtain particular levels of specificity (as judged by the proportion of subjects showing significant positive change and by the proportion of normal subjects showing significant negative change). When the specificity level was set at about 90%, roughly equal numbers progressed according to HRT and VF, with a relatively small overlap between the two. Two-thirds of the patients in the overlap changed in corresponding regions of the ONH and VF. With more stringent criteria and a specificity set at 97%, fewer cases were detected — about 9% with HRT and 15% by VF—but the very small overlap had 100% congruity between structure and function change (Figure 5).

Specificity and congruity for HRT and visual field examination in 192 ocular hypertensive patients. (Reproduced with Strouthidis et al12 with permission of Invest Ophthalmol Vis Sci via Copyright Clearance Center.) HRT, Heidelberg retinal tomograph. The numbers in the bottom left corners are: ‘Percentage of stable patients’. The numbers in the Venn diagrams are: ‘Percentage of patients identified as progressing by perimetry and imaging’.
The most likely cause for the lack of concordance between structural and functional estimates of progression in glaucoma is that ‘noise’ in the measurement system is greater for one modality than the other in some patients. It is also possible that some structural changes that occur are not directly related to RGC loss (such as lamina cribrosa bowing), or that functional loss is unrelated to RGC loss but related to RGC dysfunction, non-RGC retinal disease, cataract development or posterior visual pathway disease. Indeed, it has been suggested that reversible RGC dysfunction may be a significant component of the loss of function seen in glaucoma.13
Conclusion
It can be concluded from the evidence presented that the previously held belief, that structural tests are better than functional tests to identify abnormality or progression in OHT and early glaucoma, is not justified. Dissociation between structural and functional measurements may occur—it is possible that some structural change does not directly relate to RGC loss, and some functional loss does not directly relate to structural loss but to dysfunction. Current data suggest that both structural and functional measurements are necessary to monitor disease progression.
References
Garway-Heath DF, Poinoosawmy D, Fitzke FW, Hitchings RA . Mapping the visual field to the optic disc in normal tension glaucoma eyes. Ophthalmology 2000; 107: 1809–1815.
Gardiner SK, Johnson CA, Cioffi GA . Evaluation of the structure–function relationship in glaucoma. Invest Ophthalmol Vis Sci 2005; 46: 3712–3717.
Airaksinen PJ, Drance SM, Douglas GR, Schulzer M . Neuroretinal rim areas and visual field indices in glaucoma. Am J Ophthalmol 1985; 99: 107–110.
Bartz-Schmidt KU, Thumann G, Jonescu-Cuypers CP, Krieglstein GK . Quantitative morphologic and functional evaluation of the optic nerve head in chronic open-angle glaucoma. Surv Ophthalmol 1999; 44 (Suppl 1): S41–S53.
Garway-Heath DF, Holder GE, Fitzke FW, Hitchings RA . Relationship between electrophysiological, psychophysical, and anatomical measurements in glaucoma. Invest Ophthalmol Vis Sci 2002; 43: 2213–2220.
Arden GB, Vaegan, Hogg CR . Clinical and experimental evidence that the pattern electroretinogram (PERG) is generated in more proximal retinal layers than the focal electroretinogram. Ann NY Acad Sci 1982; 388: 580–607.
Malik R, Swanson WH, Garway-Heath DF . Development and evaluation of a linear staircase strategy for the measurement of perimetric sensitivity. Vision Res 2006; 46: 2956–2967.
Kass MA, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open angle glaucoma. Arch Ophthalmol 2002; 120: 701–713.
Heijl A, Leske MC, Bengtsson B, Bengtsson B, Hussein M, Early Manifest Glaucoma Trial Group. Measuring visual field progression in the Early Manifest Glaucoma Trial. Acta Ophthalmol Scand 2003; 81: 286–293.
Chauhan BC, McCormick TA, Nicolela MT, LeBlanc RP . Optic disc and visual field changes in a prospective longitudinal study of patients with glaucoma: comparison of scanning laser tomography with conventional perimetry and optic disc photography. Arch Ophthalmol 2001; 119: 1492–1499.
Artes PH, Chauhan BC . Longitudinal changes in the visual field and optic disc in glaucoma. Prog Retinal Res 2005; 24: 333–354.
Strouthidis NG, Scott A, Peter NM, Garway-Heath DF . Optic disc and visual field progression in ocular hypertensive subjects: detection rates, specificity, and agreement. Invest Ophthalmol Vis Sci 2006; 47: 2904–2910.
Ventura LM, Porciatti V . Restoration of retinal ganglion cell function in early glaucoma after intraocular pressure reduction: a pilot study. Ophthalmology 2005; 112: 20–27.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Garway-Heath, D. Correlation of visual changes with disc morphology. Eye 21 (Suppl 1), S29–S33 (2007). https://doi.org/10.1038/sj.eye.6702885
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702885
