
Abstract
Background
Harvard Pilgrim Health Care expanded coverage for non-invasive prenatal testing (NIPT) to include all pregnant, single-gestation women aged < 35 years, through a performance-based risk-sharing (PBRS) agreement with Illumina to offset costs from coverage expansion. NIPT analyzes cell-free DNA fragments from a maternal blood sample to screen for fetal aneuploidies and is considered a more accurate screening method than conventional serum biochemical screening and nuchal translucency ultrasound-based approaches.
Objective
This study assessed the impact of NIPT coverage expansion on prenatal screening strategies and payer expenditures.
Methods
This was a real-world comparison of utilization and expenditures of prenatal screening and diagnostic testing in pregnant women aged < 35 years pre- (1 March 2016–28 February 2018) and post- (1 March 2018–30 September 2019) coverage expansion. Incidence rate ratios (IRRs) with 95% confidence intervals (CIs) were estimated to compare changes in utilization of conventional and NIPT-based prenatal screening methods. Change in per member per month (PMPM) expenditures in $US year 2020 were assessed post-coverage expansion using a budget impact model.
Results
A total of 5041 and 4109 distinct pregnancies were identified in pre- and post-coverage expansion periods, respectively. Mean ± standard deviation maternal age was consistent between pre- and post-coverage expansion periods (30.35 ± 3.35 and 30.33 ± 3.28, respectively). Screening orders for conventional methods decreased, with an adjusted IRR in the post-expansion period of 0.87 (95% CI 0.85–0.90) times the rate in the pre-expansion period; orders for NIPT increased, with an adjusted IRR in the post-expansion period of 1.41 (95% CI 1.32–1.51) times the rate in the pre-expansion period. Invasive diagnostic testing was low at baseline (1.0%) and did not change post-coverage expansion. The change in PMPM is estimated at $US0.026 post-coverage expansion.
Conclusion
The PBRS agreement to expand NIPT coverage for women aged < 35 years was associated with an increase in NIPT utilization, decreases in conventional screening methods, and a modest increase in PMPM expenditures.
Similar content being viewed by others


Given the 2020 update of clinical guideline recommendations, payers may be considering the budget impact of expanding coverage of non-invasive prenatal testing (NIPT) to women aged < 35 years. |
The change in resource utilization for conventional screening methods and NIPT is important to quantify as other insurers consider expanding coverage for NIPT to low-/average-risk women. |
Our findings from a performance-based risk-sharing agreement that expanded NIPT coverage for women aged <35 years was associated with statistically significant increases in NIPT utilization, decreases in the use of conventional prenatal screening methods, and an overall modest increase in the budget for prenatal screening. |
1 Introduction
To address uncertainty about clinical and economic outcomes from coverage expansion of new therapies and technologies, payers and manufacturers are increasingly turning to performance-based risk-sharing (PBRS) agreements. PBRS agreements may address problems with the release of innovative technologies such as delayed market access due to limited evidence from a payer perspective [1] or providing medical products to subpopulations with patient heterogeneity and uncertain effectiveness [2]. Remedying such limitations by conditioning coverage or level of reimbursement explicitly before the collection of data may allow a more favorable distribution of risk between the manufacturer and payer [1]. Private sector stakeholders have expressed interest in PBRS, especially with real-world financial utilization estimates as an outcomes guarantee measure [3]. However, there is a paucity of historical examples of PBRS in the USA, especially for contracts dealing with diagnostics, with only 12 reported cases from 1997 to 2016 [4].
Through a collaboration with Harvard Pilgrim Health Care (HPHC) and Illumina, we report the results of a PBRS agreement on coverage expansion for non-invasive prenatal testing (NIPT) using real-world evidence from HPHC claims data. Cell-free DNA (cfDNA)-based NIPT analyzes cfDNA fragments from a maternal blood sample to screen for fetal aneuploidies, including trisomies 21, 18, and 13 (T21/18/13). A meta-analysis of 35 studies including > 200,000 pregnancies reported that NIPT in singleton pregnancies detected > 99% of fetuses with T21, 98% with T18, and 99% with T13 at a combined false-positive rate (FPR) of 0.13% [5]. NIPT is considered a more accurate method of T21/18/13 screening than conventional serum biochemical screening and nuchal translucency (NT) ultrasound-based approaches, as conventional approaches have lower sensitivity (e.g., 82–87% for first trimester screening and 81% for quadruple screen), higher FPRs (~ 5%), and lower positive predictive values (< 5%) [6,7,8]. Thus, NIPT provides clinical utility through a higher detection rate and a decrease in unnecessary confirmatory invasive procedures, such as amniocentesis and chorionic villus sampling (CVS), which carry a risk of complications and miscarriage as well as additional costs and resources associated with pre-test counseling, the procedure, and treatment of complications [9]. As of 2020, clinical practice guidelines formally recommend that all pregnant women be offered prenatal screening, including NIPT as an option, regardless of maternal age or risk status [8, 10, 11].
Historically, payer coverage policies have differed on whether utilization and insurance coverage of NIPT should be restricted to high-risk populations (e.g., maternal age ≥ 35 years or a positive conventional serum screen) versus the general obstetric population that would include low-/average-risk patients (e.g., aged < 35 years without other risk factors) [6, 10, 11]. Many of the early clinical studies reporting the performance and clinical utility of NIPT focused on high-risk populations, leading to questions regarding the generalizability of the data and the clinical utility in lower-risk populations. Payers and policymakers also highlighted the need for real-world evidence of how NIPT is integrated into practice in lower-risk populations—citing concerns regarding concurrent use of conventional testing and NIPT or NIPT use in patients with low-risk conventional test results. A growing number of studies—including a national implementation project—have evaluated the performance of NIPT as a primary screening test specifically in low-risk or general obstetric (all-risk) populations [7, 12,13,14,15], with NIPT shown to be a more sensitive and specific screening test (with higher positive predictive values) for fetal aneuploidies than conventional screening approaches.
To address the call for real-world evidence in the population of women aged < 35 years and assess the economic implications, Illumina, a developer and manufacturer of next-generation sequencing technology that is used in many NIPT assays, and HPHC, a health insurance plan that provides coverage to approximately 1.2 million people in the northeast of the USA, entered into a PBRS agreement that expanded coverage for NIPT to include all pregnant, single-gestation women aged < 35 years on the estimated delivery date [16]. HPHC’s previous cfDNA NIPT coverage policy listed advanced maternal age (i.e., ≥ 35 years) or other high-risk features (including high-risk conventional screening results) as coverage criteria. The objective of this study was to assess the impact of this real-world PBRS on prenatal screening practice patterns and payer expenditures in a lower-risk (age < 35 years) pregnancy population.
2 Methods
On 1 March 2018, Illumina and HPHC entered into a PBRS agreement with the goal of providing coverage of NIPT, regardless of manufacturer (i.e., based on clinician preference; not specific to Illumina), as a primary method of screening in pregnant women aged < 35 years. All pregnant, single-gestation women (including those aged < 35 years and without any other risk factors) enrolled in HPHC could access any NIPT. The outcomes of the agreement included (1) mitigating financial risk through a confidential agreement between HPHC and Illumina and (2) generating real-world evidence to assess the budget impact of coverage expansion. Other prenatal screening and diagnostic test policies remained the same. Providers were notified of the coverage change by HPHC in the same manner as all coverage changes are communicated, and no other interventions were conducted.
We utilized HPHC claims to identify a cohort of pregnant women with distinct pregnancies during the study time period. The subject population was limited to women aged < 35 years at the time of first prenatal screening or diagnostic test ordered using date of birth from the members’ claims (not adjusted for age at estimated delivery date). Inclusion criteria were (1) one or more pregnancy-related diagnostic or procedure code in HPHC claims during the pre-expansion period (first index date 1 March 2016; last index date 28 February 2018) or the post-expansion period (first index date 1 March 2018; last index date 30 September 2019) and (2) one or more order for prenatal screening or diagnostic testing (including any pregnancy confirmation codes). We also required women to have continuous enrollment in HPHC for 3 months before and 6 months after the pregnancy index date to decrease the chance of missing services related to the pregnancy. The durations of the pre- and post-expansion periods were approximately 24 and 19 months, respectively, taking continuous enrollment into account. Our analysis adjusted for differences in sample size between time periods. Women who had more than one pregnancy during the study time period were included. Distinct pregnancies were allocated in the pre-expansion cohort if their first prenatal screening order had a service date prior to 1 March 2018 and to the post-expansion cohort if their first prenatal screening order had a service date on or after 1 March 2018. International Classification of Diseases, Ninth Edition and Tenth Edition codes used to identify pregnancies; a complete list of current procedural terminology (CPT) codes used to identify test utilization can be found in the Appendix in the electronic supplementary material. Women who had CPT codes 84702 (human chorionic gonadotropin [hCG] quantitative) or 84703 (hCG qualitative) not in combination with other conventional screening, NIPT, or diagnostic orders were not included in the analytic sample, as these were deemed to be for pregnancy confirmation only. Given the nature of claims data, we did not have access to results of the screening tests and diagnostic procedures in our analytic sample. The study protocol was approved by the Colorado Multiple Institutional Review Board.
2.1 Utilization and Practice Patterns Analysis
To illustrate the change in utilization of screening strategies, we compared NIPT-based screening and conventional screening approaches based on clinically relevant categories initiated in the first versus second trimester. Conventional screening methods initiated during the first trimester included first trimester maternal serum screening (MSS)-based approaches—first trimester screening (FTS)/first trimester combined test (FCT), and integrated/sequential screening—and NT alone. The conventional screening method for the second trimester was quad screening. The final six clinically relevant groups categorized by screening strategy were (1) first trimester presentation with conventional MSS, (2) second trimester presentation with conventional MSS, (3) NT without MSS, (4) conventional MSS plus NIPT, (5) NIPT alone, and (6) NIPT plus NT. Among the cohort of distinct pregnancies, we also estimated the number of women who had subsequent orders for invasive diagnostic testing (amniocentesis or CVS).
Total patient orders, which included both paid and denied claims, were summarized for each screening and diagnostic testing category. We included both paid and denied claims for two reasons: (1) orders reflect demand from a patient perspective and remove the potential for external benefit management decisions outside of the provider and patient’s control and (2) to estimate a potential maximum budget impact scenario to inform payers on NIPT coverage expansion. We descriptively compared the change in conventional versus NIPT-based screening strategies using the relative percent change between the pre-expansion and post-expansion time periods, after adjusting for the number of distinct pregnancies. For example, more screening tests ordered in the post-expansion period may reflect more pregnant women choosing screening tests than in the pre-expansion period or more pregnancies that are eligible to be screened. Thus, we adjusted the pre-expansion period by a multiplier defined as the ratio of total distinct pregnancies in the post-expansion period divided by the total distinct pregnancies in the pre-expansion period to ensure equal comparison between time periods. In multivariable analyses, we used the entire sample pre- and post-coverage expansion to compare the change in conventional versus NIPT-based screening strategies using Poisson regression, adjusting for number of prior pregnancies and age. Adjusted incidence rate ratios (IRRs) with 95% confidence intervals (CIs) are reported.
2.2 Budget Impact Analysis
Using results from our screening utilization analysis, we developed a budget impact model to estimate changes in per member per month (PMPM) budget in $US year 2020 following coverage expansion of NIPT from the payer perspective. Following International Society for Pharmacoeconomics and Outcomes Research budget impact analysis (BIA) good practice principles, we used a simple cost-calculator approach [17]. The budget impact model assumed an annual time horizon to calculate the budget impact in total and PMPM. The original study spanned ~ 3.5 years but, to best account for time horizon relevant to the payer perspective, we present a 1-year budget impact estimate in line with standard payer budget planning practice. The study used data from a northeast regional health plan perspective (HPHC) with 900,000 covered lives (during the coverage expansion time frame) to inform other commercial payers on how costs of fetal aneuploidy screening and associated services changed with the introduction of NIPT for pregnant women aged < 35 years.
The BIA considered the rates of change of the screening utilization groups described in Sect. 2 (Table 1) and used 2020 Centers for Medicare and Medicaid Services (CMS) unit prices (Table 2) to estimate the PMPM budget impact post-coverage expansion [18]. The rationale for using alternative pricing for these tests is twofold: (1) HPHC has confidential contracts that do not allow public release of their prices and (2) establishment of the Protecting Access to Medicare Act of 2014 means that unit prices from CMS represent a weighted median of commercial payer rates in the USA from 2016 and are, therefore, applicable to a general US health plan population. To assess the sensitivity of the results to the variation of each parameter, we used a deterministic one-way sensitivity analysis. Moreover, findings from our BIA will be disseminated through an interactive tool, available upon request from the corresponding author, that will allow other health plans to tailor these analyses to their own populations and calculate their financial impact. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA), Stata version 16 (StataCorp, College Station, TX, USA), and Microsoft Excel 2016 (Redmond, WA, USA).
3 Results
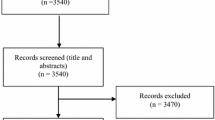
We identified 16,195 total distinct pregnancies with any prenatal screening orders (including pregnancy confirmations) from 1 March 2016 to 19 September 2019, with 9366 in the pre-coverage expansion period and 6829 in the post-coverage expansion period. After assigning continuous enrollment criteria, and removing pregnancy confirmation or single serum biochemical assay codes, the final analytic sample for the utilization analysis was 5041 distinct pregnancies in the pre-coverage expansion period and 4109 in the post-coverage expansion period (Fig. 1). The mean ± standard deviation and median age of pregnant women was 30.17 ± 3.39 and 31 in the pre-coverage period and 30.19 ± 3.32 and 31 in the post-expansion period. Across the two cohorts (pre- and post-expansion), a total of 1066 (11.65%) women had a prior pregnancy within the time period of the study.

Inclusion of study participants. MSS maternal serum screening, NIPT non-invasive prenatal testing, NT nuchal translucency
3.1 Utilization and Practice Patterns
The number of patients with screening tests ordered in each time period, the relative percent change, and IRRs are shown in Tables 1 and 3. The number of patients who received screening with conventional screening methods (e.g., serum biochemical markers or NT) decreased by 418 (from 3136 to 2718; − 13.0% change; adjusted IRR 0.87 [95% CI 0.85–0.90]), whereas the number of patients with orders for NIPT (without any serum markers) increased by 418 (from 973 to 1391; + 43% change; adjusted IRR 1.41 [95% CI 1.32–1.51]).
In the pre-coverage period, the largest proportion of patients (47.6%) had conventional MSS beginning in the first trimester (FTS, integrated, and sequential approaches), 10.8% had quad screening only, and 15.2% had NT alone. NIPT alone was observed in 14.3% of patients, 9.4% had NT and NIPT, and 2.7% had conventional MSS and NIPT. In the post-coverage period, decreases in conventional approaches were observed in all cohorts: − 307 orders (− 16%) for FTS/sequential/integrated, − 5 orders (− 0.7%) for NT alone, and -104 orders (− 23.4%) for quad screens. Conversely, claims for NIPT alone increased by 267 (+ 46%), those for NIPT + NT increased by 151 (+ 39%), and those for conventional MSS plus NIPT decreased by 2 (− 1.7%). We also observed a slight increase in claims for genetic counseling visits from the pre-coverage period to the post-coverage period (from 261 to 266; + 2%). After adjusting for prior pregnancies and age, the biggest increase in screening utilization was for NIPT alone, with a rate 1.44 (95% CI 1.32–1.59) times that in the pre-expansion period; the biggest decreases were for MSS-based approaches beginning in the first trimester (FTS, integrated, sequential), with a rate in the post-expansion period 0.86 (95% CI 0.82–0.90) times the rate in the pre-expansion period, and second trimester quad screening, with a rate in the post-expansion period 0.77 (95% CI 0.67–0.88) times that in the pre-expansion period.
We also assessed cases in which both conventional MSS tests and NIPT were ordered for the same patient. In the pre-coverage expansion period, only a small subset of patients (2.6%) had both conventional screening tests and NIPT. In this subset, the vast majority of NIPT tests (86%) were performed after the first conventional test, with a mean of 30.2 days (95% CI 23.9–36.4) between order dates. There were no changes in practice patterns following coverage expansion. A similar proportion of patients received conventional screening and NIPT (2.5%) in the post-expansion period, and 88% of NIPTs were performed after the first conventional test at a mean of 38.7 days (95% CI 31.7–45.8).
We observed a total of 41 invasive diagnostic tests (1.0% of screened pregnancies) in the pre-coverage period and 37 (0.88%)) in the post-coverage expansion period. There were 17 and 14 CVS orders in the pre-coverage expansion and post-coverage expansion periods, respectively, and 24 and 23 amniocentesis orders, respectively. Patients with orders for invasive testing decreased, with an adjusted IRR in the post-expansion period 0.97 (95% CI 0.63–1.49) times the rate in the pre-expansion period.
3.2 Budget Impact
Our BIA shows that expanded coverage for NIPT resulted in a modest increase in PMPM expenditures (Fig. 2). Total budget impact increased from a PMPM of $US0.138 to 0.164, for an incremental PMPM of $US0.026. Cost offsets included reductions in PMPM from FTS (− $US0.004), second trimester screening (− $US0.001), FTS plus NIPT (− $US0.002), and invasive diagnostic testing (− $US0.001). Cost increases included fully integrated screening ($US0.001), second trimester screening plus NIPT ($US0.002), NIPT alone ($US0.019), and NIPT plus NT ($US0.012). In one-way sensitivity analyses, each model parameter was varied using the lower and upper 95% CI of the IRRs from Table 1 to estimate the impact on the incremental PMPM. Varying the rate of change of NIPT alone was associated with a lower and upper incremental PMPM of $US0.021 and 0.033, respectively. Varying NT (without MSS) was associated with a lower and upper incremental PMPM of $US0.025 and 0.027, respectively. Varying second trimester screening ranged from a lower and upper incremental PMPM of $US0.025 and 0.026, respectively. Finally, because current average reimbursement rates may be lower than the NIPT price assumed in Table 2, we varied the lower bound of the NIPT price at $US395 [19] and found the incremental PMPM was reduced to $US0.01.

Incremental per member per month budget impact. A total of 8100 was assumed for annual number of distinct pregnancies. Number ordering prenatal screening was set as 4387. FTS first trimester screening, MSS maternal serum screening, NIPT non-invasive prenatal testing, NT nuchal translucency
4 Discussion
Our evaluation of the impact on utilization and costs of the change in coverage for NIPT screening among HPHC plan members is timely given the recent American College of Obstetricians and Gynecologists (ACOG) clinical guideline recommendation update that NIPT should be an option for all women regardless of age [8]. After HPHC expanded coverage for NIPT to all pregnant, single-gestation women aged < 35 years, orders for NIPT-based screening strategies increased (a relative increase of 43% and an absolute increase of 10%), whereas we observed a 13% decrease in the rate of conventional screening methodologies. We observed decreases in conventional screening approaches initiating in the first trimester (e.g., FTS, integrated, and sequential) and second trimester (e.g., quad screening). Expanding coverage did not result in an increase in concurrent testing (i.e., MSS in combination with NIPT). There were few invasive orders in patients in the baseline period, with no statistically significant change between pre- and post-coverage expansion time periods.
As noted, studies evaluating the performance of NIPT as a primary screening test specifically in low-risk or general obstetric (all-risk) populations [7, 12,13,14,15] have shown that NIPT is a more sensitive and specific screening test for fetal aneuploidies than conventional screening approaches. Research has shown that utilization of NIPT in women aged < 35 years has increased over time [20]. Our results add to this evidence base by providing real-world data on the impact of an expanded coverage policy by a US health plan on screening and diagnostic testing patterns. The change in resource utilization—for conventional screening methods and NIPT—is important to quantify as other insurers consider expanding coverage for NIPT to low-/average-risk women.
The results of this study help further characterize various aspects of the clinical utility of NIPT. First, removing the barrier of insurance coverage for women aged < 35 years resulted in increased utilization of NIPT, reflecting patient/physician preference for a more accurate screening method. Second, some policymakers have raised concerns that expanding coverage to women aged < 35 years without other risk factors may lead to NIPT being ordered in parallel with conventional screening tests or that clinicians may not have enough confidence in NIPT results to avoid ordering conventional tests. ACOG guidelines explicitly recommend against simultaneous testing with multiple screening methods, as this would be predicted to cause an increase in unnecessary invasive testing [8]. The results of our study do not support these concerns. Pregnant women with both conventional screening tests and NIPT were rare (2.6%) in the pre-expansion period, and in cases when both were ordered, NIPT was typically ordered ~ 4 weeks following the initial conventional screening tests, suggesting likely contingent use of NIPT in patients with high-risk conventional test results. Following initiation of the expanded coverage policy, there was no change in these observed trends. Third, we observed that, among pregnant women receiving conventional screening approaches that begin in the first trimester, 28% did not include NT. Clinical practice guidelines have highlighted that conventional screening approaches without NT are associated with lower detection rates (~ 69 to 88%) [6]; however, NT assessment requires access to a specially certified ultrasonographer. This may lead to equity of access issues because of distance or work requirements. Other events also may impact on access to NT. For example, the coronavirus 2019 (COVID-19) pandemic did not affect our study, but concerns regarding the number of in-person prenatal visits led several payers to open coverage for NIPT in low-/average-risk pregnancies [21]. Finally, another aspect of the clinical utility of NIPT is the potential to reduce invasive testing rates because its FPR is lower than that of conventional screening methodologies. Several real-world studies have evaluated the impact of NIPT on the use of invasive diagnostic tests in high-risk cohorts [22,23,24]. For example, in an analysis of NIPT uptake after its introduction among high-risk pregnant women (aged > 35 years) at a single, academic referral center, Larion et al. [25] reported that NIPT utilization increased and invasive diagnostic testing decreased in a short period of time. However, the change in invasive diagnostic testing was observed following NIPT utilization, increasing from 0% to approximately 48%. In our study, the absolute increase in NIPT utilization was only ~ 10% of pregnancies. In addition, NIPT use in patients with a high-risk MSS result was already a covered benefit with HPHC before the coverage expansion. Given the baseline utilization of NIPT in our sample, substantial changes in invasive testing rates were unlikely. However, a larger screening population and longer follow-up period would allow further characterization of the impact of increased NIPT utilization on invasive testing rates and the timing of invasive testing.
Given the recent clinical guideline recommendation update, other payers may also be considering the budget impact of expanding coverage of NIPT to women aged < 35 years. Prior economic assessments of the change in implementation of NIPT have estimated the savings threshold [26] or cost effectiveness of NIPT [27,28,29] or compared the total cost of pregnancy management and cost per trisomy detected for conventional screening and NIPT [30]. Although these studies provide evidence of the cost-saving potential of NIPT compared with conventional screening [29, 30], they are based on theoretical cohorts instead of real-world populations [26, 28,29,30]. Accordingly, results from economic models using a theoretical utilization rate of 70% [26, 29, 30] or a retrospective analysis of Medicaid-enrolled individuals [28,29,30] are not conducive to PBRS implementation from a commercial payer perspective, which is contingent upon monitoring of real-world clinical and economic endpoints. Our current real-world BIA provides payers with a case example of a PBRS to decrease uncertainty in reimbursing NIPT. The expansion in NIPT coverage resulted in a modest increase in PMPM expenditures (~ 2.6 cents). Given the limitations of our utilization analysis, we were unable to fully characterize the impact of increased NIPT utilization on invasive testing rates. Given the high cost of invasive procedures, an observed decrease in invasive diagnostic testing post-coverage expansion would likely result in overall cost savings.
The strengths of this study include the innovative nature of this project—which allowed us to evaluate the impact of an insurance coverage change associated with a PBRS agreement in the real-world setting. These findings can be utilized by both HPHC and other payers to project the real-world impact of NIPT coverage in women aged < 35 years. The study also provides a large population-based evaluation of practice patterns for prenatal screening, with the results highlighting opportunities for improving quality of care. There are also important limitations to consider. First, the HPHC claims data are not linked with electronic health records (EHRs), so we could not identify the result of each screening/diagnostic test and categorize patients by subsequent healthcare utilization following specific test findings. In addition, with no link to EHR data, we were unable to control for other confounding variables. Second, our analysis of invasive testing rates was not comprehensive because we restricted our cohort to only those ordered after prenatal screening tests. Given these limitations, we are only able to conclude associations between coverage expansion and outcomes. Nonetheless, the results of this study help elucidate the clinical utility of NIPT in women aged < 35 years using a large, population-based cohort. Third, we included all claims regardless of whether they were paid or denied to isolate the increase in utilization requested from patients. While this analysis excludes reimbursement decisions, it also provides a conservative budget impact estimate by assuming all claims were reimbursed at 100%. Fourth, we were unable to use HPHC-specific prices in our budget impact model. However, the CMS unit prices used are representative of commercial payer rates in the USA. The publicly available budget impact cost calculator, also available from the corresponding author, can be used to include prices at current reimbursement rates for individual payers to modify our analyses to their own plan populations. Finally, given there was already NIPT utilization at baseline in HPHC, it was difficult to isolate the impact of coverage change on invasive diagnostic strategies.
5 Conclusion
The PBRS agreement to expand NIPT coverage for women aged < 35 years was associated with a modest overall increase in women receiving prenatal screening and statistically significant increases in NIPT utilization and decreases in the use of conventional screening methods. We did not observe an increase in concurrent use (e.g., parallel orders) following coverage change. Few invasive diagnostic tests were ordered in the baseline period, with no statistically significant change between the pre-coverage expansion and post-coverage expansion time periods. In terms of the economic impact, there was a modest increase in PMPM expenditures. HPHC has decided to maintain coverage of NIPT for pregnant women aged < 35 years.
References
Garrison LP, et al. Performance-based risk-sharing arrangements—good practices for design, implementation, and evaluation: report of the ISPOR good practices for performance-based risk-sharing arrangements task force. Value Health. 2013;16(5):703–19.
Carlson JJ, et al. Linking payment to health outcomes: a taxonomy and examination of performance-based reimbursement schemes between healthcare payers and manufacturers. Health Policy. 2010;96(3):179–90.
Garrison LP, et al. Private sector risk-sharing agreements in the United States: trends, barriers, and prospects. Am J Manag Care. 2015;21(9):632–40.
Carlson JJ, Chen S, Garrison LP. Performance-based risk-sharing arrangements: an updated international review. Pharmacoeconomics. 2017;35(10):1063–72.
Gil MM, et al. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet Gynecol. 2017;50(3):302–14.
Committee on Practice Bulletins—Obstetrics, C.o.G., and the Society for Maternal-Fetal Medicine, Practice Bulletin No. 163: Screening for Fetal Aneuploidy. Obstet Gynecol. 2016; 127(5): e123–37.
Norton ME, et al. Cell-free DNA analysis for noninvasive examination of trisomy. N Engl J Med. 2015;372(17):1589–97.
Committee on Practice Bulletins—Obstetrics, C.o.G., and the society for maternal-fetal medicine, number 226. Screening for Fetal Chromosomal Abnormalities. Obstet Gynecol. 2020;136(4): e48–69.
Sequencing-based tests to determine fetal down syndrome (trisomy 21) from maternal plasma DNA. Technol Eval Cent Assess Program Exec Summ. 2013;27(10):1–6.
Benn P, et al. Position statement from the Chromosome Abnormality Screening Committee on behalf of the Board of the International Society for Prenatal Diagnosis. Prenat Diagn. 2015;35(8):725–34.
Gregg AR, et al. Noninvasive prenatal screening for fetal aneuploidy, 2016 update: a position statement of the American College of Medical Genetics and Genomics. Genet Med. 2016;18(10):1056–65.
Zhang H, et al. Non-invasive prenatal testing for trisomies 21, 18 and 13: clinical experience from 146,958 pregnancies. Ultrasound Obstet Gynecol. 2015;45(5):530–8.
Song Y, et al. Noninvasive prenatal testing of fetal aneuploidies by massively parallel sequencing in a prospective Chinese population. Prenat Diagn. 2013;33(7):700–6.
Pergament E, et al. Single-nucleotide polymorphism-based noninvasive prenatal screening in a high-risk and low-risk cohort. Obstet Gynecol. 2014;124(2 Pt 1):210–8.
van der Meij KRM, et al. TRIDENT-2: national implementation of genome-wide non-invasive prenatal testing as a first-tier screening test in the Netherlands. Am J Hum Genet. 2019;105(6):1091–101.
Illumina. verifi prenatal test. 2017 [cited 2017]; https://www.illumina.com/content/dam/illumina-marketing/documents/applications/reproductive-health/22337_LB_0016_G_Patient_Brochure.pdf.
Sullivan SD, et al. Budget impact analysis—principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health. 2014;17(1):5–14.
Centers for Medicare and Medicaid Services. Clinical Laboratory and Physician Fee Schedules. 2020 [cited 2020 May 20]; https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/FeeScheduleGenInfo/.
Incorporated, Q.D., QNatal Advanced: Give your patients the confidence of knowing. 2016.
Chen KM, et al. Maternal age trends support uptake of non-invasive prenatal testing (NIPT) in the low-risk population. J Matern Fetal Neonatal Med. 2019;32(23):4039–42.
aetna Serum and urine marker screening for fetal aneuploidy. Policy No. 0464, 2020.
Wallerstein R, Jelks A, Garabedian MJ. A new model for providing cell-free DNA and risk assessment for chromosome abnormalities in a public hospital setting. J Preg. 2014;2014:962720.
Warsof SL, Larion S, Abuhamad AZ. Overview of the impact of noninvasive prenatal testing on diagnostic procedures. Prenat Diagn. 2015;35(10):972–9.
Wax JR, et al. Noninvasive prenatal testing: impact on genetic counseling, invasive prenatal diagnosis, and trisomy 21 detection. J Clin Ultrasound. 2015;43(1):1–6.
Larion S, et al. Uptake of noninvasive prenatal testing at a large academic referral center. Am J Obstet Gynecol, 2014;211(6):651 e1–7.
Benn P, et al. An economic analysis of cell-free DNA non-invasive prenatal testing in the US General Pregnancy Population. PLoS ONE. 2015;10(7):e0132313–e0132313.
Hopkins MK, et al. Cell-free DNA for Down syndrome screening in obese women: is it a cost-effective strategy? Prenat Diagn. 2020;40(2):173–8.
Avram CM, et al. Cell-free fetal DNA screening for detection of microdeletion syndromes: a cost-effectiveness analysis. J Maternal Fetal Neonatal Med. 2019;1–9.
Fairbrother G, et al. Prenatal screening for fetal aneuploidies with cell-free DNA in the general pregnancy population: a cost-effectiveness analysis. J Maternal Fetal Neonatal Med. 2016;29(7):1160–4.
Song K, Musci TJ, Caughey AB. Clinical utility and cost of non-invasive prenatal testing with cfDNA analysis in high-risk women based on a US population. J Maternal Fetal Neonatal Med. 2013;26(12):1180–5.
Fairbrother G, et al. Prenatal screening for fetal aneuploidies with cell-free DNA in the general pregnancy population: a cost-effectiveness analysis. J Matern Fetal Neonatal Med. 2016;29(7):1160–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
We received institutional funding to the University of Colorado from Real Endpoints and Illumina to conduct this study. HPHC provided the data directly to University of Colorado researchers through a data use agreement. Only authors from the University of Colorado had access to the raw data to generate the aggregate findings shown in this manuscript. University of Colorado authors led the study design, data analysis, interpretation of data, and writing of the report with feedback provided by BS and JFB. All authors discussed where to submit the article for publication.
Conflicts of interest
BS is an employee of Illumina and JFB is an employee of Real Endpoints. MSS is an employee of HPHC. TAGQ, HDA, GW, SK, and RBM have no conflicts of interest that are directly relevant to the content of this article.
Availability of data and material
Due to the confidentiality requirements of HPHC and its enrollees, data used for this study are not available to the public.
Code availability
A user-friendly budget impact cost calculator will be publicly available for other health plans to tailor our analyses to their own plan populations. Please contact the corresponding author to request access to this tool.
Ethics approval
The study protocol was approved by the Colorado Multiple Institutional Review Board.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
All authors were part of the conceptualization of the design and analysis of the study. RBM and TAGQ carried out analyses. RBM, BS, TAGQ, and SK drafted the manuscript. GW prepared the data for analysis. All the authors critically reviewed the manuscript for intellectual content.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Quinlan, T.A.G., Schroeder, B., Kwon, S. et al. Economic Impact of Coverage Expansion for Non-invasive Prenatal Testing Through a Performance-Based Risk-Sharing Agreement. PharmacoEconomics Open 5, 449–458 (2021). https://doi.org/10.1007/s41669-021-00261-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41669-021-00261-y