
Abstract
Study design:
Retrospective cohort study.
Objectives:
Our study aimed to describe the outcome of bloodstream infection (BSI) in spinal cord injury (SCI) patients and their associated risk factors for severity and mortality.
Setting:
A French University Hospital.
Methods:
We conducted a retrospective cohort study of all BSIs occurring in hospitalized SCI patients. We analyzed their outcome and risk factors especially the impact of multidrug-resistant organisms (MDROs).
Results:
Overall, 318 BSIs occurring among 256 patients were included in the analysis. Mean age was 50.8 years and gender ratio (M/F) was 2.70, with a mean injury duration of 11.6 years.
Severity and 30-day mortality of BSI episodes were, respectively, 43.4% and 7.9%. BSI severity was significantly more frequent when caused by respiratory tract infections (RTIs) (odds ratio (OR)=1.38; 95% confidence interval (CI): 1.13–1.44) and significantly lower when caused by urinary tract infections (UTIs) (OR=0.47; 95% CI: 0.28–0.76). BSI mortality was significantly higher when caused by RTIs (OR=3.08; 95% CI: 1.05–8.99), catheter-related bloodstream infections (OR=3.54; 95% CI: 1.36–9.18) or Pseudomonas aeruginosa infections (OR=3.79; 95% CI: 1.14–12.55).
MDROs were responsible for 41.2% of all BSI. They have no impact on severity and mortality, whichever be the primary site of infection.
In multivariate analysis, mortality was higher when BSI episodes were due to RTIs (OR=3.26; 95% CI: 1.29–8.22) and Pseudomonas aeruginosa infections (OR=3.53; 95% CI: 1.06–11.70), or when associated with immunosuppressive therapy (OR=2.57; 95% CI: 1.14–5.78) or initial severity signs (OR=1.68; 95% CI: 1.01–2.81).
Conclusion:
BSI occurring in SCI population were often severe but mortality remained low. MDROs were frequent but not associated with severity or mortality of BSI episodes. Risk factors associated with mortality were initial severe presentation, RTI, immunosuppressive therapy and BSI due to Pseudomonas aeruginosa.
Similar content being viewed by others

Introduction
Nearly 250 000 inhabitants are affected with spinal cord injury (SCI) in the United States, with an annual incidence of 11 000.1 In Europe, SCI incidence varies between 10.4 and 29.4 per million inhabitants.
Infections are the main cause of death in SCI patients, especially bloodstream infections (BSIs).2, 3, 4, 5, 6, 7, 8
Colonizing multidrug-resistant organisms (MDROs) are frequent in the SCI population.7, 9, 10, 11, 12, 13 In the general population, hospital-acquired infections and MDRO infections are associated with increased mortality and increased cost.7 In the SCI population, such infections have been shown to increase the number of hospitalizations and the length of stay.14
The outcome of BSI in SCI has been little studied. Bhatt et al. noticed a hypotension in 5 out of 29 cases (17.1%), although mortality in this population ranges from 1.7 to 29% according to different reports.4, 15, 16, 17
In particular, the outcome of BSI due to MDROs in this population is unknown. In a previous retrospective study on BSI epidemiology in SCI population over 16 years, we concluded that the prevalence of MDROs, which was high, remained stable over the years. Also, it was not significantly different regarding age, gender, type and duration of SCI, primary site of infection or bacteria species involved.9
From this large cohort, we studied the severity and mortality of BSI according to the primary site of infection and according to the drug resistance characteristics of the microorganisms involved.
Material and methods
Settings and design
We performed a retrospective cohort study. We identified all patients hospitalized at our teaching Hospital (R. Poincaré, Garches, France), from 1 July 1998 to 31 October 2013, with an international classification disease 10th version (ICD-10). It included paraplegia or quadriplegia, and positive blood cultures for bacteria.
Then, we reviewed medical charts and excluded any code mistakes. The microbiological data, as well as demographic characteristics, risk factors and outcomes were recovered from the local computerized medical entry and medical charts.
Because of its retrospective design, no ethical advice and written consent from patients were needed for this study.
Definitions
Case definition
BSI case was defined as the association of the following:
-
At least one positive blood culture. For common skin contaminants (e.g., coagulase-negative Staphylococci diphteroids and so on), at least two different sets of blood cultures were required.
-
A prescription of a systemic antibiotic treatment to treat the BSI.
Polymicrobial BSI was defined as having more than one organism found in the same BSI episode.
Microbiological definitions
During the study, different identification methods were used. Until May 2011, Gram-negative bacilli, except for Pseudomonas aeruginosa and Stenotrophomonas maltophilia, were phenotypically identified by the API 20E biochemical identification system (BioMérieux, Lyon, France). P. aeruginosa and S. maltophilia were identified by the API 20 NE biochemical identification system (BioMérieux). The identification of Staphylococci was based on the coagulase test (Bio-Rad, Paris, France), and the identification of Enterococci was based on the use of tellurite and bile esculin agar media (BD Diagnostics, Sparks, NV, USA). After May 2011, all isolates were identified by mass spectrometry (Bruker, Bremen, Germany).
Anti-microbial susceptibility was tested using the agar disk diffusion method (Bio-Rad) or an automated broth microdilution method (Phoenix, BD Diagnostics, Oxford, UK), with susceptibility breakpoints defined by the French Committee for Anti-microbial Susceptibility Testing.
MDRO status was confirmed after antibiotic susceptibility reviewing and comparison with the definitions described in Table 1.
Confirmation of extended-spectrum β-lactamase activity was determined according to the National Committee for Clinical Laboratory Standards.10, 11 Extended-spectrum β-lactamases are enzymes produced by bacteria (also known as penicillinase) that provide multiresistance to β-lactam antibiotics such as penicillins and cephalosporins.
Primary site of infection
Primary site of infection was defined clinically by the physician in charge (reported in medical chart), or bacteriologically (same bacterial identification as in the blood culture). Primary sites were categorized as follows: urinary tract infection (UTI), pressure sore, catheter-related BSI, osteoarticular infection (OAI), respiratory tract infection (RTI), others (including skin and soft tissue infection and intra-abdominal infection) and unknown when no primary site had been identified.
Severity
Severity was defined as the requirement of at least one of the following criteria: volume expansion, assisted (mechanical) ventilation, vasopressor requirement and intensive care unit admission during the episode.
Mortality
Mortality was defined as death of the patient within 30 days following BSI episode.12
Immunosuppressive therapy
Immunosuppressive therapy was defined as corticotherapy, chemotherapy or immunosuppressive treatment such as cyclophosphamide, azathioprine and cyclosporine.
Statistical analysis
All continuous variables were presented as mean (m) and standard deviation (s.d.), and the categorical variables were presented as frequencies.
Correlations between risk factors and characteristics of BSI in patients with SCI and outcome (mortality and severity) were determined by Student’s t-test for continuous variables and the Pearson's χ2 test for categorical variables.
Multivariate analyses were performed to assess the relationship between all associated risks that had a P-value ⩽0.2. The Hosmer–Lemeshow statistic was calculated to assess the model's goodness of fit. Odds ratio (OR) was calculated from the multivariate analyses to quantify association with severity and mortality with a confidence interval (CI) of 95%. An OR >1 was considered to be associated with severity or mortality.
All reported probability values (P-values) were based on two-sided tests, and a P-value <0.05 was considered statistically significant.
All analyses were performed using the SPSS 17.0 software (SPSS Inc., Chicago, IL, USA).
Results
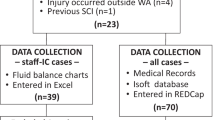
A total of 396 positive blood cultures were detected among 317 patients; 78 episodes (61 patients) were excluded because the microorganism involved was considered a contaminant. Overall, we included 318 episodes of BSI occurring among 256 patients. Table 2 shows the global sociodemographic and clinical characteristics of the study population.
The median age of the cohort was 50.8±17.0 years and the gender ratio (M/F) was 2.70. The mean duration of spinal cord injury was 11.6 years (Table 2).
Primary site of infection was identified in 91% of BSI. They were mainly UTI (34.0%) and pressure sore (25.2%), then catheter-related BSIs (11.3%) and RTI (8.5%) (Table 2).
There were 351 microorganisms identified in all 318 BSI episodes; 31 episodes (9.7%) were polymicrobial.
The most frequent pathogens identified were Enterobacteriaceae in 44.3% of cases (n=141). They were followed by Staphylococcus aureus (n=84; 26.4%), Pseudomonas aeruginosa (n=22; 6.9%), Streptococcus spp. (n=32; 10.1%) and Enterococcus spp. (n=16; 5%) (Table 2).
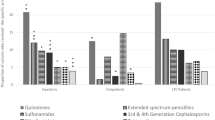
MDROs were involved in 41.2% of BSI and were distributed as follows: 53.4% of Enterobacteriaceae (Escherichia coli (n=26), Klebsiella spp. (n=13), Proteus spp. (n=7), Enterobacter spp. (n=5), Morganella spp. (n= 3), Citrobacter spp. (n=3), Providencia spp. (n=2) and Serratia spp. (n=1)), 32.8% of Staphylococcus aureus (methicillin-resistant) and 6.1% of Pseudomonas aeruginosa.
Median anti-microbial treatment duration varied from 12 to 15 days, except for OAI with a median duration of 45 days (Table 3).
Empiric treatments were microbiologically effective in 78% of the cases.
UTI were mostly treated by parenteral third-generation cephalosporins associated with aminoglycosides. Pressure sore, RTI and catheter-related BSIs were mostly treated by glycolipopeptides associated with aminoglycosides. OAIs were predominantly treated by penicillin and aminoglycosides (Table 4).
Treatment durations according to bacterial species are presented in Supplementary Appendix 1. More than 60% of the patients received combination therapy, especially when treating Pseudomonas aeruginosa infections, even if it did not involve MDR strains (Supplementary Appendix 2). The most prescribed associations were β-lactam with aminoglycosides regarding Pseudomonas aeruginosa and Enterobacteria infections (Supplementary Appendix 3).
At initial presentation, 43.4% of BSI episodes were considered severe, corresponding mostly to intensive care unit admission and volume expansion (Table 2).
Regarding the primary site of infection, UTI and OAI were associated with less frequent severity (respectively, OR=0.47; 95% CI: 0.28–0.76; P=0.002; OR=0.13; 95% CI: 0.03–0.61; P=0.003), contrary to RTI (OR=1.38; 95% CI: 1.13–1.44; P<10−4) (Table 5).
The mortality rate was 7.9% (Table 2). Studying the relationship between mortality and primary site of infection, UTI was significantly associated with less mortality (OR=0.15; 95% CI: 0.03–0.66; P=0.004). On the contrary, RTI (OR=3.08; 95% CI: 1.05–8.99; P=0.031) and catheter-related BSIs (OR=3.54; 95% CI: 1.36–9.18; P=0.006) were associated with a higher mortality (Table 5).
Considering BSI severity and mortality, we performed several analyses comparing these outcomes according to bacterial species (Table 6). BSI due to Pseudomonas aeruginosa was significantly associated with a higher mortality (OR=3.79; 95% CI: 1.14–12.55).
Also, there was no significant difference in severity presentation or mortality while comparing MDRO and non-MDRO groups (respectively, P=0.981 and P=0.306).
In multivariate analysis (Table 7), the following factors were independently associated with a higher mortality: immunosuppressive therapy (OR 2.57; 95% CI: 1.14–5.78; P=0.022), RTI (OR 3.26; 95% CI: 1.29–8.22; P=0.012), BSI due to Pseudomonas aeruginosa (OR=3.53; 95% CI: 1.06–11.70; P=0.039) and presence of initial severity sign (OR 1.68; 95% CI: 1.01–2.81; P=0.045).
Discussion
Despite the frequency of BSI episodes in SCI population, only few studies have reported their outcome. In our study, BSIs were often severe (43.4%), but the mortality rate remained low (7.9%). Moreover, severity was higher when BSI was due to RTI, and mortality rate was higher when BSI was caused by RTI, catheter-related BSIs or Pseudomonas aeruginosa. On the contrary, BSI seemed less severe and with a better outcome when the primary site was a UTI or an OAI. Also, being infected with MDROs had no impact on the severity or the mortality of the episode. A higher mortality in this population was independently associated with RTI, Pseudomonas aeruginosa infections, immunosuppressive therapy and initial severity signs.
Our study’s population was a chronic SCI population with similar characteristics than previous data from literature.3, 15, 16, 17
The median age of our study population was inferior to median age of general population suffering from BSI found in the literature.13
We reported a high proportion of episodes with severe presentation, mostly due to intensive care unit admission, volemic expansion, mechanical ventilation and vasopressor requirement. This high rate of severe cases has not yet been reported. However, really few studies are available on this topic. Only Bhatt et al.16 in their study described hypotension in 5 out of 29 cases (17.1%). This could be due to the difficulty to diagnose sepsis in SCI patients and the delay before hospitalization.
In the general population, the usual mortality rate in BSI varies from 30% to 50%.14, 18 In SCI population, according to several reports, it varies from 1.7% to 29%.4, 15, 16, 17 The low rate of mortality in this specific population could be explained by the young age of the patients compared with the general population.
Outcome depending on the primary site of infection
When focusing on the primary site of infection, UTI was associated with a significant lower mortality rate, contrary to RTI and catheter-related BSIs. This is consistent with the literature: RTI is well known to have a high mortality rate in SCI population3, 7 and UTI to be less fatal than others infections.3, 17
Indeed, DeVivo et al.19 have shown that pneumonia is the most common cause of death after SCI in all age groups. Severe bacterial pneumonias are often accompanied with bacteremia in this population, especially in patients undergoing mechanical ventilation.
However, the high mortality rate associated with catheter-related BSIs could be due to their occurrence mostly in intensive care unit. Therefore, it could be a marker of fatal prognosis rather than an independent risk factor.
Outcome depending on bacteria species involved
Considering bacterial species, the only significant association was mortality and Pseudomonas aeruginosa species. Pseudomonas aeruginosa is frequently associated with higher mortality up to 21% and could be due to difficult treatment strategy.20
Indeed, few therapeutic options exist for treating BSI due to Pseudomonas aeruginosa. A specific antipseudomonal β-lactam is needed such as ceftazidime or ureidopenicillin (ceftriaxone and cefotaxime are not effective). Moreover, a dual effective therapy is usually required.21
Outcome depending on the presence of MDROs
There is an increasing incidence of infections due to MDROs in the general population, especially due to Enterobacteriaceae and particularly extended-spectrum β-lactamase and carbapenemase producers.22 In our previous study, we found no significant increase of MDROs in SCI population.9
Infections due to MDROs could be associated with an increased mortality. As shown by Kang et al.,23 during BSI due to Enterobacter species in non-SCI population, the 30-day mortality rate was significantly higher when a broad-spectrum cephalosporin-resistant Enterobacter was involved (3.7% vs 18.6%; P=0.021).23 Moreover, Deal et al.24 identified resistance to second- or third-generation cephalosporins and to trimethoprim-sulfamethoxazole as independent risk factors for mortality during BSI caused by Enterobacter species or Citrobacter freundii (respectively, adjusted OR =5.16; 95% CI: 2.66–10.0; P=0.013 and OR=5.44; 95% CI: 2.53–11.7; P=0.027). At last, Chang et al.25 during Enterobacter aerogenes bacteremia found that resistance to extended-spectrum cephalosporins was an independent risk factor for mortality (OR=9.21; 95% CI: 1.02–83.04; P=0.048).
However, other reports state that MDROs could have no impact on mortality, as suggested by Kim et al.26 They found no difference in BSI caused by resistant or susceptible to extended-spectrum cephalosporins Citrobacter freundii (19.4% vs 25.6%; P=0.45).
Overall, the impact of MDROs during BSI is uncertain. In our study, no impact of MDRO on severity and/or mortality was noted. The main factor could be the adequacy of the initial anti-microbial therapy that has shown its major effect.27 In our center, we are aware of the high prevalence of MDROs in SCI patients and local guidelines recommend an empirical use of broad-spectrum anti-microbial treatment for this population in case of severe sepsis. This attitude could explain the absence of impact of MDROs during BSI among SCI population in our study.
Moreover, some authors suggest that immunity of SCI population is stronger against bacterial aggression because of their recurrent infections that could explain both the low mortality rate (despite the high severity rate) and the absence of impact of MDROs.16, 17, 28 These data should reassure physicians about the favorable prognosis of BSI because of MDROs occurring in disabled population, and reinforce their use of invasive therapeutics.
Outcome depending on independent factors
Finally, the only independent factors associated with 30-day mortality were RTI, immunosuppressive therapy and initial severity. In this situation, handling of such patients should be quickly optimized with prompt intensive care management and broad-spectrum anti-microbial therapy. In a retrospective study on 123 BSIs occurring in 63 SCI patients (mean age 59±2 years), Wall et al.3 reported hypoalbuminemia as the strongest independent predictor for mortality.3 This factor is linked to the initial severity of the episode or to the underlying poor conditions of patients.
The bias and weakness of our study are due to its monocentric and retrospective design. However, it is one of the largest cohorts of patients in relation to this topic to the best of our knowledge.
Therefore, these retrospective results need to be confirmed by future prospective studies. The definition of MDROs could be discussed, but there is no standard definition of anti-microbial resistance, especially for P. aeruginosa and other Gram-negative bacilli. Thus, we used a classification proposed by different authors.10, 11, 29, 30, 31, 32
In our study, MDROs have no impact on severity or mortality, whichever be the primary site of infection.
The only factors associated with higher mortality were RTI (OR=3.26; 95% CI: 1.29–8.22), BSI due to Pseudomonas aeruginosa (OR=3.53; 95% CI: 1.06–11.70), immunosuppressive therapy (OR=2.57; 95% CI: 1.14–5.78) or initial severity signs (OR=1.68; 95% CI: 1.01–2.81).
Despite the difficulties in medical management encountered with such population, mortality remained lower than that in the general population, even in critical situations, which were common. It might be due to the young age of the patients.
Thus, SCI population even with MDROs BSI has a good prognosis when managed by an expert team.
Data archiving
There were no data to deposit.
References
National Spinal Cord Injury Statistical Center Spinal Cord Injury Facts and Figures at a Glance. National Institute of Disability Rehabilitation Research: Washington, DC, USA,. 2015. Available at: https://www.nscisc.uab.edu/Public/Facts2015.pdf (last accessed 20 September 2016).
Lalwani S, Punia P, Mathur P, Trikha V, Satyarthee G, Misra MC . Hospital acquired infections: preventable cause of mortality in spinal cord injury patients. J Lab Physicians 2014; 6: 36–39.
Wall BM, Mangold T, Huch KM, Corbett C, Cooke CR . Bacteremia in the chronic spinal cord injury population: risk factors for mortality. J Spinal Cord Med 2003; 26: 248–253.
Darouiche RO . In: Lin VW, Cardenas DD, Cutter NC, Frost FS, Hammond MC, Lindblom LB et al (eds). Spinal Cord Medicine: Principles and Practice. Demos Medical Publishing LLC: New York, NY, USA. 2003, pp 201.
Evans CT, LaVela SL, Weaver FM, Priebe M, Sandford P, Niemiec P et al. Epidemiology of hospital-acquired infections in veterans with spinal cord injury and disorder. Infect Control Hosp Epidemiol 2008; 29: 234–242.
DeVivo MJ, Stover S . In: Stover SL, DeLisa JA, Whiteneck GG (eds). Spinal Cord Injury: Clinical Outcomes from the Model Systems. Aspen Publications: Gaithersburg, MD, USA. 1995, pp 289–313.
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Evans CT, Hershow RC, Chin A, Foulis PR, Burns SP, Weaver FM . Bloodstream infections and setting of onset in persons with spinal cord injury and disorder. Spinal Cord 2009; 47: 610–615.
Dinh A, Saliba M, Saadeh D, Bouchand F, Descatha A, Roux AL et al. Blood stream infections due to multidrug-resistant organisms among spinal cord-injured patients, epidemiology over 16 years and associated risks: a comparative study. Spinal Cord 2016; 54: 720–725.
NCCLS.Performance standards for Antimicrobial Susceptibility Testing, 25th Informational Supplement, NCCLS, Wayne, PA, USA, Approved standard M100-S25, 2015. http://shop.clsi.org/site/Sample_pdf/M100S25_sample.pdf?bcsi_scan_628cd39dca2568d2=8kbY8qJQWooHYUPyF0AuEjSjOCsdAAAAU/6Kwg==&bcsi_scan_filename=M100S25_sample.pdf. Accessed on 25 November 2016.
Tenover FC, Raney PM, Williams PP, Rasheed JK, Biddle JW, Oliver A et al. Evaluation of the NCCLS extended-spectrum β-lactamase confirmation methods for Escherichia coli with isolates collected during Project ICARE. J Clin Microbiol 2003; 41: 3142–3146.
Lillie PJ, Allen J, Hall C, Walsh C, Adams K, Thaker H et al. Long-term mortality following bloodstream infection. Clin Microbiol Infect 2013; 19: 955–960.
Laupland KB, Gregson DB, Zygun DA, Doig CJ, Mortis G, Church DL . Severe bloodstream infections: a population-based assessment. Crit Care Med 2004; 32: 992–997.
Wenzel RP, Edmond MB . The impact of hospital-acquired bloodstream infections. Emerg Infect Dis 2001; 7: 174–177.
Waites KB, Canupp KC, Chen Y, DeVivo MJ, Moser SA . Bacteremia after spinal cord injury in initial versus subsequent hospitalizations. J Spinal Cord Med 2001; 24: 96–100.
Bhatt K, Cid E, Maiman D . Bacteremia in the spinal cord injury population. J Am Paraplegia Soc 1987; 10: 11–14.
Montgomerie JZ, Chan E, Gilmore DS, Canawati HN, Sapico FL . Low mortality among patients with spinal cord injury and bacteremia. Rev Infect Dis 1991; 13: 867–871.
Weinstein MP, Murphy JR, Reller LB, Lichtenstein KA . The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. Clinical observations, with special reference to factors influencing prognosis. Rev Infect Dis 1983; 5: 54–70.
DeVivo MJ, Black KJ, Stover SL . Causes of death during the first 12 years after spinal cord injury. Arch Phys Med Rehabil 1993; 74: 248–254.
Micek ST, Lloyd AE, Ritchie DJ, Reichley RM, Fraser VJ, Kollef MH . Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment. Antimicrob Agents Chemother 2005; 49: 1306–1311.
Traugott KA, Echevarria K, Maxwell P, Green K, Lewis JS . Monotherapy or combination therapy? The Pseudomonas aeruginosa conundrum. Pharmacotherapy 2011; 31: 598–608.
Lim CJ, Cheng AC, Kennon J, Spelman D, Hale D, Melican G et al. Prevalence of multidrug-resistant organisms and risk factors for carriage in long-term care facilities: a nested case–control study. J Antimicrob Chemother 2014; 69: 1972–1980.
Kang CI, Kim SH, Park WB, Lee KD, Kim HB, Oh MD et al. Bloodstream infections caused by Enterobacter species: predictors of 30-day mortality rate and impact of broad-spectrum cephalosporin resistance on outcome. Clin Infect Dis 2004; 39: 812–818.
Deal EN, Micek ST, Ritchie DJ, Reichley RM, Dunne WM, Kollef MH . Predictors of in-hospital mortality for bloodstream infections caused by Enterobacter species or Citrobacter freundii. Pharmacotherapy 2007; 27: 191–199.
Chang EP, Chiang DH, Lin ML, Chen TL, Wang FD, Liu CY . Clinical characteristics and predictors of mortality in patients with Enterobacter aerogenes bacteremia. J Microbiol Immunol Infect 2009; 42: 329–335.
Kim BN, Woo JH, Ryu J, Kim YS . Resistance to extended-spectrum cephalosporins and mortality in patients with Citrobacter freundii bacteremia. Infection 2003; 31: 202–207.
Kollef MH, Sherman G, Ward S, Fraser VJ . Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest 1999; 115: 462–474.
Montgomerie JZ . Infections in patients with spinal cord injuries. Clin Infect Dis 1997; 25: 1282–1285.
Obritsch MD, Fish DN, MacLaren R, Jung R . Nosocomial infections due to multidrug-resistant Pseudomonas aeruginosa: epidemiology and treatment options. Pharmacotherapy 2005; 25: 1353–1364.
Falagas ME, Karageorgopoulos DE . Pandrug resistance (PDR), extensive drug resistance (XDR), and multidrug resistance (MDR) among Gram-negative bacilli: need for international harmonization in terminology. Clin Infect Dis 2008; 46: 1121–1122.
Falagas ME, Koletsi PK, Bliziotis IA . The diversity of definitions of multidrug-resistant (MDR) and pandrug-resistant (PDR) Acinetobacter baumannii and Pseudomonas aeruginosa. J Med Microbiol 2006; 55: 1619–1629.
Hachem RY, Chemaly RF, Ahmar CA, Jiang Y, Boktour MR, Rjaili GA et al. Colistin is effective in treatment of infections caused by multidrug-resistant Pseudomonas aeruginosa in cancer patients. Antimicrob Agents Chemother 2007; 51: 1905–1911.
Acknowledgements
We are thankful to the patients and Elodie Choisy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on the Spinal Cord website
Rights and permissions
About this article

Cite this article
Saliba, M., Saadeh, D., Bouchand, F. et al. Outcome of bloodstream infections among spinal cord injury patients and impact of multidrug-resistant organisms. Spinal Cord 55, 148–154 (2017). https://doi.org/10.1038/sc.2016.176
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.176
