
Abstract
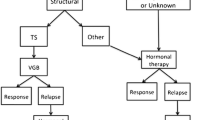
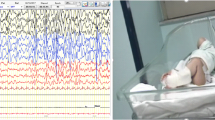
West syndrome (WS), also known as infantile spasms, occurs in infancy with a peak between 4 and 7 months. Spasms, neurodevelopmental regression and hypsarrhythmia on electroencephalogram (EEG) basically define WS. The International League Against Epilepsy commission classifies the aetiologies of WS into genetic, structural, metabolic and unknown. Early diagnosis and a shorter lag time to treatment are essential for the overall outcome of WS patients. These goals are feasible with the addition of brain magnetic resonance imaging (MRI) and genetic and metabolic testing. The present work analysed the medical literature on WS and reports the principal therapeutic protocols of its management. Adrenocorticotropic hormone (ACTH), vigabatrin (VGB) and corticosteroids are the first-line treatments for WS. There is no unique therapeutic protocol for ACTH, but most of the evidence suggests that low doses are as effective as high doses for short-term treatment, which is generally 2 weeks followed by dose tapering. VGB is generally administered at doses from 50 to 150 mg/kg/day, but its related retinal toxicity, which occurs in 21–34% of infants, is most frequently observed when treatment periods last longer than 6 months. Among corticosteroids, a treatment of 14 days of oral prednisolone (40–60 mg/day) has been considered effective and well tolerated. Considering that an early diagnosis and a shorter lag time to treatment are essential for successful outcomes in these patients, further studies on efficacy of the different therapeutic approaches with evaluation of final outcome after cessation of therapy are needed.
Similar content being viewed by others

References
Pavone P, Striano P, Falsaperla R, Pavone L, Ruggieri M. Infantile spasms syndrome, West syndrome and related phenotypes: what we know in 2013. Brain Dev. 2014;36:739–51.
West WJ. On a peculiar form of infantile convulsions. Lancet. 1841;1:724–5.
Wilmshurst JM, Ibekwe RC, O’ Callaghan FJK. Epileptic spasms—175 years on: trying to teach and old dog new tricks. Seizure. 2017;44:81–6.
Rantala H, Putkonen T. Occurence, outcome and prognostic factors of infantile spasms and Lennox–Gastaut syndrome. Epilepsia. 1999;40:286–9.
Commision and Classification and Terminology of the International. League against epilepsy. Workshop on infantile spasms. Epilepsia. 1992;33:195.
Wong M, Trevathan E. Infantile spasms. Pediatr Neurol. 2001;24:89–98.
Lux AL, Osborne JP. A proposal for case definitions and outcome measures in studies of infantile spasms and West syndrome: consensus statement of the west Delphi group. Epilepsia. 2004;45:1416–28.
Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, Cross JH, Van Emde Boas W, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE commission on classification and terminology 2005–2009. Epilepsia. 2010;51:676–85.
Gibbs EL, Fleming MM, Gibbs FA. Diagnosis and prognosis of hypsarrhythmia and infantile spasms. Pediatrics. 1954;13:66–73.
Caraballo RH, Ruggieri V, Gonzalez G, Cerosimo R, Gamboni B, Rey A, et al. Infantile spasms without hypsarrhythmia: a study of 16 cases. Seizure. 2011;20:197–202.
Kossof EH. Infantile spasms. Neurologist. 2010;2:69–75.
Baram TZ. Models for infantile spasms: an arduous journey to the Holy Grail. Ann Neurol. 2007;61:89–91.
Velisek L, Jehle K, Asche S, Veliskova J. Model of infantile spasms induced by N-methyl-d-aspartic acid in prenatally impaired brain. Ann Neurol. 2007;61:109–19.
Marsh E, Fulp C, Gomez E, Nasrallah I, Minarcik J, Sudi J, et al. Targeted loss of Arx results in a developmental epilepsy mouse model and recapitulates the human phenotype in heterozygous females. Brain. 2009;132:1563–76.
Osborne JP, Lux AL, Edwards SW, Hancock E, Johnson AL, Kennedy CRC, et al. The underlying etiology of infantile spasms (West syndrome): information from the United Kingdom Infantile Spams Study (UKISS) on contemporary causes and their classification. Epilepsia. 2010;51:2168–74.
Wirrell EC, Shellhaas RA, Joshi C, Keator C, Kumar S, Mitchell WG, et al. How should children with West syndrome be efficiently and accurately investigated? Results from the National Infantile Spasms Consortium. Epilepsia. 2015;56:617–25.
Kato M, Das S, Petras K, Sawaishi Y, Dobyns WB. Polyalanine expansion of ARX associated with cryptogenic West syndrome. Neurology. 2003;61:267–76.
Wallerstein R, Sugalski R, Cohn L, Jawetz R, Friez M. Expansion of the ARX spectrum. Clin Neurol Neurosurg. 2008;110:631–4.
Shields WD. Infantile spasms: little seizures. BIG consequences. Epilepsy Curr. 2006;6:63–9.
Go CY, Mackay MT, Weiss SK, Stephens D, Adams-Webber T, Ashwal S, et al. Evidenced-based guideline update: medical treatment of infantile spasms. Report of the Guideline Development Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2012;78:1974–80.
Marshall CR, Young EJ, Pani AM, Freckmann ML, Lacassie Y, Howald C, et al. Infantile spasms is associated with deletion of the MAGI2 gene on chromosome 7q11.23-q21.11. Am J Hum Genet. 2008;83:106–11.
Sanmaneechai O, Sogawa Y, Silver W, Ballaban-Gil K, Moshè SL, Shinnar S. Treatment outcomes of West syndrome in infants with Down syndrome. Pediatr Neurol. 2013;48:42–7.
Alrifai MT, AlShaya MA, Abulaban A, Alfadhel M. Hereditary neurometabolic causes of infantile spasms in 80 children presenting to a tertiary care center. Pediatr Neurol. 2014;51:390–7.
Auvin S, Hartman AL, Desnous B, Moreau AC, Alberti C, Delanoe C, et al. Diagnosis delay in West syndrome: misdiagnosis and consequences. Eur J Pediatr. 2012;171:1695–701.
Nelson GR. Management of infantile spasms. Transl Pediatr. 2015;4(4):260–70.
Shumiloff NA, Man Lam W, Manasco KB. Adrenocorticotropic hormone for the treatment of West syndrome in children. Ann Pharmacother. 2013;47:744–54.
Klein R, Livingston S. The effect of adrenocorticotrophic hormone in epilepsy. J Pediatr. 1950;37:733–42.
Sorel L, Dusaucy-Bauloye A. A propos de cas d’hypsarythmia de Gibbs: son traitment spectulaire per l’ACTH. Acta Neurol Belg. 1958;58:130–41.
Stafstrom CE, Arnason BG, Baram TZ, Catania A, Cortez MA, Glauser TA, et al. Treatment of infantile spasms: emerging insights from clinical and basic science perspectives. J Child Neurol. 2011;26:1411–21.
Baram TZ, Mitchell WG, Tournay A, Snead OC, Hanson RA, Horton EJ. High-dose corticotropin (ACTH) versus prednisone for infantile spasms: a prospective, randomized, blinded study. Pediatrics. 1996;97:375–9.
Mytinger JR, Weber A, Heyer GL. The response to ACTH is determined early in the treatment of infantile spasms. Epileptic Disord. 2015;17:52–7.
Ito M, Aiba H, Hashimoto K, Kuroki S, Tomiwa K, Okuno T, et al. Low-dose ACTH therapy for West syndrome: initial effects and long-term outcome. Neurology. 2002;58:110–4.
Kondo Y, Okumura A, Watanabe K, Negoro T, Kato T, Kubota T, et al. Comparison of two low dose ACTH therapies for West syndrome: their efficacy and side effect. Brain Dev. 2005;27:326–30.
Oguni H, Yanagaki S, Hayashi K, Imai K, Funatsuka M, Kishi T, et al. Extremely low-dose ACTH step-up protocol for west syndrome: maximum therapeutic effect with minimal side effects. Brain Dev. 2006;28:8–13.
Yanagaki S, Oguni H, Hayashi K, Imai K, Funatuka M, Tanaka T, et al. A comparative study of high-dose and low-dose ACTH therapy for West syndrome. Brain Dev. 1999;21:461–7.
Hrachovy RA, Frost JD Jr, Glaze DG. High-dose, long-duration versus low-dose, short duration corticotropin therapy for infantile spasms. J Pediatr. 1994;124:803–6.
Hamano SI, Yamashita S, Tanaka M, Yoshinari S, Minamitani M, Eto Y. Therapeutic efficacy and adverse effects of adrenocorticotropic hormone therapy in West syndrome: differences in dosage of adrenocorticotropic hormone, onset of age, and cause. J Pediatr. 2006;148:485–8.
Faulkner MA, Tolman JA. Safety and efficacy of vigabatrin for the treatment of infantile spasms. J Cent Nerv Syst Dis. 2011;3:199–207.
Appleton RE, Peters AC, Mumford JP, Shaw DE. Randomised, placebo-controlled study of vigabatrin as first-line treatment of infantile spasms. Epilepsia. 1999;40:1627–33.
Elterman RD, Shields WD, Bittman RM, Torri SA, Sagar SM, Collins SD. Vigabatrin for the treatment of infantile spasms: final report of randomized trial. J Child Neurol. 2010;25:1340–7.
Vigevano F, Cilio MR. Vigabatrin versus ACTH as first-line treatment for infantile spasms: a randomized, prospective study. Epilepsia. 1997;38:1270–4.
Chiron C, Dumas C, Jambaque I, Mumford J, Dulac O. Randomized trial comparing vigabatrin and hydrocortisone in infantile spasms due to tuberous sclerosis. Epilepsy Res. 1997;26:389–95.
Pesaturo KA, Spooner LM, Belliveau P. Vigabatrin for infantile spasms. Pharmacotherapy. 2011;31:298–311.
Willmore LJ, Abelson MB, Ben-Menachem E, Pellock JM, Shields WD. Vigabatrin: 2008 update. Epilepsia. 2009;50:163–73.
Lerner JT, Salomon N, Sankar R. Clinical profile of vigabatrin as monotherapy for treatment of infantile spasms. Neuropsychiatr Dis Treat. 2010;6:731–40.
Agrawal S, Mayer DL, Hansen RM, Fulton AB. Visual fields in young children treated with vigabatrin. Optom Vis Sci. 2009;86:767–73.
Conway M, Cubbidge RP, Hosking SL. Visual field severity indices demonstrate dose-dependent visual lossrom vigabatrin therapy. Epilepsia. 2008;49:108–16.
Durbin S, Mirabella G, Buncic JR, Westall CA. Reduced grating acuity associated with retinal toxicity in children with infantile spasms on vigabatrin therapy. Invest Ophthalmol Vis Sci. 2009;50:4011–6.
Maguire MJ, Hemming K, Wild JM, Hutton JL, Marson AG. Prevalence of visual field loss following exposure to vigabatrin therapy: a systematic review. Epilepsia. 2010;51:2423–31.
Westall CA, Wright T, Cortese F, Kumarappah A, Snead OC, Buncic JR. Vigabatrin retinal toxicity in children with infantile spasms: an observational cohort study. Neurology. 2014;83:2262–8.
Gaily E, Jonsson H, Lappi M. Visual field defects at school-age in children treated with vigabatrin in infancy. Epilepsia. 2009;50:206–16.
Riikonen R, Rener-Primec Z, Carmant L, Dorofeeva M, Hollody K, Szabo I, et al. Does Vigabatrin treatment for infantile spasms cause visual field defects? An international multicentre study. Dev Med Child Neurol. 2015;57:60–7.
Pearl PL, Vezina LG, Saneta RP, McCarter R, Molloy-Wells E, Heffron A, et al. Cerebral MRI abnormalities associated with vigabatrin therapy. Epilepsia. 2009;50:184–94.
Wheless JW, Carmant L, Bebin M, Conry JA, Chiron C, Elterman RD. Magnetic resonance imaging abnormalities associated with vigabatrin in patients with epilepsy. Epilepsia. 2009;50:195–205.
Lux AL, Edwards SW, Hancock E, Johnson AL, Kennedy CR, Newton RW, et al. The United Kingdom Infantile Spasms Study comparing vigabatrin with prednisolone or tetracosactide at 14 days: a multicentre, randomised controlled trial. Lancet. 2004;364:1773–8.
Lux AL, Edwards SW, Hancock E, Johnson AL, Kennedy CR, Newton RW, et al. The United Kingdom Infantile Spasms Study (UKISS) comparing hormone treatment with vigabatrin on developmental and epilepsy outcomes to age 14 months: a multicentre randomised trial. Lancet Neurol. 2005;4:712–7.
Knupp KG, Coryell J, Nickels KC, Ryan N, Leister E, Loddenkemper T, et al. Response to treatment in a prospective National Infantile Spasms cohort. Ann Neurol. 2016;79:475–84.
O’Callaghan FJK, Edwards SW, Alber FD, Hancock E, Johnson AL, Kennedy CR, et al. Safety and effectiveness of hormonal treatment versus hormonal treatment with vigabatrin for infantile spasms (ICISS): a randomised, multicentre, open-label trial. Lancet Neurol. 2017;16:33–42.
Wanigasinghe J, Arambepola C, Ranganathan SS, Sumanasena S, Muhandiram EC. The efficacy of moderate-to-high dose oral prednisolone versus low-to-moderate dose intramuscular corticotropin for improvement of hypsarrhythmia in West syndrome: a randomized, single-blind, parallel clinical trial. Pediatr Neurol. 2014;51:24–30.
Wanigasinghe J, Arambepola C, Ranganathan SS, Sumanasena S, Attanapola G. Randomized, single-blind, parallel clinical trial on efficacy of oral prednisolone versus intramuscular corticotropin on immediate and continued spasm control in West syndrome. Pediatr Neurol. 2015;53:193–9.
Darke K, Edwards SW, Hancock E, Johnson AL, Kennedy CR, Lux AL, Newton RW, O’Callaghan FJ, Verity CM, Osborne JP, Trial steering committee on behalf of participating investigators. Developmental and epilepsy outcomes at age 4 years in the UKISS trial comparing hormonal treatments to vigabatrin for infantile spasms: a multi-centre randomised trial. Arch Dis Child. 2010;95:382–6.
Karvelas G, Lortie A, Scantlebury MH, Duy PT, Cossette P, Carmant L. A retrospective study on aetiology based outcome of infantile spasms. Seizure. 2009;18:197–201.
Widjaja E, Go C, McCoy B, Snead OC. Neurodevelopmental outcome of infantile spasms: a systematic review and meta-analysis. Epilepsy Res. 2015;109:155–62.
Kivity S, Lerman P, Ariel B, Danziger Y, Mimouni M, Shinnar S. Long-term cognitive outcomes of a cohort of children with cryptogenic infantile spasms treated with high-dose adrenocorticotropic hormone. Epilepsia. 2004;45:255–62.
Primec Z, Stare J, Neubauer D. The risk of lower outcome in infantile spasms increases after three weeks of hypsarrhythmia duration. Epilepsia. 2006;47:2202–5.
Cohen-Sadan S, Kramer U, Ben-Zeev B, Lahat E, Sahar E, Nevo Y, Eidlitz T, Zeharia A, Kivity S, Goldberg-Stern H. Multicenter long-term follow-up of children with idiopathic West syndrome: aCTH versus vigabatrin. Eur J Neurol. 2009;16:482–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors have no conflicts of interest to declare.
Funding
This review was supported by an unrestricted grant from the World Association of Infectious Diseases and Immunological Disorders (WAidid).
Rights and permissions
About this article

Cite this article
D’Alonzo, R., Rigante, D., Mencaroni, E. et al. West Syndrome: A Review and Guide for Paediatricians. Clin Drug Investig 38, 113–124 (2018). https://doi.org/10.1007/s40261-017-0595-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-017-0595-z