
Summary
The seasonality of influenza continues to attract many studies, yet there is likely to be no definitive explanation that covers all regions, climates and populations, at all times. The influenza seasonality in each area is most likely the result of a number of factors contributing to different degrees to the observed incidence and timing of influenza infections. However, despite the massive growth in the human population and its global mobility over the last 40–50 years, it is remarkable how the patterns of seasonal influenza incidence have remained relatively unchanged in temperate, subtropical and tropical regions, alike. This suggests that there may well be some sort of underlying, characteristic, intrinsic host-pathogen-environmental oscillation in each of these regions that is relatively unperturbed by human activities and behaviour. This review critically highlights some of these factors in the light of more recent, modern studies and suggests some additional experimental studies that may help to elucidate further and provide some additional supporting evidence for some of the postulated mechanisms underlying the seasonality of influenza.
Similar content being viewed by others

Introduction
It is likely that there has been some pattern of influenza seasonality in the human population through the ages, but it is only the identification and naming of the virus in the early twentieth century that has allowed us to try to define this more clearly in global, rapidly expanding populations with modern methods.
The seasonality of any pathogen requires several basic elements to be in place: a susceptible population in which the pathogen can replicate and propagate, an accurate, sensitive and specific diagnostic test to detect its presence, and a reliable, robust reporting system and database to record the results to allow seasonality patterns and trends to be determined and analysed. Although there have been several reviews on the seasonality of influenza, none have addressed these issues in much detail.
Potential biases in available data for analysis
If laboratory testing is not performed, then the pathogen cannot be detected. Due to resource limitations or a desire to optimise resource usage in other directions, some diagnostic laboratories may decide to stop routine testing for influenza during the spring and summer months in temperate regions. In some areas of the world where vector-borne infections become a higher risk and a more serious public health concern during the warmer months (e.g. West Nile virus testing in Canada), such a resource reallocation would not be unreasonable [1]. The cessation of routine testing may give the impression that influenza disappears entirely during these warmer months in some regions, when in fact, the testing is just not being done.
The type of testing matters. Some laboratories may still rely on older types of diagnostic methods, such as viral culture or immunofluorescence testing, rather than more modern sensitive molecular methods, such as multiplex PCR, where multiple respiratory pathogens can be detected within one sample, simultaneously. The older diagnostic techniques are more labour-intensive, slower, and less sensitive than these modern, semi- (or entirely) automated multiplex PCR assays [2–4]. Yet, as they are cheaper run, require less expensive equipment and do not require specific workflow and laboratory space organisation, they are still common in some parts of the world. So comparing data obtained from a region where viral culture is used may give the impression that there is less influenza in that population than in another population of similar size and influenza incidence, where molecular testing methods are the norm.
The most obvious patterns of influenza seasonality are well known: distinct and large peaks of influenza incidence in northern and southern temperate countries versus smaller and lesser well-defined peaks in subtropical and tropical countries. This seems to be the case globally, whatever variation there might be in the local clinical sampling and testing protocols. Most of this data comes from patients who are either hospitalised or are seen in a hospital setting (including the emergency department), who, even if not admitted, are still considered ill enough to be sampled and tested. Yet, these sources of data also come with their own biases.
Apart from a few examples, there are relatively few studies that have randomly been sampled from the general population throughout the year to see if influenza is continuously circulating within any given population [5••]. Outside of a research study, from a clinical and diagnostic cost-effectiveness viewpoint, this makes sense in temperate regions, since previous records have shown little or no circulating influenza between the autumn and winter months. Inter-seasonal influenza viruses arriving into such populations are therefore most likely to have been imported from elsewhere (e.g. the tropics). This (tropical) source-(temperate) sink hypothesis has been postulated by some researchers [6, 7], but it has not been easy to demonstrate, and may not apply in every influenza season [8]. A recent study from Australia suggests that there is inter-seasonal influenza persistence and transmission across a variety of climates and populations [5••]. However, further studies elsewhere are needed to determine if these findings apply in other populations and climates. Given the limited duration of such studies, the pattern of influenza introduction and transmission may vary in different ways from year to year.
To some extent, there will be a sampling bias in any population simply because of the variation in health-seeking behaviours, which may be affected by cultural and economic factors. An example of likely cultural bias can be found in Southeast Asian populations, where it is more common to seek out healthcare services for relatively mild seasonal coughs and colds, compared to Western cultures where stoicism for such ailments is more common. This difference in behaviour can be explained by a difference in the perceived vulnerability to disease between cultures [9]. This was particularly evident during the 2009 influenza A/H1N1 pandemic, where Eastern populations were much more compliant and attentive to government advice about limiting virus transmission during this period [10, 11].
A potential economic bias may be seen where healthcare is available in both the public (government-funded) and private (where the patient pays) sectors. In some studies from middle-income countries in Central America, it was found that the private sector is consulted first if the illness is considered to be urgent, particularly in young children or the elderly, as the physicians are thought to be better trained and there is little or no delay in being seen [12, 13]. For less urgent illness in older children or younger adults, government clinics are usually visited [14], though there is also a tendency for more wealthy families to use private health services [15]. Elsewhere, in lower- and middle-income countries, medical costs are a significant proportion of daily household income, and clearly influence families’ decisions to seek medical attention for various ailments [16, 17]. Such choices may skew influenza surveillance data, and potentially underestimate the burden of mild disease, and/or overestimate the burden of severe disease from hospital or tertiary referral centres (to whom the smaller, private clinics may refer severely ill cases), particularly if the data from private clinics is not made available. However, these differences may have more impact on the relative size of the incidence peaks, and less on their timing, as long as some testing is performed throughout the year.
Acknowledging this variety of diagnostic methods that are used to obtain this viral incidence data from different regions, and accepting that teams can only analyse the data they have, we can now examine what the current data has been telling us.
Drivers of influenza seasonality: indoor versus outdoor, temperate versus tropical factors?
Many factors have been postulated as underlying drivers of influenza seasonality in human populations. There may be an intrinsic host-pathogen-environment cycle, which has existed since the evolution of the pathogen and its host. This is complicated for influenza, as the natural reservoir for influenza viruses is in birds (specifically, waterfowl) [18]. However, if we confine this discussion to the behaviour of established human influenza viruses, other viral and host-related factors can be identified and assessed as to how they might contribute to influenza seasonality.
Moorthy et al. [19] defined seasonality as “a temporal pattern of systematic periodic oscillation within a predetermined cycle that can be characterized by peak timing, amplitude, and duration.” The most obvious example of this is the annual seasonal influenza peaks in the northern and southern temperate regions—a pattern that disappears in the tropics. So whatever is driving this seasonal cycle of influenza infection in these temperate regions, these factors must change significantly in tropical zones. The most obvious change is the climate.
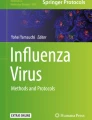
Various aspects of these meteorological changes (relative and absolute humidity, temperature, rainfall, sunshine hours and even wind speed) have been correlated with local influenza incidence by teams from around the world (Table 1, Figs. 1 and 2). However, these studies are generally conducted over a fixed period of several years, so it is possible that any reported correlations could be different in subsequent or earlier years. The overall picture that has emerged for influenza (which is a lipid-enveloped virus and therefore more prone to inactivation in warm, humid conditions) is that in temperate regions, its incidence peaks in the colder, drier months of the year (i.e. autumn and winter), whereas in tropical regions, its incidence peaks in the wetter, rainy months [38••]. These correlations are based on influenza incidence data from human patient populations during routine clinical encounters, rather than in in vitro or animal experiments in laboratory settings. The latter point is important because the seasonality of influenza in human populations in both temperate and tropical climates is likely to be closely linked to human behavioural and environmental factors.

World map showing the location (indicated by their latitude/longitude) of the studies listed in Table 1, summarising the correlation with influenza A incidence. Up arrow positive correlation, down arrow negative correlation, horizontal double-headed arrow no significance correlation either way, mixed arrows separated by a slash a mixed correlation found among different studies for the particular geographical location. T temperature; RH relative humidity; SP H specific humidity; OR odds ratio.

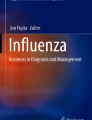
World map showing the location (indicated by their latitude/longitude) of the studies listed in Table 1, summarising the correlation with influenza B incidence. Up arrow positive correlation, down arrow negative correlation, horizontal double-headed arrow no significance correlation either way, mixed arrows separated by a slash a mixed correlation found among different studies for the particular geographical location. T temperature, RH relative humidity, SP H specific humidity, OR odds ratio.
One well-designed study examining this interaction between influenza seasonality, climate and human behaviour from a tropical population in Bangladesh suggested that the positive correlation between the peak of influenza incidence with rainfall was due to the heavy rain driving people indoors, where they are closer together so that viral transmission occurs more frequently [39••]. There may also be a contribution from the potentially longer survival of influenza in surface water droplets [40], which are more prevalent in conditions of high humidity and rainfall. This correlation appeared to work well for up to five people per room in the household. However, the authors found that when the number of people in the household reached five or more per room, the correlation broke down. One suggested reason for this was that households with more children would have older children who were partially or completely immune to infection from previous exposure to influenza viruses. Yet, the authors appeared to not have recorded the age of the individuals in the household that they examined, nor to have taken any blood from them to assess the presence of any cross-reacting protective immunity to other influenza viruses to which they had been previously exposed. Whilst these additional steps would probably have required additional ethical approval, and more funding, these would have been achievable—if the authors had been able to predict these possible outcomes of their initial analysis. Thus, a further study covering these points would be very useful.
Another series of studies that lacked an additional environmental element that would have been very helpful to try to resolve these questions of influenza seasonality are the household influenza transmission studies by Cowling and colleagues. Cowling and colleagues conducted a series of household transmission studies in subtropical Hong Kong, where the population density is one of the highest in the world. Perhaps not unsurprisingly, they did find evidence of household transmission. They also assessed the effectiveness of various interventions to reduce such transmission [41, 42, 43•, 44]. Whilst these studies are valuable in assessing the degree to which members within a household can potentially transmit the virus between one another, there was no environmental measurement and correlation component to the analysis. Also, in terms of extrapolating the findings of the potential for influenza transmission between individuals to the community in general, the results from household studies are not very generalizable. The household environment is very specific in that it entails close contact for long duration between individuals who know each other intimately. Therefore, it would be valuable to repeat such intensive sampling-epidemiological modelling studies in the workplace and leisure/shopping amenities, where transmission is mostly between colleagues and/or strangers, where contact is more casual and less intimate, to assess how intense such transmission events are in these environments.
Finally, there are many studies examining the correlation between influenza incidence and outdoor meteorological conditions. This is probably because this outdoor climate data is collected systematically and routinely in most countries, and is often freely available from local weather websites. In contrast, there are very few studies examining the variety of indoor climates and influenza incidence, e.g. what is the average indoor temperature, and relative or absolute humidity throughout the year in houses in temperate, subtropical and tropical countries? Is there a diurnal variation to this? Particularly with people mostly working outside the house during the day and sleeping in the house at night? What different methods of indoor heating do people use (water or oil-based, gas-based, electric, wood-burning systems, etc.)? This will affect the indoor climate in which influenza transmission may occur.
Some older studies have linked changes in indoor heating methods to cardiovascular mortality [45]. It is known that influenza infection can exacerbate these conditions, so it makes sense that during the influenza season, any indoor environment that favours prolonged influenza survival may contribute to such mortality. One Japanese study found that more severe influenza infections were decreased in children living in homes heated by kerosene or gas heaters. These heating methods produce water as a combustion by-product, thus increasing the indoor ambient humidity [46], which is detrimental to influenza survival. More recent studies have modelled the impact of altering temperature and humidity on the airborne survival of influenza and have recommended indoor humidification as a potential intervention to reduce the infection rate [47, 48]. Multiple studies have detected airborne viruses in the indoor environment, usually citing the ‘potential’ for, though not actually demonstrating an actual, subsequent increase in the incidence of new influenza infections arising as a direct consequence of these airborne viruses, in that same environment [49–51, 52••].
Other potential drivers and/or contributions to influenza seasonality
It is worth recapping on some of the oft-discussed factors that are thought to contribute to influenza seasonality. These are all interconnected and it is likely that the seasonality of influenza in any particular population will depend on a variable contribution from any of these factors, e.g. whether or not seasonal influenza epidemics are triggered by either an imported virus or the persistence of the previous season’s virus, or a combination of both, is still unclear [5 ••]. However, once that season’s virus enters that population, how it spreads in that population will depend on the variety and combination of indoor versus outdoor climate factors, and their impact on both virus survival and host (human) behaviour and immunity.
Intrinsic oscillations
Intrinsic oscillations of influenza circulation and infection may exist at a fundamental host-pathogen-environment level that are independent of his behaviour and daily activities [19, 38••, 53–55]. However, although these oscillations may well exist, the intrinsic oscillation cycles may be very difficult to separate out from ‘extrinsic’ factors such as those associated with the diversity of modern interconnected human behaviour in different cultures and climates. Some of these human activities have their own cycles, superimposed on this intrinsic cycle, e.g. the cycles of school terms, and the mass human movements associated with the school holidays.
It is remarkable that these seasonality patterns in temperate and tropical regions have remained so distinctive and robust over the past 50 years, a period which spans most of these influenza-climate correlation studies (Table 1, Figs. 1 and 2). This is despite the massive increase in the human population [56], travel and connectivity (including the impact of the Internet). Hence, the continued assertion by some authors that there must be some sort of fundamental, underlying intrinsic oscillation of the influenza virus-human-environment cycle seems plausible—but how can we reveal this more clearly?.
Teasing out the various contributing factors that sustain this intrinsic cycle is difficult, but maybe easier in more isolated, rural communities, which are less internationally connected. One potential site for such a study may be found in rural China. With the relaxation of the one-child policy in China, there is an opportunity to see how the increase in the number of newborns (and therefore susceptible hosts) into each family impacts on the existing seasonal influenza cycle in these communities. It has been suggested already that this change in policy may potentially impact on the epidemiology of other viruses, such as cytomegalovirus [57]. Will the incidence peaks just become higher? Or might there be a phase shift in the timing of the peaks as well? There would have to be reasonably detailed medical records of confirmed influenza infections before and after the lifting of this policy in such rural communities to be able to discern any differences. With the recent increase in comprehensive surveillance for human and animal (swine and avian) influenza infections in China, there are likely to be some communities with good surveillance records that could conduct this sort of study [58–61].
Factors affecting influenza virus survival
Factors affecting influenza virus survival (viability) and therefore transmission in an outdoor setting include temperature, relative or absolute humidity, rainfall, sunlight hours and/or combinations of these parameters [39••, 62–64]. Although there have been many studies investigating these factors, not all of them agree, which could be due to a difference in human behaviour patterns, which themselves differ between seasons, cultures and countries—all interacting in different ways, which just adds to the confusion [38••]. Again, a good example of this are the well-defined annual peaks of influenza incidence in the autumn/winter months in temperate countries, where people tend to stay indoors in centrally heated homes, and where the warmer more humid air may be less favourable to longer-term airborne influenza survival versus the all-year-round low level of influenza incidence in tropical countries where indoor air-conditioning is the norm, when the drier, cooler air is less favourable to airborne influenza survival [34, 35, 47, 48].
Although the virus clearly needs to remain viable for long enough to transmit to and infect the next host, another important factor is how much viable virus is actually exhaled by an infected host and is then available in an aerosol to transmit to another nearby susceptible host. Some recent studies have shown that the amount of viable virus exhaled by an infected individual that is then available to pass to another individual is relatively low, even if the initial source host influenza viral load is very high [65••, 66, 67]. This implies that some sort of attenuation or degradation process occurs during this viral shedding or exhalation, indicating that prolonged and/or close contact may be required to cause a secondary infection. Subsequent successful infection will also depend on the degree of pre-existing immunity in the exposed contact, but this may all explain why that even at the height of a influenza season, only 20–30 % of people actually become infected with influenza [68•].
The emphasis is on aerosol transmission here, mainly because most non-intimate, casual and stranger ‘conversational’ encounters do not involve direct touching (though hand-shaking is a possibility in some situations) or shared fomite contact. Whilst it is well-documented that influenza can survive for several hours to days on various household materials and surfaces [69, 70], it is not clear if the amount of viable virus surviving on these surfaces, after touching then self-inoculating to mucous membranes, is sufficient to cause infection.
Studies attempting to quantify the types and numbers of viruses potentially present during such daily human-human interactions, using naturally infected volunteers should be possible. One way to do this in a study setting would be for infected volunteers to wear a lapel button air-sampler [71] for a few days whilst they are symptomatic and conducting their usual daily activities, whilst keeping an ‘encounter’ diary of the proximity and duration of each human contact in the following categories: intimate (family/household); work (at the workplace with colleagues) and casual/stranger (at shops, cinemas, restaurants) encounters. Each of the exposed contacts would have been immunologically characterised (using haemagglutination inhibition or microneutralisation assays) beforehand, as part of the study enrolment. Documented contacts would then be followed up clinically and via laboratory testing to see if they eventually develop infection with the same influenza virus, as confirmed using viral sequencing techniques.
This sort of approach has been used in human volunteer studies (where source and contacts interact in a specialised experimental environment), most recently in the EMIT study [72]. These sorts of studies are potentially fraught with possible confounders, e.g. the use of laboratory rather than wild-type viral strains, unnatural means of inoculating the index cases with these laboratory influenza strains, the impact of differing patterns of pre-existing immunity in the exposed contacts [73••, 74]. Yet, such experiments may be the only way to determine what concentration of airborne virus is required to cause secondary infections via the airborne route—at least in a specific, experimental group of well-characterised, albeit captive human volunteers.
Factors affecting host proximity
Factors affecting susceptible host proximity that may enhance influenza transmission, mainly relate to crowding, either indoors (e.g. at home, on public transport, at the workplace or in leisure or shopping amenities) or outdoors (e.g. at sporting, entertainment or political demonstration events). The acceptable degree of proximity is very much influenced by cultural norms, such as the amount of personal space acceptable between individuals in a crowd. For example, in Southeast Asia, it is acceptable for people tend to stand closer together in crowds than in Western European and North American countries, where such closer proximity may be found to be uncomfortable [75, 76 ]. The potential for virus transmission is clearly enhanced where susceptible hosts are closer together, as this intensifies any potential exposure from just a purely physical dispersion and dilution viewpoint [67].
The studies by Cowling and colleagues [41, 42, 43•, 44] have already been mentioned, but household transmission is a very specific scenario and it is not clear how household transmission events compare, in terms of numbers of secondary cases generated, with transmission occurring via more casual or ‘stranger’ style contacts in that population. The physical space available in households versus workplaces versus leisure amenities also varies considerably across the world, so the intensity of close, intimate household contact in a large, spacious home in North America, for example may be less than that in a more formal working environment in a cramped office in Hong Kong.
Overall, this hypothesis about human indoor crowding (i.e. susceptible host proximity) offers a very tempting explanation. The argument seems to work well for both colder, wetter temperate regions (where people stay inside centrally heated environments) and hotter, more humid subtropical and tropical regions (where people stay in air-conditioned environments), where such indoor crowding can enhance influenza transmission. Certainly, laboratory data on influenza survival indicates that the virus generally survives better in colder, drier environments (such as those produced by air-conditioning) rather than warmer, more humid environments (such as those produced by some forms of indoor heating) [77]. Perhaps in the latter case, the closer proximity of susceptible hosts outweighs the decreased survival of the virus, as it may be able to transmit into another susceptible host before it is sufficiently degraded by the environment to make it non-infectious.
Studies characterising human social mixing behaviour are generally model-based [78–81]. Whilst these models give a good idea of the contact networks when these people are well, these behaviours may change when people become ill. It is also unclear exactly how much transmission would actually occur between these contacts when these individuals are well versus when they are sick, as both the source (index case) and contacts may have differing levels of pre-existing specific and/or cross-reactive immunity to various pathogens. Although sensitivity analyses within these models can be reassuring to some extent, they cannot cover the variability of such individual characteristics—all of which can be different for different pathogens, e.g. non-influenza viruses tend not to cause the same degree of prostration that influenza does, so the behavioural differences may be less between well versus infected individuals for these non-influenza viruses. To take an extreme example, one of the reasons that the smallpox ‘contact-trace and isolate’ approach eradication campaign was so effective was that when individuals were infected with smallpox, they felt so unwell that they rarely left their bed or house [82], and were therefore easy to track and isolate. So, some comparative observational studies of the same individuals’ (volunteers) illness behaviour during periods when they are well versus when they are ill, when infected with each of the different specific pathogens (e.g. influenza or other respiratory viruses) would be useful to determine the validity of the assumptions made and outcomes produced from these models.
Another potentially important angle is the potential risks that different spoken languages may pose. Some common words in some languages may produce more aerosolised virus due to the way they are pronounced [83]. Together with the culturally acceptable closer proximity between people in some of the countries where such languages are spoken (e.g. Chinese and Japanese), this may predispose to a more rapid spread of seasonal influenza viruses in those populations. Certainly, in one series of experiments, there was a difference in airflow dissemination distance for certain numbers spoken in Mandarin Chinese compared to English [84].
Factors affecting host susceptibility
Variations in host (human) susceptibility, i.e. the ability of the immune system to protect against the virus, have been considered to be a major factor in influenza seasonality in human populations. Factors considered as having an impact on this include sunlight exposure and vitamin D levels [85, 86], peripheral blood lymphocyte activation responses [87], as well as psychological factors [88, 89]. Some or all of these factors may be relevant to different degrees in different individuals, but it is difficult to determine if any single one of these is necessarily predominant in most people. The seasonal change in sunlight exposure (and therefore human vitamin D levels) with latitude is perhaps the most generalisable [85, 86]. This also ties in with the more seasonally defined peaks and troughs of influenza incidence in more temperate countries where there is a distinct and significant change in the number of sunlight hours with the seasons. Whilst some aspects of this hypothesis are still controversial [90, 91], there seems to be increasing support for the role of adequate vitamin D levels being necessary to aid the effective immune clearance of respiratory infections [92–94].
Children are particularly vulnerable to influenza infection, as they do not have a long history of exposure to influenza and thus have not acquired a large spectrum of immunity to the different strains. Children are more susceptible to severe influenza infection than adults and may shed the virus at higher loads for longer, and are therefore significant sources of influenza infection for adults who come into contact with them. Whilst many influenza transmission and intervention modelling studies have been performed in schools, the recommended intervention of widespread school closures are rather impractical and may have severe economic impact on parents and carers alike [95–98].
Using a different approach, a series of papers modelling the potential effect of immunising school children (aged 2–16 years) against seasonal influenza has demonstrated significant benefits in terms of cost-effectiveness and cost-savings [99–104]. This apparent benefit has been so convincing that this paediatric influenza immunisation policy has now been implemented in UK schools, from 2014 onwards. It will be of interest to see if the predicted benefits from these models become a reality in this population, in terms of lower numbers of influenza infections in both the paediatric and their related adult populations, over the next few influenza seasons. Depending on the uptake and effectiveness of this vaccination programme, this may reduce the amplitude of the annual seasonal influenza incidence peak. It will be of even more interest to see if this paediatric influenza immunisation policy can also affect the distinctive timing of this seasonal influenza peak.
Even newborn babies have been shown to acquire some maternal antibodies that are potentially protective (as demonstrated by postnatal serological measurements) to currently circulating viruses, either by natural infection or influenza immunisation of the mother [105–107]. In fact guidelines for pregnant women now recommend influenza vaccination at any time during their pregnancy [108–110], both to protect the mother during pregnancy, but also, to offer the possibility that in the third trimester, vaccine-induced maternal antibodies may pass to the newborn and offer some short-lived protection postnatally, whilst its own immune system matures. If this recommendation is adopted widely, it will be of interest to see how this may possibly alter the local seasonal influenza peak incidence and timing, as compared to the previous era when influenza immunisation during pregnancy was rare.
The rapidity with which a new pandemic influenza virus moves through a global population again suggests that existing host immunity is an important factor in the establishment of seasonality. Once the new virus has infected the majority of the global population, then, presumably, the intrinsic oscillation cycles of annual seasonal influenza epidemics will begin. This pattern has been consistently followed in the 1918 A/H1N1, 1957 AH2N2, 1968 A/H3N2 and 2009 A/H1N1pdm09 influenza pandemics over the past century [111]. This indicates that the lack of host immunity to the new virus is important to allow the seeding of a new virus (and the displacement of the previous subtype) prior to the kick-starting of the intrinsic seasonal influenza oscillation cycle.
Interestingly, the apparent duration of the previous influenza pandemics seem to be similar—all lasting around 6–12 months [111, 112]. Whilst it is difficult to ascertain the exact onset of a pandemic (when a new influenza virus enters the human population) and its end (when the new virus has effectively infected virtually every individual on the planet), it is remarkable that despite the development of accessible, rapid, global transport, the new virus still needs a similar amount of time to reach all the susceptible individuals on the planet.
Data published by the International Air Travel Association showed that during 1950–2010, the global air passenger numbers grew from 0 to about 3.5 billion [113], a growth rate of about 58.3 × 106 passengers/year. During the same period, the world population grew from 2.5 to 7 billion [114], a growth rate of about 75 × 106 total number of living humans on Earth/year. Despite the crudeness of this comparison (as some people travel frequently and others not at all—though they may well have sufficient contact with those that do), the similarity of these figures suggests that despite very different world populations at the time of each of the influenza pandemics, the travel-assisted spread of a pandemic virus, internationally, to a rapidly increasing global population within a seemingly constant 6–12-month period, has been made potentially possible by a similar and matching increase in global passenger transport.
Apart from man-made modes of transport for the virus, there has been a long-standing hypothesis about the atmospheric transport of influenza viruses [115], though this is very difficult to prove. Even with the improved sensitivity of molecular detection assays for influenza, it is not possible to sample any significant fraction of the vast atmospheric air volume to confirm or exclude the presence and movement of viable influenza virus at various altitudes in different directions. However, given the intense solar ultraviolet exposure to which these atmospheric airborne viruses would be subjected, their long-term, airborne viability seems unlikely [54].
Human (host) movement
The hypothesis of global, travel-assisted transport of pandemic influenza viruses above has received some support from various recent studies suggesting that human movement (as carriers of the virus) may be an important factor in the patterns of influenza infection that we are observing, globally [116, 117, 118•, 119]. However, it is difficult to ascertain how significant this contributor might be to the global patterns of influenza actually observed. Whilst the approaches are elegant, these inferences are nevertheless drawn from human and viral population level analyses, coupling influenza virus phylodynamics, patterns of influenza antigenicity and passenger transport data, rather than from data obtained from directly sampling individuals travelling between various destinations. Although this may invalidate this modelling approach, it is difficult to evaluate the various assumptions in the model (as with any model) without some empirical data from those who actually travel these routes and test whether or not they are infected with influenza, and ascertain exactly where their infection originated and their final destination—indeed some of the modellers themselves have also called for more of this type of epidemiological data [54].
With a dedicated laboratory network and enthusiastic and committed participant/passenger efforts, it should not be too difficult. Consenting adults and their families could be supplied with several self-sampling viral swab kits for each person in their travelling party. They would then be instructed to swab themselves just before they travel (either a nasopharyngeal or oropharyngeal swab), then again during any prolonged stopovers (say >12 h), then again upon arrival at their destination. They would then all swab themselves further if any of their travelling party became symptomatic during their holidays, then again before they boarded their return flight (and again, during any prolonged stopover on the return flight), then again once they arrived home. In addition, they would be asked to swab themselves 3–4 days later after returning home, whether symptomatic or not, just to catch any viral infection that may have been incubating during their return journey. All the swabs would then be sent to the designated research lab for testing and sequencing, if positive for influenza or any other respiratory viruses of interest. The participants would be advised to store any samples (and unused virus transport medium with the sampling kits, which might be needed later) in a fridge whenever possible—special containers and labels would be provided. Ideally, any swabs that are taken would be sent to any of a variety of participating laboratories around the world that is closest to them for testing, at the origin, stopover and destination stops, to avoid carrying clinical samples on the plane itself. This will also reduce the delay in testing these samples and maximise their viral yield. Thus, perhaps, only certain routes with such collaborating laboratories already in place would be eligible for such a study.
Again, it is remarkable that despite the massive rise in air passenger numbers over the last 40–50 years [113], several studies that have reviewed the timing of past annual seasonal influenza epidemics have shown that the timing of peak influenza incidence has not changed much (if at all) during this period [120–123]. Perhaps, this could be considered as additional support for a strong, fundamental intrinsic oscillation cycle, as advocated by some researchers [19, 38••, 53–55].
Conclusions
Are we any further forward? Yes, we think so. With each new study, some old questions are answered and new questions are raised. Experiments (and models) can be designed to address them in the hope that we may eventually achieve a level of understanding that has both a practical utility, as well as being a fundamental scientific achievement. However, ongoing new developments in technology and new social trends (like the massive increase in air travel to previously more remote and/or less accessible areas for new tourism—like China and Mongolia, the explosion of the Internet with the rapid rise and increasingly widespread use of social media) may keep introducing new factors that may add to or change the already complex interaction of the contributing factors currently under investigation.
One example of this is the current trend in diagnostic technology for respiratory pathogens, where there is an increasingly widespread use of multiplex PCR or microarray-based assays that allows the detection of multiple pathogens in one sample.
With this technology, it is possible now to assess the clinical impact of influenza mono- or co-infection with other respiratory viruses on the clinical severity of illness, and how this may impact on human illness (and therefore social mixing) behaviour. With a little diagnostic assay customisation, it is also possible to quantify the level and duration of viral shedding from different sample types (and therefore anatomical sites). Co-infections may result in higher influenza viral loads to be shed via different routes (i.e. airborne and contact) for longer, thereby enhancing the potential transmissibility of influenza in such patients. In fact, it is still unclear whether multiple infections with respiratory viruses necessarily leads to more severe disease [124••, 125–128], but the use of these assays is still expanding (they are not cheap at present) and it is likely that a clearer picture will emerge on this question, fairly soon.
So, perhaps any intrinsic host-pathogen-environment oscillation cycle is dependent on not just one pathogen (influenza), but also its interactions with other, co-infecting respiratory pathogens (together with their varied host immune experience and responses), which were not routinely detected using older, less sensitive diagnostic assays. Thus, age-related, immunologically variable, multiply co-infected individuals (probably mostly children) could also be contributing to such an intrinsic oscillation. However, like the other factors driving influenza seasonality, the contribution and impact of these co-infecting respiratory viruses will vary between different populations, cultures and climates, via changing immunological host profiles which are themselves driven by their local seasonal respiratory virus incidence, in these environments. Then, as always, more studies from different regions will be needed to clarify the answer to these (and other related) questions, to allow us to further understand the underlying basis for the global seasonality of influenza.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Government of Canada. Surveillance of West Nile Virus. http://healthycanadians.gc.ca/diseases-conditions-maladies-affections/disease-maladie/west-nile-nil-occidental/surveillance-eng.php. [16 February 2016].
van Elden LJ, Nijhuis M, Schipper P, et al. Simultaneous detection of influenza viruses A and B using real-time quantitative PCR. J Clin Microbiol. 2001;39:196–200.
Herrmann B, Larsson C, Zweygberg BW. Simultaneous detection and typing of influenza viruses A and B by a nested reverse transcription-PCR: comparison to virus isolation and antigen detection by immunofluorescence and optical immunoassay (FLU OIA. J Clin Microbiol. 2001;39:134–8.
Templeton KE, Scheltinga SA, Beersma MF, et al. Rapid and sensitive method using multiplex real-time PCR for diagnosis of infections by influenza A and influenza B viruses, respiratory syncytial virus, and parainfluenza viruses 1, 2, 3, and 4. J Clin Microbiol. 2004;42:1564–9.
Patterson Ross Z, Komadina N, Deng YM, et al. Inter-seasonal influenza is characterized by extended virus transmission and persistence. PLoS Pathog. 2015;11:e1004991.This is a very interesting and possibly significant paper—but needs other studies from elsewhere to show something similar, i.e. whether the introduction of out of season influenza viruses can seed and result in a local epidemic in that area, as well as the characterization of inter-seasonal influenza dynamics in Australia.
Nelson MI, Simonsen L, Viboud C, et al. Phylogenetic analysis reveals the global migration of seasonal influenza A viruses. PLoS Pathog. 2007;3:1220–8.
Rambaut A, Pybus OG, Nelson MI, et al. The genomic and epidemiological dynamics of human influenza A virus. Nature. 2008;453:615–9.
Bahl J, Nelson MI, Chan KH, et al. Temporally structured metapopulation dynamics and persistence of influenza A H3N2 virus in humans. Proc Natl Acad Sci U S A. 2011;108:19359–564.
Duncan LA, Schaller M, Park JH. Perceived vulnerability to disease: development and validation of a 15-item self-report instrument. Pers Indiv Differ. 2009;47:541–6.
Hamamura T, Park JH. Regional differences in pathogen prevalence and defensive reactions to the “swine flu” outbreak among east Asians and westerners. Evol Psychol. 2010;8:506–15.
Lau JT, Griffiths S, DW A, et al. Changes in knowledge, perceptions, preventive behaviours and psychological responses in the pre-community outbreak phase of the H1N1 epidemic. Epidemiol Infect. 2011;139:80–90.
van der Stuyft P, Delgado E, Sorensen SC. Utilisation rates and expenditure for public and private, curative-care services in semi-urban Guatemala. Ann Trop Med Parasitol. 1997;91:209–16.
Leon M. Perceptions of health care quality in Central America. Int J Qual Health Care. 2003;15:67–71.
Lindblade KA, Johnson AJ, Arvelo W, et al. Low usage of government healthcare facilities for acute respiratory infections in Guatemala: implications for influenza surveillance. BMC Public Health. 2011;11:885.
Goldman N, Pebley AR, Gragnolati M. Choices about treatment for ARI and diarrhea in rural Guatemala. Soc Sci Med. 2002;55:1693–712.
Burton DC, Flannery B, Onyango B, et al. Healthcare-seeking behaviour for common infectious disease-related illnesses in rural Kenya: a community-based house-to-house survey. J Health Popul Nutr. 2011;29:61–70.
Yang J, Jit M, Leung KS, et al. The economic burden of influenza-associated outpatient visits and hospitalizations in China: a retrospective survey. Infect Dis Poverty. 2015;4:44.
Nicholson KG, Wood JM, Zambon M. Influenza. Lancet. 2003;362:1733–45.
Moorthy M, Castronovo D, Abraham A, et al. Deviations in influenza seasonality: odd coincidence or obscure consequence? Clin Microbiol Infect. 2012;18:955–62.
Chen Z, Zhu Y, Wang Y, et al. Association of meteorological factors with childhood viral acute respiratory infections in subtropical China: an analysis over 11 years. Arch Virol. 2014;159:631–9.
Chen ZR, Ji W, Wang YQ, et al. Etiology of acute bronchiolitis and the relationship with meteorological conditions in hospitalized infants in China. J Formos Med Assoc. 2014;113:463–9.
Soebiyanto RP, Clara WA, Jara J, et al. Associations between seasonal influenza and meteorological parameters in Costa Rica, Honduras and Nicaragua. Geospat Health. 2015;10:372.There has been a relative scarcity of influenza incidence-climate data from the Central American countries—this paper has filled some of this data gap.
Agrawal AS, Sarkar M, Chakrabarti S, et al. Comparative evaluation of real-time PCR and conventional RT-PCR during a 2 year surveillance for influenza and respiratory syncytial virus among children with acute respiratory infections in Kolkata, India, reveals a distinct seasonality of infection. J Med Microbiol. 2009;58:1616–22.
Jaakkola K, Saukkoriipi A, Jokelainen J, et al. Decline in temperature and humidity increases the occurrence of influenza in cold climate. Environ Health. 2014;13:22.
Iha Y, Higa F, Sunagawa S, et al. Effect of climatic conditions on epidemic patterns of influenza in Okinawa, Japan, during the pandemic of 2009: surveillance of rapid antigen test results. Jpn J Infect Dis. 2012;65:295–300.
Jusot JF, Adamou L, Collard JM. Influenza transmission during a one-year period (2009-2010) in a Sahelian city: low temperature plays a major role. Influenza Other Respir Viruses. 2012;6:87–9.
Dangi T, Jain B, Singh AK, et al. Influenza virus genotypes circulating in and around Lucknow, Uttar Pradesh, India, during post pandemic period, August 2010–September 2012. Indian J Med Res. 2014;139:418–26.
Soebiyanto RP, Clara W, Jara J, et al. The role of temperature and humidity on seasonal influenza in tropical areas: Guatemala, El Salvador and Panama, 2008-2013. PLoS One. 2014;9:e100659.There has been a relative scarcity of influenza incidence-climate data from the Central American countries—this paper has filled some of this data gap.
Martin AJ, Gardner PS, McQuillin J. Epidemiology of respiratory viral infection among paediatric inpatients over a six-year period in north-East England. Lancet. 1978;2:1035–8.
Chadha MS, Broor S, Gunasekaran P, et al. Multisite virological influenza surveillance in India: 2004-2008. Influenza Other Respir Viruses. 2012;6:196–203.
Viegas M, Barrero PR, Maffey AF, et al. Respiratory viruses seasonality in children under five years of age in Buenos Aires, Argentina: a five-year analysis. J Infect. 2004;49:222–8.
Chew FT, Doraisingham S, Ling AE, et al. Seasonal trends of viral respiratory tract infections in the tropics. Epidemiol Infect. 1998;121:121–8.
Freitas FT. Sentinel surveillance of influenza and other respiratory viruses, Brazil, 2000–2010. Braz J Infect Dis. 2013;17:62–8.
Tang JW, Lai FY, Wong F, et al. Incidence of common respiratory viral infections related to climate factors in hospitalized children in Hong Kong. Epidemiol Infect. 2010;138:226–35.
Tang JW, Lai FY, Nymadawa P, et al. Comparison of the incidence of influenza in relation to climate factors during 2000–2007 in five countries. J Med Virol. 2010;82:1958–65.
Shoji M, Katayama K, Sano K. Absolute humidity as a deterministic factor affecting seasonal influenza epidemics in Japan. Tohoku J Exp Med. 2011;224:251–6.
Rao BL, Banerjee K. Influenza surveillance in Pune, India, 1978–90. Bull World Health Organ. 1993;71:177–81.
Dowell SF. Seasonality-still confusing. Epidemiol Infect. 2012;140:87–90 A very useful editorial overview of the various factors possibly contributing to the seasonality of influenza.
Murray EL, Klein M, Brondi L, et al. Rainfall, household crowding, and acute respiratory infections in the tropics. Epidemiol Infect. 2012;140:78–86 A very well-designed study that shows how human behaviour (indoor crowding during heavy rains) can significantly contribute to the risk of influenza transmission. This study from a resource-limited region, using a different design and investigating a slightly different question provides a useful contrast to the household influenza transmission studies of Cowling and colleagues from Hong Kong—whose studies did not record any indoor environmental factors that may have affected the airborne survival and therefore the transmissibility of influenza viruses that were able to cause secondary infections.
Paynter S. Humidity and respiratory virus transmission in tropical and temperate settings. Epidemiol Infect. 2015;143:1110–8.
Cowling BJ, Chan KH, Fang VJ, et al. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009;151:437–46.
Cowling BJ, Chan KH, Fang VJ, et al. Comparative epidemiology of pandemic and seasonal influenza A in households. N Engl J Med. 2010;362:2175–84.
Cowling BJ, Ip DK, Fang VJ, et al. Aerosol transmission is an important mode of influenza A virus spread. Nat Commun. 2013;4:1935. An interesting study where Cowling and colleagues pooled their considerable data obtained from household influenza transmission studies over several years in a mathematical model that demonstrated a significant contribution to influenza transmission via the aerosol route. Although some might dispute their approach, it clearly demonstrates the potential for some influenza transmission to occur via aerosols.
Tsang TK, Lau LL, Cauchemez S, et al. Household transmission of influenza virus. Trends Microbiol. 2016;24:123–33.
Keatinge WR, Coleshaw SR, Holmes J. Changes in seasonal mortalities with improvement in home heating in England and Wales from 1964 to 1984. Int J Biometeorol. 1989;33:71–6.
Hirota Y, Takeshita S, Kataoka K, et al. Individual and environmental characteristics related to influenza-like illness among children: a school-based case-control study. Nihon Eiseigaku Zasshi. 1992;47:587–99.
Myatt TA, Kaufman MH, Allen JG, et al. Modeling the airborne survival of influenza virus in a residential setting: the impacts of home humidification. Environ Health. 2010;9:55.
Koep TH, Enders FT, Pierret C, et al. Predictors of indoor absolute humidity and estimated effects on influenza virus survival in grade schools. BMC Infect Dis. 2013;13:71.
Tseng CC, Chang LY, Li CS. Detection of airborne viruses in a pediatrics department measured using real-time qPCR coupled to an air-sampling filter method. J Environ Health. 2010;73:22–8.
Goyal SM, Anantharaman S, Ramakrishnan MA, et al. Detection of viruses in used ventilation filters from two large public buildings. Am J Infect Control. 2011;39:e30–8.
Bischoff WE, Swett K, Leng I, et al. Exposure to influenza virus aerosols during routine patient care. J Infect Dis. 2013;207:1037–46.
Lindsley WG, Noti JD, Blachere FM, et al. Viable influenza A virus in airborne particles from human coughs. J Occup Environ Hyg. 2015;12:107–13 One of many useful studies from this group demonstrating the viability of airborne influenza virus and the potential for them to then cause secondary cases of influenza (secondary infections). There has been a long-standing debate at WHO (World Health Organization) level about whether influenza RNA detected in air-samples necessarily represent truly viable virus that is capable of causing secondary infections. With multiple studies from this and other groups demonstrating the presence of live influenza virus in aerosols, we now cannot ignore the risk posed by aerosolised influenza to cause secondary cases of influenza when exposed to an infected source—possibly some distance away—requiring the appropriate level of infection control to be instigated.
Dushoff J, Plotkin JB, Levin SA, et al. Dynamical resonance can account for seasonality of influenza epidemics. Proc Natl Acad Sci U S A. 2004;101:16915–6.
Lofgren E, Fefferman NH, Naumov YN, et al. Influenza seasonality: underlying causes and modeling theories. J Virol. 2007;81:5429–36.
Tamerius J, Nelson MI, Zhou SZ, et al. Global influenza seasonality: reconciling patterns across temperate and tropical regions. Environ Health Perspect. 2011;119:439–45. doi:10.1289/ehp.1002383.
The Lancet Infectious Diseases. 7 billion of us. Lancet Infect Dis 2011;11:801. doi: 10.1016/S1473-3099(11)70296-1.
Griffths PD. When prevalence of infection may not directly reflect the burden of disease. Rev Med Virol. 2016;26:2–3.
Tan L, Cheng L, Yan W, et al. Using daily syndrome-specific absence data for early detection of school outbreaks: a pilot study in rural China. Public Health. 2014;128:792–8.
Peng Z, Wu P, Ge L, et al. Rural villagers and urban residents exposure to poultry in China. PLoS One. 2014;9:e95430.
Zhang Y, Li L, Dong X, et al. Influenza surveillance and incidence in a rural area in China during the 2009/2010 influenza pandemic. PLoS One. 2014;9:e115347.
Jiang CQ, Lessler J, Kim L, et al. Cohort profile: a study of influenza immunity in the urban and rural Guangzhou region of China: the Fluscape Study. Int J Epidemiol 2016. pii: dyv353.
Chan PK, Mok HY, Lee TC, et al. Seasonal influenza activity in Hong Kong and its association with meteorological variations. J Med Virol. 2009;81:1797–806.
Mahamat A, Dussart P, Bouix A, et al. Climatic drivers of seasonal influenza epidemics in French Guiana, 2006–2010. J Infect. 2013;67:141–7.
Imai C, Brooks WA, Chung Y, et al. Tropical influenza and weather variability among children in an urban low-income population in Bangladesh. Glob Health Action. 2014;7:24413.
Milton DK, Fabian MP, Cowling BJ, et al. Influenza virus aerosols in human exhaled breath: particle size, culturability, and effect of surgical masks. PLoS Pathog. 2013;9:e1003205. An important paper showing that whilst viable influenza viruses can be detected in the exhaled, airborne droplets from infected sources, the actual number of these viable viruses is very low compared to the level of detectable influenza RNA in these same airborne droplets. This mitigates but does not entirely remove the concerns about the significance of the airborne/aerosol route of influenza infection—particularly in healthcare settings where multiple infected sources may be exhaling infectious virus within a confined environment for hours to days at a time—often assisted by oxygen masks and nebulisers that may further assist the environment dissemination of such aerosols.
Hatagishi E, Okamoto M, Ohmiya S, et al. Establishment and clinical applications of a portable system for capturing influenza viruses released through coughing. PLoS One. 2014;9:e103560.
Tang JW, Gao CX, Cowling BJ, et al. Absence of detectable influenza RNA transmitted via aerosol during various human respiratory activities—experiments from Singapore and Hong Kong. PLoS One. 2014;9:e107338.
Tang JW. Investigating the airborne transmission pathway—different approaches with the same objectives. Indoor Air. 2015;25:119–24. A useful overview in a primarily engineering journal, of the various aspects of the methods and specialist expertise and knowledge in further elucidating the aerosol transmission pathway for influenza and other airborne pathogens—involving both clinical air-sampling and diagnostic pathogen detection methods, as well as engineering airflow visualisation and dynamics modelling.
Mukherjee DV, Cohen B, Bovino ME, et al. Survival of influenza virus on hands and fomites in community and laboratory settings. Am J Infect Control. 2012;40:590–4.
Oxford J, Berezin EN, Courvalin P, et al. The survival of influenza A (H1N1)pdm09 virus on 4 household surfaces. Am J Infect Control. 2014;42:423–5.
SKC. Button sampler. http://www.skcltd.com/index.php/products2/9-uncategorised/204-button-sampler [16 February 2016].
Evaluating Modes of Influenza Transmission (EMIT): http://nottingham.ac.uk/research/groups/healthprotection/projects/index.aspx [30 August 2016].
Killingley B, Enstone J, Booy R, et al. Potential role of human challenge studies for investigation of influenza transmission. Lancet Infect Dis. 2011;11:879–86 These two commentaries (above and below) discuss some issues around possible confounders for human volunteer transmission experiments with influenza. Such experiments are necessarily artificial (as well as costly), and the trick is to try to neutralise these potential confounders through careful experimental design—so that the final outcomes are applicable to the wild-type virus and real-life potential transmission situations.
Tang JW. Pre-existing immunity in human challenge studies of influenza transmission. Lancet Infect Dis. 2012;12:744 .author reply 744-5
Sussman NM, Rosenfeld HM. Influence of culture, language and sex on conversational distance. J Pers Soc Psychol. 1982;106:215–25.
Bond R, Smith PB. Culture and conformity: a meta-analysis of studies using Aschís (1952, 1956) line judgment task. Psychol Bull. 1996;119:111–37.
Tang JW. The effect of environmental parameters on the survival of airborne infectious agents. J R Soc Interface. 2009;6:S737–46.
Funk S, SalathÈ M, Jansen VA. Modelling the influence of human behaviour on the spread of infectious diseases: a review. J R Soc Interface. 2010;7:1247–56.
Read JM, Lessler J, Riley S, et al. Social mixing patterns in rural and urban areas of southern China. Proc Biol Sci. 2014;281:20140268.
Kucharski AJ, Kwok KO, Wei VW, et al. The contribution of social behaviour to the transmission of influenza A in a human population. PLoS Pathog. 2014;10:e1004206.
Kwok KO, Cowling BJ, Wei VW, et al. Social contacts and the locations in which they occur as risk factors for influenza infection. Proc Biol Sci. 2014;281:20140709.
Henderson DA, Inglesby TV, Bartlett JG, et al. Smallpox as a biological weapon: medical and public health management. Working group on civilian biodefense. JAMA. 1999;281:2127–37.
Inouye SSARS. Transmission: language and droplet production. Lancet. 2003;362:170.
Jiang M, Nicolle A, Klettner C, et al. Shadowgraph imaging and quantitative analysis of human breathing and talking—potential risks for cross-infection. Abstract/Paper. Healthy Buildings, 10th International Conference, Brisbane, Australia. 8–12 July 2012.
Cannell JJ, Vieth R, Umhau JC, et al. Epidemic influenza and vitamin D. Epidemiol Infect. 2006;134:1129–40.
Cannell JJ, Zasloff M, Garland CF, et al. On the epidemiology of influenza. Virol J. 2008;5:29.
Michelis FV, Delitheos AK, Tiligada E. Seasonal influence on mitogen and cyclosporin responses of peripheral blood lymphocytes. Int Immunopharmacol. 2013;16:154–9.
Sher L. Effects of seasonal mood changes on seasonal variations in coronary heart disease: role of immune system, infection, and inflammation. Med Hypotheses. 2001;56:104–6.
De Jong S, Neeleman M, Luykx JJ, et al. Seasonal changes in gene expression represent cell-type composition in whole blood. Hum Mol Genet. 2014;23:2721–8.
Radonovich LJ, Martinello RA, Hodgson M, et al. Influenza and ultraviolet germicidal irradiation. Virol J. 2008;5:149.
Cannell JJ, Zasloff M, Garland CF, et al. Commentary. On the epidemiology of influenza: reply to Radonovich et al. Virol J. 2009;6:121.
Bergman P, Norlin AC, Hansen S, et al. Vitamin D3 supplementation in patients with frequent respiratory tract infections: a randomised and double-blind intervention study. BMJ Open. 2012;2:e001663.
Science M, Maguire JL, Russell ML, et al. Low serum 25-hydroxyvitamin D level and risk of upper respiratory tract infection in children and adolescents. Clin Infect Dis. 2013;57:392–7.
Kroner Jde C, Sommer A, Fabri M. Vitaminn D every day to keep the infection away? Nutrients. 2015;7:4170–1488.
Glass LM, Glass RJ. Social contact networks for the spread of pandemic influenza in children and teenagers. BMC Public Health. 2008;8:61.
House T, Baguelin M, Van Hoek AJ, et al. Modelling the impact of local reactive school closures on critical care provision during an influenza pandemic. Proc Biol Sci. 2011;278:2753–60.
Toth DJ, Leecaster M, Pettey WB, et al. The role of heterogeneity in contact timing and duration in network models of influenza spread in schools. J R Soc Interface. 2015;12:20150279.
Fumanelli L, Ajelli M, Merler S, et al. Model-based comprehensive analysis of school closure policies for mitigating influenza epidemics and pandemics. PLoS Comput Biol. 2016;12:e1004681.
Salo H, Kilpi T, Sintonen H, et al. Cost-effectiveness of influenza vaccination of healthy children. Vaccine. 2006;24:4934–41.
Vynnycky E, Pitman R, Siddiqui R, et al. Estimating the impact of childhood influenza vaccination programmes in England and Wales. Vaccine. 2008;26:5321–30.
Nichol KL. Cost-effectiveness and socio-economic aspects of childhood influenza vaccination. Vaccine. 2011;29:7554–8.
Pitman RJ, White LJ, Sculpher M. Estimating the clinical impact of introducing paediatric influenza vaccination in England and Wales. Vaccine. 2012;30:1208–24.
Pitman R, Nagy LD, Sculpher MJ. Cost-effectiveness of childhood influenza vaccination in England and Wales: results from a dynamic transmission model. Vaccine. 2013;31:927–42.
Thorrington D, Jit M, Eames K. Targeted vaccination in healthy school children—can primary school vaccination alone control influenza? Vaccine. 2015;33:5415–24.
MacDonald NE, Riley LE, Steinhoff MC. Influenza immunization in pregnancy. Obstet Gynecol. 2009;114:365–8.
Steinhoff MC, Omer SB, Roy E, et al. Influenza immunization in pregnancy—antibody responses in mothers and infants. N Engl J Med. 2010;362:1644–6.
Steinhoff MC, Omer SBA. Review of fetal and infant protection associated with antenatal influenza immunization. Am J Obstet Gynecol. 2012;207:S21–7.
Committee on infectious diseases. Recommendations for prevention and control of influenza in children, 2013–2014. Pediatrics. 2013;132:e1089–104.
Public Health Agency of Canada. Canadian immunization guide. Part 3 Vaccination of specific populations. Immunization in pregnancy and breastfeeding. 2015. http://www.phac-aspc.gc.ca/publicat/cig-gci/p03-04-eng.php [16 February 2016].
Public Health England. Summary of influenza immunisation policy. Recommendations for the use of the vaccines. http://www.guidelines.co.uk/phe/flu [16 February 2016].
Kilbourne ED. Influenza pandemics of the twentieth century. Emerg Infect Dis. 2006;12:9–14.
U.S. Department of Health & Human Services. Pandemic flu history. http://www.flu.gov/pandemic/history/ [16 February 2016].
Oxley D, Jain C. Global air passenger markets: riding out periods of turbulence. International Air Transport Association (IATA). Chapter 1.4, in "The Travel & Tourism Competitiveness Report 2015". http://www3.weforum.org/docs/TT15/WEF_TTCR_Chapter1.4_201. [16 February 2016].
Worldometers. World population: past, present, and future. http://www.worldometers.info/world-population/ [16 February 2016].
Hammond GW, Raddatz RL, Gelskey DE. Impact of atmospheric dispersion and transport of viral aerosols on the epidemiology of influenza. Rev Infect Dis. 1989;11:494–7.
Zinder D, Bedford T, Baskerville EB, et al. Seasonality in the migration and establishment of H3N2 influenza lineages with epidemic growth and decline. BMC Evol Biol. 2014;14:272.
Tan Y, Lam TT, Wu C, et al. Increasing similarity in the dynamics of influenza in two adjacent subtropical Chinese cities following the relaxation of border restrictions. J Gen Virol. 2014;95:531–8.
Lemey P, Rambaut A, Bedford T, et al. Unifying viral genetics and human transportation data to predict the global transmission dynamics of human influenza H3N2. PLoS Pathog. 2014;10:e1003932. An interesting population level study assessing the contribution of global transport to the transmission and seasonality of influenza around the world. But obviously limited to the data available and influenza infections occur in many members of the population at various locations who don’t travel, whose influenza viruses have not been sequenced.
Bedford T, Riley S, Barr IG, et al. Global circulation patterns of seasonal influenza viruses vary with antigenic drift. Nature. 2015;523:217–20.
Dowell SF. Seasonal variation in host susceptibility and cycles of certain infectious diseases. Emerg Infect Dis. 2001;7:369–74.
Viboud C, Tam T, Fleming D, et al. 1951 influenza epidemic, England and Wales, Canada, and the United States. Emerg Infect Dis. 2006;12:661–8.
Nelson MI, Holmes EC. The evolution of epidemic influenza. Nat Rev Genet. 2007;8:196–205.
Truscott J, Fraser C, Cauchemez S, et al. Essential epidemiological mechanisms underpinning the transmission dynamics of seasonal influenza. J R Soc Interface. 2012;9:304–12.
Kouni S, Karakitsos P, Chranioti A, et al. Evaluation of viral co-infections in hospitalized and non-hospitalized children with respiratory infections using microarrays. Clin Microbiol Infect. 2013;19:772–7. This paper and the remainder that follow examine co-infections with one or more respiratory viruses in the same patient. This raises the possibility that influenza infectiousness may be increased (or possibly decreased) in the presence of other co-infecting respiratory viruses. But this effect has not yet been evaluated—and it may vary depending on which other respiratory virus species is co-infecting with influenza. These questions open up a host of other possible studies.
Goka E, Vallely P, Mutton K, et al. Influenza a viruses dual and multiple infections with other respiratory viruses and risk of hospitalisation and mortality. Influenza Other Respir Viruses. 2013;7:1079–87.
Asner SA, Science ME, Tran D, et al. Clinical disease severity of respiratory viral co-infection versus single viral infection: a systematic review and meta-analysis. PLoS One. 2014;9:e99392.
Goka EA, Vallely PJ, Mutton KJ, et al. Single, dual and multiple respiratory virus infections and risk of hospitalization and mortality. Epidemiol Infect. 2015;143:37–47.
Asner SA, Rose W, Petrich A, et al. Is virus coinfection a predictor of severity in children with viral respiratory infections? Clin Microbiol Infect. 2015;21:264.e1–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Julian Wei-Tze Tang declares that he has no conflict of interest. Dr. Tze Ping Loh declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Viral Infections
Rights and permissions
About this article

Cite this article
Tang, J.WT., Loh, T.P. Influenza Seasonality. Curr Treat Options Infect Dis 8, 343–367 (2016). https://doi.org/10.1007/s40506-016-0088-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40506-016-0088-2