The corona virus disease 2019 (COVID-19) outbreak has increased the prevalence of depressive/anxiety symptoms (Oh et al., Reference Oh, Yang, Suh, Byun, Kim, Kwak and Kim2021). The presence of anxiety and depressive symptoms is up to 56.3% and 39.3% in hospitalized patients by COVID-19 (Li et al., Reference Li, Sun, Liu, Wang, Zhang, Gong and Duan2021). Furthermore, anxiety/depressive symptoms and sleep disorders are also present at a post-COVID phase (Shanbehzadeh, Tavahomi, Zanjari, Ebrahimi-Takamjani, & Amiri-Arimi, Reference Shanbehzadeh, Tavahomi, Zanjari, Ebrahimi-Takamjani and Amiri-Arimi2021). Most studies assessing post-COVID anxiety/depressive symptoms are cross-sectional since they assessed just at one moment. Two recent studies published in Psychological Medicine had described the trajectories of anxiety/depressive levels in the general population during the outbreak. Gambin et al. (Reference Gambin, Oleksy, Sękowski, Wnuk, Woźniak-Prus, Kmita and Bonanno2021) described the trajectory of anxiety/depressive symptoms over the first year of the pandemic in Poland and found that the increased anxiety/depressive levels occurring at the early stages of the lockdown declined in just 10% of individuals, being resilient or chronic in most of them. Saunders, Buckman, Fonagy, and Fancourt (Reference Saunders, Buckman, Fonagy and Fancourt2021) analyzed the trajectory of anxiety/depressive levels in the UK and revealed that most subjects presented low anxiety/depressive symptom severity and evolved positively during the first week after the lockdown. No previous study has investigated the trajectory curve of anxiety/depressive symptoms as post-COVID sequelae. We present here a study investigating the trajectory curves of post-COVID anxiety/depressive symptoms as well as sleep quality, fitted with an exponential trajectory model, in previously hospitalized COVID-19 survivors.
The LONG-COVID-EXP-CM is a multicenter cohort study including individuals with a diagnosis of SARS-CoV-2 (ICD-10 code) by RT-PCR technique and radiological findings hospitalized during the first wave of the pandemic in five urban hospitals of Madrid (Spain). From all patients hospitalized during the first wave, a sample of 400 from each hospital was randomly selected. The Ethics Committees of all hospitals approved the study (HCSC20/495E, HSO25112020, HUFA 20/126, HUIL/092-20, and HUF/EC1517). Informed consent was obtained from all participants.
Patients were scheduled for two telephone interviews conducted by trained healthcare professionals at two follow-up periods with a 5-month period in between. The Hospital Anxiety and Depression Scale (HADS) was used to evaluate anxiety (HADS-A, 7 items, 0–21 points) and depressive (HADS-D, 7 items, 0–21 points) symptoms (Herrmann-Lingen, Buss, & Snaith, Reference Herrmann-Lingen, Buss and Snaith2011). The following cut-off scores suggesting anxiety (HADS-A ⩾12 points) or depressive (HADS-D ⩾10 points) symptoms were considered (Grupo de Trabajo de la Guía de Práctica Clínica, 2008). The Pittsburgh Sleep Quality Index (PSQI, 0–21 points) was used to evaluate sleep quality (Buysse, Reynolds, Monk, Berman, & Kupfer, Reference Buysse, Reynolds, Monk, Berman and Kupfer1989). Poor sleep quality was defined if PSQI ⩾8 points. Clinical (i.e. age, gender, height, weight, and pre-existing comorbidities) and hospitalization (e.g. symptoms at hospital admission, hospital stay, and intensive care unit admission) data were collected from hospital medical records and used as adjusted covariables in the analysis.
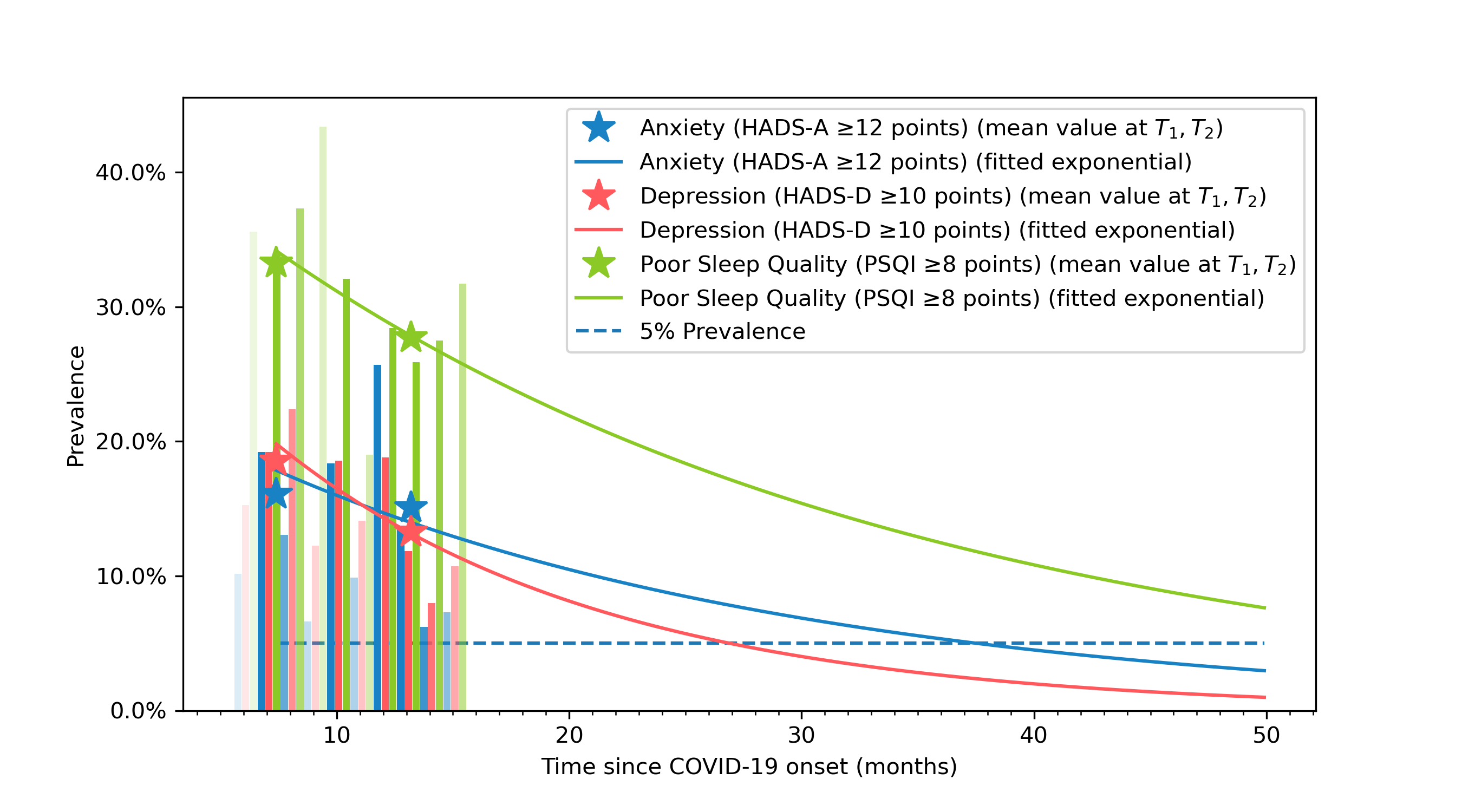
The exponential curves were fitted to the data according to the formula y = Ke ct, where y represents the modeled prevalence of the symptom (anxiety, depression, sleep quality) at a time t (in months), and K and c are the parameters of the model.
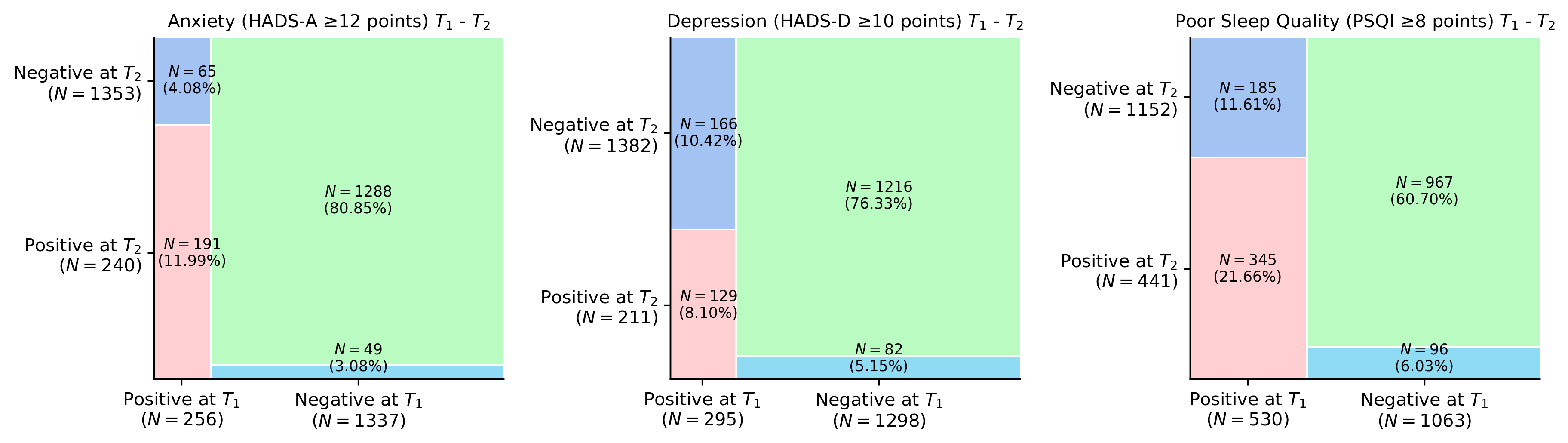
|From 2000 patients randomly selected, 1593 (80.9%) were assessed at T1 (mean: 8.4, range 6–10) and T2 (mean: 13.2, range 11–15) months after hospital discharge. Mosaic plots revealed that the prevalence of anxiety symptoms slightly decreased from 16% at T1 to 15.1% at T2, whereas the prevalence of depressive symptoms decreased from 18% at T1 to 13.2% at T2 (online Supplementary Fig. S1). A similar trend was observed for poor sleep quality with a decrease from 33.2% at T1 to 27.7% at T2. The mosaic plots revealed that a small number of patients developed anxiety (n = 49, 3%) or depressive (n = 82, 5.1%) symptoms or poor sleep quality (n = 96, 6%) between T1 and T2 (online Supplementary Fig. S1). The fitted exponential curves visualized a decreased prevalence trend for anxiety/depressive levels and poor sleep quality (online Supplementary Fig. 2).
To the best of our knowledge, this is the first analysis showing the trajectory curve of recovery of post-COVID anxiety/depressive symptoms and sleep quality in previously hospitalized COVID-19 survivors. Although the prevalence of post-COVID anxiety and depressive symptoms was considerable, a potential recovery the following months was observed, explaining the downward prevalence trend. A decreasing trend in the presence of anxiety/depressive symptoms agree with previous studies on heart surgery showing that these symptoms improve the first year after heart surgery (Rosson et al., Reference Rosson, Monaco, Miola, Cascino, Stubbs, Correll and Solmi2021). However, the decreased trajectory curves observed in COVID-19 survivors were not as pronounced as expected suggesting that anxiety/depressive symptoms and poor sleep quality could be long-lasting post-COVID sequelae. This may be related to the fact that some COVID-19 survivors not experiencing these symptoms at the first assessment presented them at the second and longer follow-ups, supporting the hypothesis of delayed-onset symptoms (Fernández-de-las-Peñas et al., Reference Fernández-de-las-Peñas, Florencio, Gómez-Mayordomo, Cuadrado, Palacios-Ceña and Raveendran2021). In fact, a recovery trajectory for anxiety/depressive symptoms would agree with the results observed by Saunders et al. (Reference Saunders, Buckman, Fonagy and Fancourt2021) for the general population, but would disagree with those reported by Gambin et al. (Reference Gambin, Oleksy, Sękowski, Wnuk, Woźniak-Prus, Kmita and Bonanno2021). It is highly important to consider that population samples and surrounding factors of these studies were different. Furthermore, the recovery trajectory of poor sleep quality was slower than that of anxiety/depressive symptoms, suggesting that poor sleep quality will be present longer than 5 years after infection and will require further attention and treatment.
Although this is the first-time investigating the trajectory recovery curves of post-COVID anxiety/depressive symptoms and sleep quality functional status with a large and multicenter design, potential weaknesses should be recognized. First, only hospitalized individuals aged 60-years old were included. Second, we did not collect the presence of anxiety/depressive symptoms and sleep quality at hospital admission. Finally, anxiety and depressive symptoms could also be affected by external surrounding factors (e.g. relative affection by COVID-19, isolation, and social pressure) which were not assessed in this study. In fact, the presence of post-traumatic stress disorder in our sample could be associated with the identified trajectory curves.
In conclusion, a trajectory curve analysis revealed that post-COVID anxiety/depressive symptoms and poor sleep quality tend to slowly recover during the following 5 years after SARS-CoV-2 infection in previously hospitalized COVID-19 survivors.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S003329172200006X.
Author contributions
All authors contributed to the study concept and design. CFdlP, JMG, and OPV conducted literature review and conducted the statistical analysis. All authors recruited participants and collected data. OPV supervised the study. All authors contributed to interpretation of data. All authors contributed to drafting the paper. All authors revised the text for intellectual content and have read and approved the final version of the manuscript.
Financial support
The LONG-COVID-EXP-CM is supported by a grant associated with the Fondo Europeo De Desarrollo Regional – Recursos REACT-UE del Programa Operativo de Madrid 2014–2020, en la línea de actuación de proyectos de I + D + i en materia de respuesta a COVID 19. The sponsor had no role in the design, collection, management, analysis, or interpretation of the data, draft, review, or approval of the manuscript or its content. The authors were responsible for the decision to submit the manuscript for publication, and the sponsor did not participate in this decision.
Conflict of interest
No conflict of interest is declared by any of the authors.
Consent to participate
Participants provided informed consent before collecting data.
Consent for publication
No personal info of any patient is provided in the text.