
Abstract
Conventional renal cell carcinoma (CRCC) may appear in families with germline translocations involving chromosome 3, although a recurrent responsible gene has not been found. We recently described a family with CRCC and a constitutional t(3;8)(p14.1;q24.23), and we demonstrated that no genes were disrupted by the translocation breakpoints. In order to investigate the genetic origin and features of the CRCC tumors that occurred in this family, we have extended the pedigree up to four generations, and analyzed peripheral blood samples from 36 members, CRCC tumors, normal renal tissues, and a gastric tumor. (1) By means of comparative genomic hybridization (CGH), we have detected loss of the derivative chromosome carrying 3p in all CRCC but not in the corresponding normal renal tissue. In addition, by means of the fluorescence in situ hybridization technique, we have observed that not all tumoral cells lose the der(3p), which suggests that, previous to this loss, another hit should occur to initiate the transformation of normal into tumoral cells. (2) All known mechanisms of inactivation of the candidate von Hippel-Lindau (VHL) gene have been studied in the tumors, detecting alterations in 65% of them. This confirms that inactivation of the VHL gene is not always required to develop CRCC, and that (an)other suppressor gene(s) on 3p could be involved. (3) We discard FHIT as an alternative pathway to VHL. We have not found new candidate regions along 3p by using a 1-Mb resolution array-based CGH. (4) The tumorigenesis mechanism of a second gastric tumor developed in the probandus is different from that of CRCC.
Similar content being viewed by others

Introduction
Hereditary conventional renal cell carcinoma (CRCC) is a rare entity mostly associated with the von Hippel-Lindau (VHL) syndrome caused by germline mutations in the VHL gene located in 3p25.1, 2, 3 However, some hereditary CRCC cases associated with constitutional chromosome translocations involving chromosome 3 have also been reported.4 At the present time, seven families and two de novo cases carrying constitutional translocations involving chromosome 3 associated with high risk of developing CRCC have been reported.5, 6, 7, 8, 9, 10, 11, 12, 13, 14
Although all CRCC-associated translocations involve chromosome 3, the partners are not recurrent. The positions of the breakpoints in chromosome 3 vary among all cases, but they all map in the proximal p- and q-arm regions. In some of them, different genes have been cloned at the breakpoints: FHIT and TRC8 on chromosomes 3 and 8, respectively, in t(3;8)(p14;q24);15, 16 DIRC3 and DIRC2 in t(2;3)(q35;q21) translocation;17, 18 DIRC1 on chromosome 2 in t(2;3)(q33;q21);9 and finally, LSAMP and NORE1 in t(1;3)(q32;q13.3).19 As regards t(3;8)(p14.1;p14.23), previously identified by our group,14 no genes have been found in the breakpoints.20
A very common event identified by comparative genomic hybridization (CGH) or LOH in most of the tumor samples of these families is the loss of the derivative chromosome carrying the 3p segment. In addition to this, somatic VHL mutations have been identified in about 50% of tumor samples.4, 8, 10, 11, 14, 21, 22, 23
According to these data and in contrast with the classical two-hit model of Knudson for tumor suppressor genes,24 an alternative three-step tumorigenesis model for familial renal cell carcinoma with chromosome 3 translocation has been proposed.22, 25 The first step would consist of the inheritance of the constitutional chromosome 3 translocation that would be the primary oncogenic event. The second hit would be the loss in the tumor, of the derivative chromosome carrying the 3p segment der(3p), as a consequence of an erroneous chromatid separation, due to the presence of the translocation.26 And finally, the third hit would occur in cells lacking the derivative chromosome and would consist of a somatic mutation in a tumor suppressor gene located on 3p, relevant to renal tumorigenesis, such as the VHL gene.
According to these points, hereditary CRCC associated with constitutional chromosome 3 translocations constitutes a paradigm from a genetic point of view with some unsolved questions: (1) Is the loss of der(3p) the first tumorigenic event? (2) Does the same tumorigenesis mechanism occur in other nonrenal tumors developed by translocation carriers? (3) Is a mutation in the VHL gene always necessary to develop the tumor?
In the present work, we have extended the analysis of a t(3;8)(p14.1;q24.23) family previously studied by us14 to 36 members through four generations. We have performed an extensive genetic and cytogenetic analysis of the family: renal tumors and corresponding normal renal tissues, and a second gastric tumor developed by the probandus. Our results showed that: (1) previous to the loss of the derivative chromosome carrying 3p, another hit should occur to transform normal renal cells, (2) a gastric tumor developed by a translocation carrier does not follow the same multistep tumorigenesis mechanism as dorenal tumors, and (3) the VHL gene is not always necessary for the development of a tumor.
Materials and methods
Patients and samples
Previously, we described a family with three CRCC and t(3;8)(p14;q23).14 Since then, the study has been extended to other familial branches. The number of members identified as affected with CRCC and/or translocation carriers is represented in Figure 1. At present, nine members of the family belonging to four generations have developed CRCC and eight of them developed bilateral forms. The ages of onset vary from 25 to 82 years. Other neoplasias have occurred in this family: two gastric tumors (II-2 and IV-3), a central nervous system tumor (II-3), a papillary renal cell carcinoma (III-2), two lymphomas (III-5 and III-22), and two breast tumors (III-3 and III-21).

t(3;8)(p14.1;q24.23) family pedigree. The framed part of the pedigree was previously reported by Melendez et al (2003).
Peripheral blood samples from 36 members of the family were available for cytogenetic analysis. In addition, 10 CRCC samples from four family members (IV-3, IV-22, IV-31, and V-5) (five paraffin embedded, four frozen, one fresh), and one fresh normal kidney tissue (IV-22 (N)), were studied. We also obtained frozen material from the gastric tumor of the proband (IV-3). Five sporadic CRCC samples were used as controls for immunohistochemistry studies.
Informed consent was obtained from all the individuals studied.
Cytogenetic analyses
Cytogenetic analyses were carried out on metaphase spreads derived from cultured peripheral blood lymphocytes using standard cytogenetic procedures. A normal fresh renal tissue sample from patient IV-22 of the t(3;8)(p14.1;q24.23) family was disaggregated with collagenase and subsequently cultured in RPMI 1640 medium supplemented with 10% fetal serum and antibiotics. Metaphase spreads were prepared according to standard procedures. Karyotypes were described according to ISCN.27
DNA isolation from blood cells and from paraffin-embedded and frozen tissues
High-molecular-weight DNAs were directly extracted from peripheral blood cells using standard procedures of proteinase K/SDS treatment followed by phenol/chloroform extraction and ethanol precipitation.
With regard to tumors, prior to DNA extraction, tumor and normal tissue areas were selected via microscopic inspection. DNA was extracted from paraffin and frozen tissues using a proteinase K, phenol–chloroform, Phase Lock Gel™ Light (Eppendorf AG, Germany) and EtOH protocol.
Comparative CGH and LOH analysis
For the analysis of the loss of der(3p), CGH was performed in paraffin-embedded and frozen samples, according to Kallioniemi et al28 with slight modifications.
The 3p LOH analysis of the gastric tumor sample of patient IV-3 was performed with the microsatellites and conditions used by Melendez et al.14
Fluorescence in situ hybridization (FISH) on paraffin sections and on touch imprint cytologies
In order to detect the status of the derivative chromosome with the 3p segment in the tumor and normal renal tissue of the translocation carriers, FISH analyses were carried out on paraffin sections from IV-31 and on touch imprint cytology from IV-22. In each sample, an average of 110 (50–200) well-defined nuclei were analyzed. The tumor samples (both paraffin and touch cytology) contained more than 90% of tumor cells.
Two sets of probes were used to detect the loss of derivative chromosome 8 carrying the 3p segment: green commercial centromeric probe of chromosome 8 (CEP 8 (D8Z2) SpectrumGreen, Vysis) with red commercial probe of chromosome 17 as internal control (CEP 17 (D1721) SpectrumOrange, Vysis), and a green CEP 8 and a bacterial artificial chromosome that hybridized with 3p (RP11-129B22), labeled by nick translation with Texas Red (Vysis Inc., Downer's Grove, IL, USA).
Hybridization was carried out according to the manufacturer's instructions with slight modifications. The slides were deparaffinized, boiled in a pressure cooker with 1 mM EDTA (pH 8.0) for 10 min, and incubated with pepsin at 37°C for 30 min. The slides were then dehydrated. The probe was denatured at 75°C for 1 min before overnight hybridization at 37°C in a humid chamber. Slides were washed with 0.4 × SSC and 0.3% NP40.
Cell images were captured by using a cooled charge-coupled device (CCD) camera (Photometrics SenSys camera) connected to a computer running the Chromofluor image analysis system (Cytovision; Applied Imaging Ltd, New Castle, UK).
VHL gene analysis
Mutation analysis
Direct sequencing of the three exons of the VHL gene was carried out.29 Primers and conditions were as described elsewhere.30
Methylation status of the VHL CpG islands, Southern blot, and multiplex ligation-dependent probe amplification (MLPA)
The methylation status of the VHL CpG islands was analyzed by using the methylation-specific polymerase chain reaction (MSP).31 The MSP technique applied for VHL gene has been previously described by us.32
Southern blot33 and MLPA were used to detect great rearrangements in the VHL gene. In our work, these techniques were used for those tumor samples in which no VHL mutations were found. MLPA technique was performed by following the manufacturer's instructions using 200 ng of DNA (SALSA P016 VHL exon deletion test kit, MRC-Holland, Amsterdam).34
Immunohistochemistry
Sections were cut at a thickness of 3 μm, dried for 16 h at 56°C before being dewaxed in xylene, and rehydrated through a graded ethanol series to phosphate-buffered saline. Antigen retrieval was heat mediated in a pressure cooker treated for 2 min in a 10 mM citrate buffer (pH 6.5) with an additional proteinase K treatment (10 min at room temperature). Before staining the sections, endogenous peroxidase was blocked.
Immunohistochemical staining of FHIT (Zymed, San Francisco, USA) was performed at a dilution of 1:300 for 30 min at room temperature. After washing, the sections were incubated in a biotinylated secondary rabbit anti-rat (Dako, Glostrup, Denmark) for 30 min, followed by peroxidase-labeled streptavidin (Dako).
Immunohistochemical staining of VHL (NeoMarkers-Labvision, Fremont, CA, USA) was performed at a dilution of 1:10 for 40 min at room temperature. The Visualization System was EnVision (DakoCytomation, Glostrup, Denmark).
After incubation, sites of peroxidase activity were developed by using 3,3-diaminobenzidene chromogen as a substrate. Sections were counterstained with hematoxylin. A positive control was included with each batch of staining to ensure consistency between each consecutive run. Immunohistochemical staining was performed on an automated immunostainer (Techmate 500, Dako, Glostrup, Denmark).
A non-neoplastic kidney tissue adjacent to the tumor served as positive internal control.
Array-based CGH (aCGH)
A 1-Mb resolution aCGH35 was used in order to explore possible microdeletions that could be taking place in the remaining 3p within those tumors without alterations in the VHL gene (IV-22, IV-35, and V-5 (R)).
Methods and conditions were as described previously.35
Results
A summary of the results is shown in Table 1.
Familial t(3;8)
At present, 36 living members have been studied to determine their translocation carrier status (Figure 1). Of these, 16 were demonstrated carriers and five deceased individuals were deduced to carry the familial translocation (Figure 2). Eight family members belonging to four generations (III-1, III-11, III-16, III-18, IV-3, IV-22, IV-31, and V-5) developed bilateral CRCC and only one, IV-32, developed unilateral CRCC, all of them being carriers of the constitutional translocation. Two carriers (II-2 and IV-3) presented gastric tumors. On the other hand, noncarrier family members also developed other types of tumors (papillary renal cell carcinoma, breast cancer, and lymphoma).

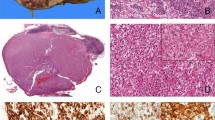
Multistep model in the t(3;8)(p14.1;q24.23) family. (A) Peripheral blood karyotype from a t(3;8) carrier. (B) Loss der(3p) in CRCC detected by CGH in all CRCC tumors. (C) FISH on touch imprint cytologies of normal and tumor samples (case IV-22). Green signal corresponds to CEP 8, and red signal to CEP 17. (a) No loss of der(3p), green signal, was observed in any of the normal renal cells analyzed. (b) Loss of one copy of CEP 8, loss of der(3p), was detected in approximately 50% of tumoral cells analyzed. (D)VHL gene studies in the tumors. (a) VHL mutation analysis: CD123delG detected in the tumor V-5(L). (b) Promoter hypermethylation analysis (IV-31); U=unmethylated, M=methylated. (c) Negative result of gross deletions studied by Southern blot (case IV-31).
CGH and FISH analyses
We carried out a CGH analysis in renal tumor samples in order to detect copy number changes. The analysis of six tumoral DNA samples belonging to four individuals (two of IV-3, studied by Melendez et al,14 IV-22, IV-31, and two of V-5) showed the loss of the derivative chromosome 8, which includes the 3p segment, der(3p), as the sole imbalance in all cases (Figure 2). No changes were observed in the normal kidney tissue from IV-22 and IV-31 members (Table 1). These results from the normal tissue were according to the normal karyotype obtained after culture from the fresh IV-22 (N) sample. The loss of der(3p) of tumor and normal samples was tested by means of FISH, and these showed that der(3p) loss was not present in all cells (around 50% of the nuclei), while this loss was not detected in the normal samples (Table 1 and Figure 2).
VHL
To verify the third hit of the proposed model for the development of CRCC in this family, a VHL gene mutational study on tumoral DNA was performed. We studied six tumor samples from four family members and we found three different VHL mutations (Table 1): D123delG, present in the tumor from patient V-5 (L), and R161P and L118P exhibited in two different samples from the same patient IV-3, as described by Meléndez et al.14 The remaining three analyzed tumors from patients IV-22, IV-31, and V-5 (R) showed no VHL mutations, and neither did the normal tissues studied.
The next step in these three samples without VHL mutation was the detection of gross deletions (by Southern blot and/or MLPA), and the hypermethylation study of VHL by MSP technique. Neither gross deletion nor CpG island hypermethylation of the VHL gene were found (Table 1 and Figure 2).
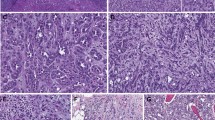
In order to discard the fact that any other kind of mechanism of inactivation could be acting on the expression of VHL in these samples with no apparent genetic or epigenetic alterations, we performed an immunohistochemical analysis of the VHL protein. As expected, the three samples with VHL mutation showed lack of expression of the protein, and the three tumors with an apparently normal VHL gene showed a variable range of expression values: normal in the tumor of case V-5 (R), nonconclusive value in IV-22, and nondetectable in case IV-31 (Figure 3). Normal expression of the protein was observed in normal renal tissues (IV-22 (N)) and IV-31 (N)). In order to test the accuracy of the immunohistochemistry in these kinds of tumors, we studied five sporadic CRCC: four out of five tumors carried mutation in the VHL gene and none of these expressed the protein, while the case without the VHL mutation did.

Immunohistochemistry of VHL and FHIT proteins. (a) VHL expression and lack of expression in cases V-5 (R) and IV-3 (L), respectively. (b) FHIT expression and lack of expression in cases IV-3 (R) and IV-31, respectively.
aCGH
To study if small microdeletions in the remaining 3p were taking place, we performed aCGH technique by using a 1-Mb resolution aCGH in three cases without VHL mutation (IV-22, IV-31, and V-5 (R)). Taking into account that not all tumoral cells lose der(3p), which includes part of 3p arm (p14.1 → pter) and most of chromosome 8 (8pter → 8q24.23), we considered the level of loss of chromosome 8 as the internal control of one loss.
Using this technique, we have not been able to distinguish homozygous microdeletions that could be affecting the nonlost 3p arm. BACs located in 3p were lost at the same level as those located in chromosome 8 (data not shown).
FHIT
We decided to study the expression of the FHIT protein in order to check its role as a tumor suppressor gene in families with chromosome 3 translocation and to determine whether FHIT could be an alternative pathway to that of VHL. Immunohistochemistry was performed on five samples: IV-3 (L), IV-3 (R), IV-22, IV-31, and V-5 (L). A wide variety of results were found as shown in Table 1: IV-3 (L) and V-5 (L) tumor samples with mutated VHL, showed the absence or reduction of FHIT expression, while IV-3 (R), also with VHL mutation, expressed the protein normally (Figure 3). On the other hand, the two samples studied without VHL alterations, IV-22 and IV-31, showed normal and no expression results, respectively. Expression of the protein was detected in normal renal tissues (IV-22 (N) and IV-31 (N)).
Other tumors
Patient IV-3 developed a gastric tumor at the age of 49, 3 years after having being diagnosed of bilateral CRCC. In addition to this, another member of the family (II-2), an obliged translocation carrier, died of gastric cancer. In order to prove or discard a possible relationship with the constitutional translocation, different studies were performed using DNA extracted from a frozen gastric tumor sample of IV-3 (Table 1). CGH analysis did not show loss of the chromosome derivative harboring the 3p segment and no alterations were detected in the VHL gene. LOH studies with molecular markers located on 3p and part of the q arm were also performed. The LOH results confirmed the results obtained by CGH in which no 3p loss was detected. We performed immunohistochemistry of VHL and FHIT proteins and both were expressed normally.
Discussion
Few families with hereditary CRCC and constitutional translocations involving chromosome 3p have been described. However, until now, no candidate genes have been cloned and an alternative model of three hits has been proposed in order to explain this atypical situation. This includes: (a) presence of the constitutional translocation, (b) loss of 3p in the tumor, and (c) mutation in a suppressor gene (VHL gene) in the remaining chromosome 3. In order to analyze this model in depth, and to give some answers to the questions above, we have extended our study in the family previously identified with three CRCC affected members and t(3;8)(14.1;q24.23).14 Moreover, for this translocation, we cloned the breakpoints of the two involved chromosomes and we did not find genes in these regions.20 In subsequent clinical controls and periodic advising, another seven cases of CRCC were diagnosed or reported. This allowed us to fully describe and analyze 36 members through four generations (Figure 1), and to study tumor and normal samples from the affected members.
In this family, we have observed high variability in the age of onset and an anticipation phenomenon through the generations: the three members of the II generation, obliged carriers of the t(3;8), died at over 70 years of age and none of them had developed CRCC. In the following generation (III), the range of ages of onset is 56–82 years; in generation IV, 39–49; and in the last generation, one member has developed a bilateral form of the neoplasia at 25 years of age. The reason as to why this happens is not known, although some speculations have been proposed for other kinds of hereditary syndromes,36 such as the role of genomic imprinting, or environmental interactions, as it has been observed for BRCA1 and two positive hereditary breast cancers.37 In any case, the anticipation in the age of onset phenomenon is very important with regard to genetic counseling, in order to determine when these members should be studied to start the clinical follow-up.
In this large family, we have observed incomplete penetrance: two carriers in the III generation of 71 and 75 years of age have not yet developed CRCC and the three members of the II generation died over 70 without neoplasia. Although the risk of developing the bilateral form of CRCC is very high in these families, we cannot determine exact figures of risk on account of the few cases reported.
The three-step model in CRCC associated with t(3;8)(p14.1;q24.23): only three steps?
The three-step model previously proposed includes der(3p) loss in the tumoral samples as a second step. In our family, the six tumor samples analyzed by CGH presented der(3p) loss (Table 1), and the same phenomenon has been reported in most of the other chromosome 3 translocation families.6, 10, 11, 12, 21, 38 Including our data, more than 90% of the reported cases showed loss of the derivative chromosome carrying the 3p segment, confirming that 3p loss is a critical step in the genesis of CRCC. We investigated if the loss of der(3p) was also present in normal renal tissue by using FISH analysis in samples from IV-22 and IV-31 members. We demonstrated that normal cells did not show the der(3p) loss, by CGH and FISH, and that only a proportion of the tumor cells actually presented this aberration. The loss of der(3p) assessed by CGH in renal tumor samples was detected by FISH in around 50% of the nuclei (Table 1 and Figure 2). These results suggest that an additional genetic event should antecede the loss of 3p, playing a role in the normal to tumor transformation. This hypothesis was also suggested by Eleveld et al when they did not find the loss of der(3p) in two out of five CRCC samples belonging to a family with t(3;6)(q12;q15). So, tumorigenesis may be initiated in these families by other genetic and/or microenvironmental changes affecting chromosome stability.
The third step in this model includes the mutation of a suppressor gene located in the other normal chromosome 3. As VHL families develop CRCC in some cases, VHL gene was considered to be a good candidate and it has been found mutated in about 50% of the tumors of individuals with 3p translocations. In our tumor samples, VHL is only mutated in three of the six tumors (50%) (Table 1), a similar result to previous reports. In addition, we have not detected mutations in the normal renal tissues analyzed. To exclude other inactivation mechanisms affecting the VHL gene, we analyzed the presence of gross deletions and the methylation status in the three cases without mutation. For these three CRCCs, no genetic or epigenetic alterations in the VHL gene were identified, but immunohistochemistry revealed the lack of expression of the protein in at least one of the tumors (IV-31). In this case, another mechanism of inactivation, different from those we have studied, might be acting on the VHL gene. It is very significant that after different approaches, only 65% of tumors exhibited alterations involving VHL gene (4/6, including case IV-31). In fact, one of the tumors without apparent VHL alteration expressed normal level of the VHL protein. These results question the role of the VHL gene as a mandatory step in the development of CRCC, strongly supporting the existence of other notyet identified tumor suppressor genes located in 3p with much importance for the genesis of kidney tumors.
We studied the expression FHIT gene in order to check whether alterations in this gene could explain those cases without VHL alteration. The FHIT gene is located at chromosome 3p and was cloned in t(3;8)(p14;q24) of a family with CRCC.39 Ohta et al40 suggested that the FHIT gene would be a candidate for the initiation of familial and sporadic CRCC. However, the role of FHIT as a tumor suppressor gene is still controversial because (1) genomic deletions and point mutations are uncommon, (2) aberrant FHIT mRNA transcripts have also been identified in non-neoplastic tissues,41, 42, 43 and (3) immunohistochemical studies have shown variable results among CRCC tumors.
Our results did not show any correlation between VHL and FHIT expression, indicating that FHIT does not seem to be an alternative pathway to VHL. We have also confirmed these results for sporadic cases (data not shown).
aCGH technique was performed in order to detect microdeletions in the remaining 3p in the cells that lose the der(3p) of the tumors without VHL alteration. In the three analyzed cases, we have not been able to detect homozygous microdeletions, but taking into account that the array used has a 1-Mb resolution, this could be making us miss the detection of deletions in the gaps. However, microdeletions as a second hit would be a very rare mechanism and it is difficult to think of it as a generalized event.
A gastric tumor developed by a translocation carrier does not follow the multistep tumorigenesis mechanism
Although the risk for developing bilateral CRCC is very high in this family (8/9 members), the risk of second tumors, different from CRCC, seems to be low, which is supported by similar observations in other chromosome 3 translocation families.13 The majority of the members of the present family with other tumors were not carriers of translocation, except for the two members with gastric cancer. Member II-2, a compulsory translocation carrier, died of this tumor, and the probandus developed a gastric cancer at the age of 49 years, after bilateral CRCC. We studied this tumor but we found neither loss of the 3p by CGH nor VHL gene alteration, and FHIT expressed normally. These results suggest that, either this is a sporadic cancer that has coincided with a hereditary syndrome or that although related to the translocation, the tumorigenesis pathway is different from that of CRCC in the family. The last alternative could be supported by the early age of onset of the gastric cancer (49) and by the fact that another translocation carrier of this family died of this tumor. To our knowledge, in the other reported families with chromosome 3 translocations associated with high risk of CRCC, no other non-CRCC tumors developed by translocation carriers have been studied.5, 7, 10, 38 We consider that the study of other nonrenal tumors developed by translocation carriers would be useful to prove that the multistep tumorigenesis mechanism is specific of renal tumors.
In summary, in the large t(3;8) family that we have studied, we confirmed the multistep model previously proposed. However, based on our FISH data, we propose that a step previous to the loss of the 3p (genetic instability?) should happen in the origin of the tumor. A gastric tumor developed by a translocation carrier does not follow the same mechanism of tumorigenesis. Finally, our data question the role of VHL gene as a mandatory step in all CRCC cases, strongly supporting the existence of other not yet identified tumor suppressor genes located in 3p (we discard the FHIT gene as an alternative pathway to VHL, and microdeletions, studied by aCGH, as a possible mechanism of inactivation of a region in the remaining 3p). New studies analyzing other candidate genes on 3p will help to understand the genetic origin of these tumors.
References
Maher ER, Bentley E, Yates JR et al: Mapping of the von Hippel-Lindau disease locus to a small region of chromosome 3p by genetic linkage analysis. Genomics 1991; 10: 957–960.
Maher ER, Bentley E, Yates JR et al: Mapping of von Hippel-Lindau disease to chromosome 3p confirmed by genetic linkage analysis. J Neurol Sci 1990; 100: 27–30.
Maher ER : The gene for von Hippel-Lindau disease. BMJ 1993; 307: 279–280.
Bodmer D, van den Hurk W, van Groningen JJ et al: Understanding familial and non-familial renal cell cancer. Hum Mol Genet 2002; 11: 2489–2498.
Cohen AJ, Li FP, Berg S et al: Hereditary renal-cell carcinoma associated with a chromosomal translocation. N Engl J Med 1979; 301: 592–595.
Kovacs G, Brusa P, De Riese W : Tissue-specific expression of a constitutional 3;6 translocation: development of multiple bilateral renal-cell carcinomas. Int J Cancer 1989; 43: 422–427.
Koolen MI, van der Meyden AP, Bodmer D et al: A familial case of renal cell carcinoma and a t(2;3) chromosome translocation. Kidney Int 1998; 53: 273–275.
Eleveld MJ, Bodmer D, Merkx G et al: Molecular analysis of a familial case of renal cell cancer and a t(3;6)(q12;q15). Genes Chromosomes Cancer 2001; 31: 23–32.
Druck T, Podolski J, Byrski T et al: The DIRC1 gene at chromosome 2q33 spans a familial RCC-associated t(2;3)(q33;q21) chromosome translocation. J Hum Genet 2001; 46: 583–589.
Kanayama H, Lui WO, Takahashi M et al: Association of a novel constitutional translocation t(1q;3q) with familial renal cell carcinoma. J Med Genet 2001; 38: 165–170.
Kovacs G, Hoene E : Loss of der(3) in renal carcinoma cells of a patient with constitutional t(3;12). Hum Genet 1988; 78: 148–150.
Kajaczek S, Gronwald J, Kata G, Borowka A, Lubinski J : Familial clear renal cell cancer (CRCC) associated with constitutional reciprocal translocation t(2;3)(q33;q21). Cytogenet Cell Genet 1999; 85: 172.
Geurts van Kessel AWH, Bodmer D, Eleveld M et al: Renal cell cancer: chromosome 3 translocations as risk factors. J Natl Cancer Inst 1999; 91: 1159–1160.
Melendez B, Rodriguez-Perales S, Martinez-Delgado B et al: Molecular study of a new family with hereditary renal cell carcinoma and a translocation t(3;8)(p13;q24.1). Hum Genet 2003; 112: 178–185.
Glover TW, Coyle-Morris JF, Li FP et al: Translocation t(3;8)(p14.2;q24.1) in renal cell carcinoma affects expression of the common fragile site at 3p14(FRA3B) in lymphocytes. Cancer Genet Cytogenet 1988; 31: 69–73.
Gemmill RM, West JD, Boldog F et al: The hereditary renal cell carcinoma 3;8 translocation fuses FHIT to a patched-related gene, TRC8. Proc Natl Acad Sci USA 1998; 95: 9572–9577.
Bodmer D, Schepens M, Eleveld MJ, Schoenmakers EF, Geurts van Kessel A : Disruption of a novel gene, DIRC3, and expression of DIRC3-HSPBAP1 fusion transcripts in a case of familial renal cell cancer and t(2;3)(q35;q21). Genes Chromosomes Cancer 2003; 38: 107–116.
Bodmer D, Eleveld M, Kater-Baats E et al: Disruption of a novel MFS transporter gene, DIRC2, by a familial renal cell carcinoma-associated t(2;3)(q35;q21). Hum Mol Genet 2002; 11: 641–649.
Chen J, Lui WO, Vos MD et al: The t(1;3) breakpoint-spanning genes LSAMP and NORE1 are involved in clear cell renal cell carcinomas. Cancer Cell 2003; 4: 405–413.
Rodriguez-Perales S, Melendez B, Gribble SM et al: Cloning of a new familial t(3;8) translocation associated with conventional renal cell carcinoma reveals a 5 kb microdeletion and no gene involved in the rearrangement. Hum Mol Genet 2004; 13: 983–990.
Bodmer D, Eleveld M, Ligtenberg M et al: Cytogenetic and molecular analysis of early stage renal cell carcinomas in a family with a translocation (2;3)(q35;q21). Cancer Genet Cytogenet 2002; 134: 6–12.
Bodmer D, Eleveld MJ, Ligtenberg MJ et al: An alternative route for multistep tumorigenesis in a novel case of hereditary renal cell cancer and a t(2;3)(q35;q21) chromosome translocation. Am J Hum Genet 1998; 62: 1475–1483.
Woodward ER, Clifford SC, Astuti D, Affara NA, Maher ER : Familial clear cell renal cell carcinoma (FCRC): clinical features and mutation analysis of the VHL, MET, and CUL2 candidate genes. J Med Genet 2000; 37: 348–353.
Knudson Jr AG : Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci USA 1971; 68: 820–823.
Kovacs G : Molecular cytogenetics of renal cell tumors. Adv Cancer Res 1993; 62: 89–124.
Kovacs G, Kung HF : Nonhomologous chromatid exchange in hereditary and sporadic renal cell carcinomas. Proc Natl Acad Sci USA 1991; 88: 194–198.
Mitelman F : ISCN. An International System for Human Cytogenetic Nomenclature. Basel: S Karger, 1995.
Kallioniemi OP, Kallioniemi A, Piper J et al: Optimizing comparative genomic hybridization for analysis of DNA sequence copy number changes in solid tumors. Genes Chromosomes Cancer 1994; 10: 231–243.
Latif F, Tory K, Gnarra J et al: Identification of the von Hippel-Lindau disease tumour suppressor gene. Science 1993; 260: 1317–1320.
Chen F, Kishida T, Yao M et al: Germline mutations in the von Hippel-Lindau disease tumor suppressor gene: correlations with phenotype. Hum Mutat 1995; 5: 66–75.
Herman JG, Graff JR, Myohanen S, Nelkin BD, Baylin SB : Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc Natl Acad Sci USA 1996; 93: 9821–9826.
Cascon A, Ruiz-Llorente S, Fraga M et al: Genetic and epigenetic profile of sporadic pheochromocytomas. J Med Genet 2004; 41: e30.
Ruiz-Llorente S, Bravo J, Cebrian A et al: Genetic characterization and structural analysis of VHL Spanish families to define genotype–phenotype correlations. Hum Mutat 2004; 23: 160–169.
Schouten JPMCJ, Waaijer R, Zwijnenburg D, Diepvens F, Pals G : Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acid Res 2002; 30.
Greshock J, Naylor TL, Margolin A et al: 1-Mb resolution array-based comparative genomic hybridization using a BAC clone set optimized for cancer gene analysis. Genome Res 2004; 14: 179–187.
Dagan E, Gershoni-Baruch R : Anticipation in hereditary breast cancer. Clin Genet 2002; 62: 147–150.
King MC, Marks JH, Mandell JB : Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 2003; 302: 643–646.
Li FP, Decker HJ, Zbar B et al: Clinical and genetic studies of renal cell carcinomas in a family with a constitutional chromosome 3;8 translocation. Genetics of familial renal carcinoma. Ann Intern Med 1993; 118: 106–111.
Boldog FL, Gemmill RM, Wilke CM et al: Positional cloning of the hereditary renal carcinoma 3;8 chromosome translocation breakpoint. Proc Natl Acad Sci USA 1993; 90: 8509–8513.
Ohta M, Inoue H, Cotticelli MG et al: The FHIT gene, spanning the chromosome 3p14.2 fragile site and renal carcinoma-associated t(3;8) breakpoint, is abnormal in digestive tract cancers. Cell 1996; 84: 587–597.
Croce CM, Sozzi G, Huebner K : Role of FHIT in human cancer. J Clin Oncol 1999; 17: 1618–1624.
Druck T, Berk L, Huebner K : FHITness and cancer. Oncol Res 1998; 10: 341–345.
Mao L : Tumor suppressor genes: does FHIT fit? J Natl Cancer Inst 1998; 90: 412–414.
Acknowledgements
This work was partially supported by the Consejería de Sanidad of the Autonomous Community of Madrid (CAM). Laura Valle holds a Fellowship from the CAM. We thank Ma Carmen Carralero, Ma Carmen Martín, and Rocío Letón for technical assistance, Marta Cuadros for her help in the LOH study, and Ellen Alacid for linguistic corrections.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Valle, L., Cascón, A., Melchor, L. et al. About the origin and development of hereditary conventional renal cell carcinoma in a four-generation t(3;8)(p14.1;q24.23) family. Eur J Hum Genet 13, 570–578 (2005). https://doi.org/10.1038/sj.ejhg.5201371
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5201371
