
Abstract
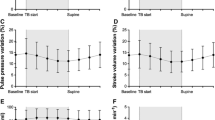
Objective.It is necessary to define a reference systolic arterial blood pressure (RP) to calculate delta-Up (dUp) and delta-Down (dDown) for systolic pressure variation. Most studies define the reference pressure as the average systolic blood pressure during a short period of apnea. We describe an automated systolic pressure variation monitor that measures airway pressure and defines the reference pressure as the systolic blood pressure at end-expiration. The present study compares the reference systolic blood pressure measured at end-expiration by the automated systolic pressure variation monitor and the reference systolic blood pressure measured during apnea to test whether the end-expiration value is an adequate substitute for the value during apnea. Methods.After obtaining informed consent, 108sets of measurements of systolic pressure variation (SPV) were made in 20intubated, mechanically-ventilated, anesthetized patients by the automated SPV monitor and during apnea. Measurements were taken during periods of hemodynamic stability defined as three consecutive end-expiratory systolic blood pressures within four mmHg of each other. The three systolic pressure sat end-expiration were averaged (RP monitor ). Immediately following these measurements, the ventilator was turned off and the systolic blood pressure was measured at 6, 8, 10 and 12 seconds of apnea. The reference pressure during apnea (RP apnea ) was defined as the average of the systolic blood pressure at 8, 10 and 12 seconds of apnea. For each measurement set, RP monitor and the systolic blood pressure at6 seconds of apnea (SBP6) were compared to RP apnea using Bland–Altman analysis. Results.Bland–Altman analysis for the difference between SBP6 and RP apnea yielded a small bias of −0.3 mmHg with standard deviation of 1.3, indicating that the systolic pressure tends to continue to increase slightly after 6seconds of apnea. Results were similar for the difference between RP monitor and RP apnea (−0.2 ± 3.1mmHg). Conclusions.dUp and dDown are calculated using the reference pressure. RP monitor is an average of 0.2 mm Hg less than RP apnea , thus dUp calculated by the automated SPV monitor is an average of 0.2 mm Hg greater than dUp measured by the reference pressure during apnea and dDown is 0.2 mm Hg less. Since the bias of −0.2 mm Hgis clinically insignificant, there is acceptable agreement between the reference pressure obtained during apnea and that obtained by the automated SPV monitor at end-expiration. The mean difference between RP monitor and RP apnea is explained by the continued rise in systolic pressure during the period of apnea as demonstrated by the difference between SBP6 and RP apnea .
Similar content being viewed by others

REFERENCES
Perel A, Pizov R, Cotev S. Systolic blood pressure variation is a sensitive indicator of hypovolemia in ventilated dogs subjected to graded hemorrhage. Anesthesiology 1987; 67: 498-502
Pizov R, Ya'ri Y, Perel A. Systolic pressure variation is greater during hemorrhage than during sodium nitroprusside-induced hypotension in ventilated dogs. Anesth Analg 1988; 67: 170-174
Rooke GA, Schwid HA, Shapira Y. The effect of graded hemorrhage and intravascular volume replacement on systolic pressure variation in humans during mechanical and spontaneous ventilation. Anesth Analg 1995; 80: 925-932
Marik PE. The systolic blood pressure variation as an indicator of pulmonary capillary wedge pressure in ventilated patients. Anaesthesia Intens Care 1993; 21: 405-408
Coriat P, Vrillon M, Perel A, Baron JF, LeBret F, Saada M, Viars P. A comparison of systolic blood pressure variations and echocardiographic estimates of end-diastolic left ventricular size in patients after aortic surgery. Anesth Analg 1994; 78: 46-53
Tavernier B, Makhotine O, Lebuffe G, Dupont J, Scherpereel P. Systolic pressure variation as a guide to fluid therapy in patients with sepsis-induced hypotension. Anesthesiology 1998; 89: 1313-1321
Pizov R, Ya'ari Y, Perel A.The arterial pressure waveform during acute ventricular failure and synchronized external chest compression. Anesth Analg 1989; 68: 150-156
Pizov R, Cohen M, Weiss Y, Segal E, Cotev S, Perel A. Positive end-expiratory pressure-induced hemodynamic changes are reflected in the arterial pressure waveform. Crit Care Med 1996; 24: 1381-1387
Perel A. Assessing fluid responsiveness by the systolic pressure variation in mechanically ventilated patients. Anesthesiology 1998; 89: 1309-1310
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; i: 307-310
Szold A, Pizov R, Perel A. The effect of tidal volume and intravascular volume state on systolic pressure variation in ventilated dogs. Intens Care Med 1989; 15: 368-371
Vedrinne JM, Duperret S, Decaillot F, Gratadour P, Motin J. Haemodynamic changes induced by two I: E ratios: A transoesophageal echocardiographic study. Can J Anaesth 1997; 44: 354-359
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Schwid, H.A., Rooke, G.A. Systolic Blood Pressure at End-Expiration Measured by the Automated Systolic Pressure Variation Monitor is Equivalent to Systolic Blood Pressure during Apnea. J Clin Monit Comput 16, 115–120 (2000). https://doi.org/10.1023/A:1009933029279
Issue Date:
DOI: https://doi.org/10.1023/A:1009933029279