
Abstract
This study aims to explore the effects of a 1-week inpatient course including information, physical activity (PA), and group sessions on physical and mental health-related outcomes for prostate cancer (PCa) patients. Further to assess the patients’ satisfaction with the course. PCa patients completed a questionnaire assessing PA, fatigue, mental distress, and quality of life 1 month before (T0) and 3 months after (T1) the course. Total fatigue, physical fatigue, and PSA anxiety decreased significantly from T0 to T1. No significant changes were observed in the other measures. The majority of the participants were satisfied with the course. In spite of minor reductions in fatigue and PSA anxiety and satisfied patients, the findings indicate that a 1-week inpatient course does not influence substantially on most of the health-related outcomes in PCa patients 3 months after the course.
Similar content being viewed by others


Introduction
Prostate cancer (PCa) is the most frequent malignancy among men and mostly affecting men at older age [1]. Surgery, radiation therapy, or androgen-suppressive treatment are the most commonly used treatment modalities [2]. The 5-year survival rate of PCa is high and has increased over the past years probably due to earlier diagnosis and improved treatment [1]. However, many PCa survivors experience late effects caused by the disease and/or the treatment like decreased physical function, increased body fat mass [3], impairment of bladder, bowel, or sexual function [4], fatigue, depression, and reduced quality of life (QoL) [5].
On this background, information on the late effects after treatment for PCa and how to deal with them becomes highly relevant. Information can be downloaded from internet sites or be presented in written forms. The information can also be conveyed by courses such as those organized by cancer organizations. In Norway, hospitals by law are obliged to have ‘teaching and coping’ centers providing information and social contact among different groups of patients. In these courses, the participants stay at home and participate in, i.e., bi-weekly sessions at the centers. The effects of all these efforts are sparsely documented, and knowledge about the potential effects is paramount in order to establish effective and supportive interventions. In addition to the information per se, communication with other PCa survivors can also reduce psychosocial distress and enhance coping [6].
In 1990, The Norwegian Radium Hospital (NRH), a comprehensive cancer center, opened a national center [The Montebello Center (MBC)] for cancer survivors and their families. Cancer patients from all over Norway can be referred to MBC [7]. The center offers cancer patients and their spouses/relatives intensive courses of 5–10 days duration while staying at the institution with the aim to improve the patients’ coping with the disease and the side-effects of their treatment. Patients with similar diagnosis attend diagnosis-specific courses, while the basic structure of the content of the courses is quite similar across the courses including lectures, physical activity (PA), group sessions, and social gatherings. Reviewing 15 years of operation at the MBC, 10,173 cancer patients from all over Norway have participated in these courses with breast cancer patients represented the largest group. The proportion of men has increased over time. Most patients attended a course less than 2 years after diagnosis. Immediately after the courses, the majority (90%) of the patients was highly satisfied with the courses, reported increased knowledge about their cancer, and had better coping with their disease [7]. However, the effects of the courses in terms of improved health have not been assessed until now.
The objectives of the present study were to explore the effects of PCa-specific courses on: PA, fatigue, mental distress, and Global QoL assessed prior to the course and 3 months thereafter. Our secondary objective was to assess the patients’ satisfaction with the courses.
Material and Methods
Participants
To participate in one of the PCa-specific courses, three inclusion criteria had to be fulfilled by the participants: (1) having PCa; (2) being referred by a physician confirming a ‘need for the course’; and (3) being self-reliant. One month before the start of the course (T0), patients were invited to participate in the questionnaire-based study. An invitation letter and a questionnaire were sent by mail. Those who completed the first questionnaire received a second questionnaire 3 months after the course (T1). No reminder was sent to those were not responding at T0.
The Intervention
Each course was conducted by a multidisciplinary team, lasted for 6 days, and consisted of lectures, PA, and group sessions. The lectures covered different topics. An oncologist presented basic medical facts concerning PCa, treatment modalities, and late effects. A social worker and a physiotherapist/sport instructor informed about social benefits and the expected effects of PA, respectively. Lectures about sexuality/partnership and urinary problems were given by a sexual therapist and a cancer nurse. Finally, factual information about mental distress after PCa was presented by a psychologist or psychiatrist.
PA was performed in groups of 6–9 participants two times per day and was led by a physiotherapist or a sport instructor. PA included water gymnastic, walking, Nordic walking, resistance training, pelvic floor training, stretching, and relaxation. The length of the sessions varied from 30 to 90 min. The participants rated their subjectively experienced exertion rating after every session, with the alternatives: very mild, mild, moderate, strenuous, and very strenuous. Overall, the activities were done with moderate intensity.
The participants met 1 hour daily for a group session which was led by a nurse experienced in group counseling. The themes of the sessions were related to the content of the lectures, and the purpose was to discuss the themes in relation to the participants’ personal experiences with PCa.
The total active hours of the program were approximately 30 h. The lectures amounted to about 45% of total active hours of the course, the PA to approximately 35%, and the group sessions to roughly 20%. The spouses took part in the lectures and PA, while they had group sessions separately. The effects of the course on the spouses were not part of the study.
The participants could also make appointments for individual consultations with the professionals who gave the lectures. Additionally, social and cultural activities were a large part of the course evenings.
Measurements
Demographic and medical variables were self reported at baseline including: present age, marital status, level of education, employment status, time since diagnosis, physical comorbidity (cardiovascular diseases, diabetes, asthma, or allergy), and treatment. PA level was assessed by a modified version of the Leisure Score Index from The Godin Leisure Time Exercise Questionnaire (GLTEQ) [8]. The GLTEQ consists of three questions concerning mean frequency and duration of mild (minimal effort, no perspiration), moderate (not exhausting, light perspiration), and strenuous (heart beats rapidly, sweating) exercise in leisure time during an average week. The GLTEQ has been found to be both valid and reliable [9]. The GLTEQ was translated into Norwegian by two independent translators following standard forward and backward translation procedures [10]. The total minutes of moderate and strenuous exercise were calculated and the proportion of respondents meeting public health exercise guidelines (≥150 min of moderate-to-strenuous intensity or ≥75 min of strenuous intensity per week) [11] was registered.
Fatigue was assessed by The Fatigue Questionnaire (FQ) [12].The FQ consists of 11 items, seven cover physical fatigue (PF), and four cover mental fatigue (MF) experienced during the last month. The sum of PF and MF constitutes total fatigue (TF). The responses are scored on a four-point Likert scale from 0 to 3 and higher scores imply more fatigue, and the range of scores for the whole scale is 0–33 (PF 0–21 and MF 0–12) [12]. The FQ has robust psychometric properties [13].
The Memorial Anxiety Scale for Prostate Cancer (MAX-PC) [14] consists of three subscales: general PC anxiety (11 items), anxiety related to prostate-specific antigen (PSA) levels (three items), and fear of recurrence (four items). Responses are scored on a four-point Likert scale from 0 to 3, and higher scores imply more cancer-related anxiety. The range of scores on the subscales is 0 to 33, 0 to 9, and 0 to 12, respectively. The scores on the three subscales are added in order to get the total MAX-PC score, which ranges from 0 to 54. The MAX-PC has shown to have an acceptable validity and reliability [14].
The Hospital Anxiety and Depression Scale (HADS) [15]. The HADS consists of two subscales with seven items on depression (HADS-D) and seven on anxiety. Each item is scored on a 0 to 3 Likert scale, and a higher score implies higher level of anxiety/depression. The HADS total score is the sum of the items scores on both subscales. The range of scores is 0 to 21 for each subscale. The psychometric properties of HADS are reported as good [16].
QoL was assessed by the two items constituting the Global QoL-Scale in The European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire C30 (EORTC QLQ-C30) [17]. The range of transformed scores is to 0–100. A higher score represents better QoL. The Norwegian version of the EORTC-QLQ C30 has shown good reliability and validity [18].
Satisfaction with the course was evaluated by two questions specially developed for this study in order to cover two aspects of satisfaction (response alternatives within a parenthesis): (1) ‘Did the course change your expectations towards everyday life?’ (to a high extent, to a fair extent, only partially, not at all) and (2) ‘Did the course help you to cope better with your prostate cancer and/or the side-effects associated with the treatment?’ (to a high extent, to a fair extent, only partially, not at all).
Statistical Analysis
The statistics were performed in the Statistical Package of Social Science 15.0 (Windows, Chicago, IL). Standard descriptive statistics were used to analyze differences between the completers and non-completers. Changes from T0 to T1 were examined with paired sample t test for continuous data and with McNemar’s test for categorical data. All tests were two-sided, and the level of significance was set at p < 0.05.
Ethics
The institutional review board at the MBC and the NRH and the Regional Ethics Committee for Medical Research Region South-East Norway approved the study. All the patients who participated in the study gave their consent to take part in the evaluation.
Results
Participation
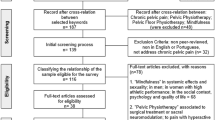
Seventy-five men who signed up for a course for PCa patients at MBC in October 2006 (n = 29), December 2006 (n = 23), and February 2007 (n = 23) were invited to participate. Of the men invited, 67 (89%) were willing to participate and returned the questionnaire at T0. At T1, 51 men returned the questionnaire (participation rate 68%). Compared to those who responded at both time points, those who only responded at T0 had higher level of depression (HADS-D) (p = 0.04) and a higher level of total fatigue (p = 0.05) (Table 1).
Characteristics at T0
The median age of the completers (n = 51) was 67.4 years (48.5–81.2) and 86% was married or cohabiting (Table 1). According to the self report, 53% had completed college or university, 51% were retired, and 23% worked full-time or part-time. The median time since diagnosis was 18.2 months (3.0–97.0), and 23% reported physical comorbidities. Forty-three percent had undergone surgery ± radiotherapy, 20% had received radiotherapy, 16% had received hormone therapy, 8% had ‘wait and see’, and 14% had received hormone therapy + other therapies. Eighty-six percent had localized or pelvis-confirmed advanced disease and 14% had metastatic PCa.
Changes in PA, Fatigue, Mental Distress, and QoL
The proportion of men meeting public exercise guidelines did not change significantly from T0 to T1 (Table 2). The mean of total fatigue was significantly reduced from 16.1 (4.8) at T0 to 14.0 (4.4) at T1 (p = 0.001), and physical fatigue decreased from 11.1 (4.0) at T0 to 9.2 (3.4) at T1 (p = 0.001). The reduction in mental fatigue did not reach statistical significance. Of the MAX-PC subscales, the mean level of PSA anxiety was reduced from 0.8 (1.3) at T0 to 0.3 (0.9) at T1 (p = 0.001), while the remaining MAX-PC subscales did not change significantly. The mean scores of HADS and Global QoL did not change significantly.
Satisfaction with the Course
Concerning satisfaction with the course, the respondents provided the following ratings at T1: 56% stated that the course had changed their everyday life expectations (to a high extent/fair extent) and 60% reported that the course had helped them to cope better with their PC and/or the side-effects associated with the treatment (to a high extent/fair extent) (data not shown).
Discussion
This explorative study on the effects of a 1-week course showed that the levels of total and physical fatigue were significantly reduced from T0 to T1. A significant reduction in the PSA anxiety subscale was also found, while no significant changes were observed concerning the general PCa anxiety and fear of recurrence subscales. The course did not significantly change the levels of PA, anxiety/depression, or Global QoL. The majority of the respondents stated that the course had helped them to meet everyday’s requirements.
During the 1990s, institutions similar to MBC were established in Sweden (e.g., Lydiagården) and Denmark (e.g., Dallund) based on the assumption that PA, lectures, and group sessions were important elements in the rehabilitation of cancer patients. PA seems to have promising effects in PCa patients resulting in improved muscular fitness, physical function, QoL, and reduced fatigue [19]. General informational and educational programs for cancer patients have been found to have beneficial effects on emotional and functional adjustment, and treatment- and disease-related symptoms [20]. Group sessions focusing on sharing of experiences based on the importance of support from fellow patients have shown to improve coping in cancer patients [6, 20]. Such effects could not be detected in the present sample. This implies that the intervention could be ‘too weak’ or the sample did not fit the intervention.
Overall, in spite of some positive results such as reduction in fatigue and PSA anxiety, the 3-month effect of MBC’s prostate cancer-specific courses must be considered as negative. Similarly, Jorgensen et al. did not find any changes in QoL and mental distress at 1- and 6-months follow-up of Danish breast cancer patients attending a 1-week similar intervention at Dallund that was also compared to a control group. Jorgensen et al. suggest that the intervention could have been useful if the patients had attended the program closer to the end of treatment [21]. Courses starting as long as 2 years after the end of treatment may have limited effects due to the patients’ capacity for improvement actually are limited (a ceiling effect). This could also be the case in our study, since half of our sample was participating more than 1.5 years after diagnosis, when their health condition probably is relatively stable.
Our findings are in contrast to a Dutch randomized study comparing groups getting PA and PA + cognitive-behavioral training compared to a control group in a 12-week outpatient program starting ≥3 months (average 1.3 years) after treatment. That study found an improved QoL in both intervention groups immediately after the intervention and at 3- and 9-month follow-up [22, 23]. Interestingly, the participants in that study should have three or more physical or psychological complaints in order to be included, thereby documenting morbidity and thus avoiding a major ceiling effect. The MBC PCa courses did not use such an inclusion criterion. This interpretation is supported by the fact that the mean Global QoL score at T0 was approximately 10 points higher than in the abovementioned Dutch sample [23].
The ceiling effect and the patients’ potential for improvement are issues to consider in future studies of information/exercise and rehabilitation programs. Heterogeneity of the study sample as to age and treatment is another issue to be considered in relation to rehabilitation of cancer patients. For example, the rehabilitation needs among young professionally active men who have undergone curative treatment of localized prostate cancer probably differ from the needs of older men with life-long androgen-suppressive therapy due to metastatic disease. Unselected inclusion of cancer patients will easily reduce the chance of improvement. Another strategy could be to include only those who report specific problems or in other ways have reduced health and thereby aiming the intervention group more homogeneous. The duration of the interventions might also be of importance since the intervention tested by May et al. [23] lasted for 12 weeks (once to twice weekly) compared to our intensive 1-week course.
In line with May et al. [23], we found a positive effect on fatigue. Due to the lack of a control group in our study, we cannot state whether the positive changes in fatigue at T1 are due to the course. The significant improvements observed could be due to ‘regression toward the mean’ rather than the intervention. The statistically documented improvement at T1 could in line with this, represents a spontaneous transition to their habitual level of fatigue [24]. On the other hand, fatigue was a central topic in the lectures which in combination with the PA could have influenced upon both the participants’ cognition and level of activity and thus contributed to the reduced level of fatigue. The lack of a control group limits further elaboration on this point.
We believe the improvement in PSA anxiety is related to the information on this particular issue presented in the lectures and discussed in the group sessions. Factual knowledge about PSA’s significance for the clinical course of PCa is of relevance and will presumably reduce anxiety about PSA tests results.
At several places in Europe, both outpatient- and inpatient-based programs, including information, PA, and group sessions, for cancer patients with different duration are currently running. So far, there is no conclusive evidence that longer programs are more beneficial than short ones. Further, the effects of an inpatient 1-week program like ours as compared to less intensive programs administered over weeks while the patients stay at home are unknown. Factors like employment status, family situation, social network, health status, and specific problems will probably determine the patients’ preference for the type of program. For example, PA might have better effects in a program lasting for several weeks while information and group sessions might be more efficiently administered in an intensive program outside the routines of daily life. We believe that a follow-up or a booster procedure on PA and perhaps other elements could be relevant supplements to the 1-week course. Probably a 1-week course alone is too short to influence the patients’ exercise behavior over time. It is therefore reasonable to speculate that a follow-up course would increase the chance to obtain positive results. Also, the use of objective measurements of PA or physical performance would improve the program.
Behavior change is a complex process and there are several levels in motivation for changes. A well-known model is ‘the transtheoretical model’ [25] with five stages of change and it can be used in a variety of behaviors. Most probably, the PCa patients in the present study were in different motivation stages in terms of their wishes/desires to change their exercise behaviors. For future studies in the field, it would be interesting to include the model, so even if the participants did not change their level of PA, it would be possible to see if they had changed in stage to become an exerciser.
There are some major limitations of the present study. The heterogeneity of the sample in terms of a relatively wide span between the participants’ health status is related to referral patterns of the MBC. These could not be changed when the study was designed. The relatively high mean scores on the outcome variables at T0 limit the possibility to improve and detect improvements of the participants’ health. The lack of a control group is another limitation specifically affecting the implications of the finding of a lowered fatigue level at T1. Since the study was based upon a convenience sample, further elaboration on this point is not possible except stating that a control group is needed in order to verify such an effect of the course on fatigue.
In conclusion, the intensive 1-week inpatient course was followed by minor reductions in fatigue and PSA anxiety and satisfied patients. Still, the overall findings indicate that an intensive 1-week course does not influence substantially on most of the health-related outcomes in PCa patients after 3 months. Controlled trials directed towards a more homogenous group of patients with anticipated recovery capacity are needed for documentation of efficacy rehabilitation efforts among cancer patients.
References
Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, Altekruse SF, Feuer EJ, Huang L et.al. (2009) SEER Cancer Statistics Review. National Cancer Institute. http://seer.cancer.gov/csr/1975_2006/. Accessed 25 October 2009
Heidenreich A, Aus G, Bolla M, Joniau S, Matveev V, Schmid H-P, Zattoni F (2007) Guidelines on prostate cancer. European Association of Urology. Type ref: report
Galvao DA, Taaffe DR, Spry N, Joseph D, Turner D, Newton RU (2009) Reduced muscle strength and functional performance in men with prostate cancer undergoing androgen suppression: a comprehensive cross-sectional investigation. Prostate Cancer Prostatic Dis 12:198–203
Potosky AL, Davis WW, Hoffman RM, Stanford JL, Stephenson RA, Penson DF, Harlan LC (2004) Five-year outcomes after prostatectomy or radiotherapy for prostate cancer: the prostate cancer outcomes study. J Natl Cancer Inst 96:1358–1367
Roth AJ, Weinberger MI, Nelson CJ (2008) Prostate cancer: psychosocial implications and management. Future Oncol 4:561–568
Gregoire I, Kalogeropoulos D, Corcos J (1997) The effectiveness of a professionally led support group for men with prostate cancer. Urol Nurs 17:58–66
Fossa SD, Kvaloy J, Kvaloy S, Loge JH, Dahl AA (2008) [Courses for cancer patients-15 years' experience at The Montebello Centre in Norway]. Tidsskr Nor Laegeforen 128:2554–2557
Godin G, Jobin J, Bouillon J (1986) Assessment of leisure time exercise behavior by self-report: a concurrent validity study. Can J Public Health 77:359–362
Jacobs DR, Ainsworth BE, Hartman TJ, Leon AS (1993) A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc 25:81–91
Guillemin F, Bombardier C, Beaton D (1993) Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 46:1417–1432
US Department of Health and Human Services (2008) 2008 Physical Activity Guidelines for Americans. Be active, healthy, and happy! Ref type: report
Chalder T, Berelowitz G, Pawlikowska T, Watts L, Wessely S, Wright D, Wallace EP (1993) Development of a fatigue scale. J Psychosom Res 37:147–153
Minton O, Stone P (2009) A systematic review of the scales used for the measurement of cancer-related fatigue (CRF). Ann Oncol 20:17–25
Roth AJ, Rosenfeld B, Kornblith AB, Gibson C, Scher HI, Curley-Smart T, Holland JC, Breitbart W (2003) The memorial anxiety scale for prostate cancer: validation of a new scale to measure anxiety in men with prostate cancer. Cancer 97:2910–2918
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67:361–370
Bjelland I, Dahl AA, Haug TT, Neckelmann D (2002) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 52:69–77
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376
Hjermstad MJ, Fossa SD, Bjordal K, Kaasa S (1995) Test/retest study of the European Organization for Research and Treatment of Cancer Core Quality-of-Life Questionnaire. J Clin Oncol 13:1249–1254
Thorsen L, Courneya KS, Stevinson C, Fossa SD (2008) A systematic review of physical activity in prostate cancer survivors: outcomes, prevalence, and determinants. Support Care Cancer 16:987–997
Meyer TJ, Mark MM (1995) Effects of psychosocial interventions with adult cancer patients: a meta-analysis of randomized experiments. Health Psychol 14:101–108
Jorgensen IL, Frederiksen K, Boesen E, Elsass P, Johansen C (2009) An exploratory study of associations between illness perceptions and adjustment and changes after psychosocial rehabilitation in survivors of breast cancer. Acta Oncol 48:1119–1127
Korstjens I, May AM, van Weert E, Mesters I, Tan F, Ros WJ, Hoekstra-Weebers JE, van der Schans CP, van den Borne B (2008) Quality of life after self-management cancer rehabilitation: a randomized controlled trial comparing physical and cognitive-behavioral training versus physical training. Psychosom Med 70:422–429
May AM, Korstjens I, van Weert E, van den Borne B, Hoekstra-Weebers JE, van der Schans CP, Mesters I, Passchier J, Grobbee DE, Ros WJ (2009) Long-term effects on cancer survivors' quality of life of physical training versus physical training combined with cognitive-behavioral therapy: results from a randomized trial. Support Care Cancer 17:653–663
Chernick MR, Friis RH (2003) Introductory biostatistics for the health sciences. Modern applications including bootstrap. Wiley, Hoboken
Prochaska JO, DiClemente CC (1983) Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol 51:390–395
Acknowledgment
This study was supported by The Norwegian Radium Hospital Foundation and Trivselsanleggets Foundation, Department of Cancer Rehabilitation, The Norwegian Radium Hospital, and Anette and Brynjulf Skaugen Charitable Foundation. The authors wish to acknowledge the work and collaboration of the staff of the Montebello Center of Norway.
Conflicts of Interest
We state that there are no potential conflicts of interest in this study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Gjerset, G.M., Fosså, S.D., Dahl, A.A. et al. Effects of a 1-Week Inpatient Course Including Information, Physical Activity, and Group Sessions for Prostate Cancer Patients. J Canc Educ 26, 754–760 (2011). https://doi.org/10.1007/s13187-011-0245-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13187-011-0245-8