
Abstract
Background
In youth with inflammatory bowel disease (IBD), health-related quality of life (HRQOL) has been shown to be affected by individual disease factors and specific psychological factors. The innovative aim of this study is to examine the combined impact of psychological factors (illness perceptions, cognitive coping, anxiety, and depression) on HRQOL, over and above the associations of demographic and disease factors with HRQOL in youth with IBD.
Method
Data on clinical disease activity, illness perceptions, cognitive coping, anxiety, depression, and HRQOL were prospectively collected in 262 consecutive youth (age 10–20, 46.6% male) with confirmed IBD. Multiple linear regression analyses tested the associations of demographic, disease, and psychological variables with HRQOL in separate groups for Crohn’s disease (CD; N = 147) and ulcerative colitis and IBD unclassified (UC/IBD-U; N = 115), using age-specific validated instruments.
Results
In both disease groups, more negative illness perceptions (ß = − .412; ß = − .438, p < .001) and more depression (ß = − .454; ß = − .279, p < .001) were related to lower HRQOL. In the UC/IBD-U group, more anxiety was related to lower HRQOL (ß = − .201, p = .001). The model with the psychological variables explained a large and significant amount of variance in both groups: 74% and 83%, respectively (p < .001).
Conclusion
In 10–20-year-old IBD patients, negative illness perceptions and depression were significantly and more strongly associated with lower HRQOL than demographic and disease factors. Thus, it is important to integrate psychological factors in the treatment for IBD patients. To improve HRQOL in young IBD patients, psychological interventions should be targeted at negative illness perceptions and depression.
Similar content being viewed by others

Introduction
Inflammatory bowel disease (IBD) is a disabling chronic gastrointestinal condition, with two predominant subtypes: Crohn’s disease (CD) and ulcerative colitis (UC). In up to 25% of patients, IBD starts in late childhood or adolescence [1,2,3]. The designation IBD unclassified (IBD-U) is used for patients in which it is not (yet) possible to make a distinction between CD and UC. IBD is characterized by periods of clinical disease activity and remission and presents with symptoms such as abdominal pain, bloody diarrhea, fatigue, and weight loss [4]. In adolescence, growth failure and delayed pubertal development is common, specifically in Crohn’s disease. The adolescent life phase is characterized by development on several domains (biological, psychological, social, cognitive, academic). Having a chronic disease such as IBD can affect all these domains, for example, not only becoming more independent from parents, developing long-term friendships, starting secondary education, forming an own identity, but also experimenting with alcohol and drugs, seeking and finding a (side) job, and having romantic relationships. The teenage years are a crucial period of transition from childhood to young adulthood [5]. IBD and its medical treatment may severely impact psychosocial functioning: health-related quality of life (HRQOL) in children and adolescents (further referred to as youth) with IBD is significantly lower than in healthy peers [6, 7]. Furthermore, high prevalence rates varying from 20 to 50% for anxiety and depression are found in these patients [8,9,10,11]. A recent meta-analysis in children and adolescents showed pooled prevalence rates for anxiety and depressive symptoms of 15% and for anxiety and depressive disorders of 3–4% [12].
Other psychological factors are also important to consider in patients with IBD, such as illness perceptions and coping, because these have been shown to be related to psychosocial outcomes (such as HRQOL, general functioning or adjustment to IBD). Illness perceptions refer to the cognitive and emotional representations a patient forms about his or her disease [13]. These representations cover several dimensions, i.e., consequences (the expected effects of the disease), timeline (expectations about the duration of the disease), cause (thoughts about the cause of the disease), controllability (the extent to which the individual believes he or she can control the disease with or without treatment), identity (how the individual describes the symptoms and perceives as part of the disease), concern (worries about the disease), and emotions (the emotional response to the disease) [13, 14]. Coping refers to intentional efforts to regulate negative emotions in response to harm, threat, or challenges [15, 16] in this study dealing with IBD. Coping encompasses both cognitive and behavioral regulation. Cognitive coping is implicated in the etiology and the maintenance of anxiety and depression [17, 18] and is therefore important as well in studying youth with IBD.
The common sense model (CSM) is a model to describe the relationships between disease characteristics, illness perceptions, coping, and anxiety, depression, and HRQOL, originally developed by Leventhal and Diefenbach [13]. In this model, illness characteristics (such as clinical disease activity) lead to certain thoughts about the illness, the so-called illness perceptions of a patient. These illness perceptions influence the type of coping the patient uses to deal with his/her symptoms. Together, these factors lead to positive or negative illness outcomes, for example, anxiety, depression, or HRQOL. In patients with IBD, several relationships have been found between these variables, mostly in adults. Below it will be explicitly mentioned if studies were conducted in youth with IBD. For example, more clinical disease activity has been found to be associated with more anxiety and depression separately [19, 20]. Previous studies have also demonstrated a relationship between clinical disease activity and HRQOL, with a mediating role for anxiety and depressive symptoms [19, 21]. Furthermore, negative illness perceptions are associated with lower HRQOL in adults with IBD [22] and also with more psychological problems in youth with IBD [23]. Coping was associated with anxiety and depression [24] or adjustment to IBD [25] in adults and found as predictor of depression in youth with IBD as well [26].
Unfortunately, very little is known on how all the factors described above together affect health outcomes, more specifically HRQOL in young IBD patients. Only a few studies examined several psychological factors simultaneously. In adults, illness perceptions [27] and coping [24] have been reported to impact the relationship between clinical disease activity on HRQOL. Recently, Van Tilburg et al. [28] showed in adolescents with IBD that patient-reported disability (as outcome) was associated not only with clinical disease activity but also with a combined latent construct ‘psychological factors’ (including coping, pain beliefs, anxiety, and depression). However, they did not control for demographic factors (gender, age, socioeconomic status) and did not include other disease factors, such as disease type and disease duration. In addition, there is some evidence that these disease factors are associated with HRQOL [20, 29, 30] and with anxiety and/or depression as well [23, 31]. Moreover, because the authors used a combined psychological construct, their findings provide no insight on which psychological factors in particular psychological interventions for youth with IBD should focus.
The complex interplay between clinical disease activity, illness perceptions, coping, anxiety, and depression makes it challenging to attune both the medical and psychological treatment to the individual needs of IBD patients to improve their HRQOL. The surplus value of the present study in a cohort of youth with IBD is that it aims to clarify the association of a combination of psychological factors (illness perceptions, cognitive coping, anxiety, and depression) with HRQOL, over and above demographic and disease factors. By selecting the 10–20-year age range, we cover the period of transition from childhood to young adulthood. More specific insight on how psychological factors are associated with HRQOL in these vulnerable youth can offer guidance on which factors psychological interventions should focus. Ultimately, with tailored psychological interventions, the course of the IBD and of possible psychological problems may be positively affected. We hypothesize that clinical disease activity is negatively associated with HRQOL. Furthermore, we hypothesize that psychological factors (i.e., illness perceptions, cognitive coping, anxiety, and depression, when tested simultaneously) are associated with HRQOL, even after controlling for clinical disease activity and other demographic and disease factors.
Materials and Methods
Design
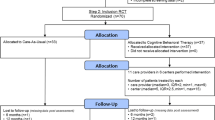
The present cross-sectional cohort study is based on a large patient sample (N = 374), completing the baseline assessment of a multicenter randomized controlled trial (RCT), investigating a disease-specific cognitive behavioral therapy in youth with IBD and symptoms of anxiety and/or depression (trial registration number: NCT02265588, see also Van den Brink and Stapersma et al. [32]). In the current study, only data from patients aged 10–20 years were used (N = 262).
Inclusion criteria were as follows: (1) age 10 to 20 years and (2) diagnosis of IBD, according to the consensus criteria [33] [34, 35].
Exclusion criteria were as follows: (1) intellectual disability; (2) current treatment for mental health problems (pharmacological and/or psychological); (3) insufficient mastery of the Dutch language; (4) a diagnosis of selective mutism, bipolar disorder, schizophrenia, autism spectrum disorder, obsessive-compulsive disorder, posttraumatic or acute stress-disorder, or substance use disorder; (5) cognitive behavioral therapy in the past year (at least eight sessions); and (6) participation in another intervention study.
Procedure
Consecutive patients and their parents were recruited between October 2014 and September 2016 from the outpatient clinic in two academic hospitals and four community hospitals in the Southwest region of the Netherlands. Patient information was given, and written informed consent was requested in all patients and, if applicable, their parents or caregivers. Patients (and parents), who consented to participate, received an e-mail with a link to online questionnaires. Clinical disease activity was scored by the (pediatric) gastroenterologist around the time of inclusion (i.e., within approximately a month around the time of inclusion, median = 3.42 weeks).
Measures
Control Variables
Gender, age, disease type, and disease duration of the patients were derived from their medical record. Socioeconomic status (SES) was determined using the occupational level from the parents or, if they lived on their own, patients themselves. Using the standard coding system of Statistics Netherlands ([36]), occupations were categorized in low, middle, and high. For gender and SES, dummy variables were created to use in the analyses.
Clinical disease activity was assessed by two validated clinical disease activity instruments. For CD, the short Pediatric Crohn’s Disease Activity Index (sPCDAI) and, for UC, the Pediatric Ulcerative Colitis Activity Index (PUCAI) were used. The sPCDAI comprises six items on medical history (abdominal pain, stools), well-being, physical examination (abdomen), weight, and extra-intestinal manifestations [37]. Scores range from 0 to 90 points [38]. The PUCAI comprises six items on abdominal pain, rectal bleeding, stool frequency and consistency, and activity level. Scores range from 0 to 85.
Psychological Factors
Illness perceptions were assessed by the Brief Illness Perceptions Questionnaire (B-IPQ; [14, 39]). This 9-item self-report questionnaire assesses cognitive and emotional representations of illness, covering eight dimensions: consequences, timeline, personal control, treatment control, identity, concern, emotions, and understanding. All dimensions are scored on an 11-point Likert-scale (0: not at all–10: very much/severely). A higher score represents more negative illness perceptions. Good test–retest reliability and concurrent validity have been found [14], and the B-IPQ has been used before in adolescents with IBD [40]. Internal consistency (Cronbach’s alpha) for the current sample was .81 in the CD group and .81 in the UC/IBD-U group.
Cognitive coping was measured with the Cognitive Emotion Regulation Questionnaire (CERQ). This self-report scale consists of 36 items, scored 1 to 5 points, with nine subscales (e.g., self-blame, acceptance, putting into perspective, positive refocusing, positive reappraisal, and catastrophizing). These scales are divided into two domains: adaptive cognitive coping (e.g., positive reappraisal, putting in perspective) and maladaptive cognitive coping (e.g., self-blame, catastrophizing). A higher score indicates more use of a particular coping style. Good reliability and construct validity have been found [41]. Both adaptive coping and maladaptive coping were used as variable in the analyses. For adaptive cognitive coping, internal consistency was .90 in the CD group and .93 in the UC/IBD-U group. For maladaptive cognitive coping, internal consistency was .88 in the CD group and .90 in the UC/IBD-U group.
Anxiety was assessed using the 69-item self-report questionnaire Screen for Child Anxiety Related Disorders (SCARED). The SCARED contains five subscales: general anxiety disorder, separation anxiety disorder, specific phobia, panic disorder, and social phobia, rated on a 3-point scale (0–2: total score 0–138). Satisfactory reliability and validity have been reported [42]. The cutoffs for elevated anxiety were total score ≥ 26 for boys, ≥ 30 for girls, or subscale score ≥ 8 [43]. These were only used to decide whether patients had elevated anxiety, i.e., could be included in the RCT. Internal consistency for the current sample was .95 in the CD group and .94 in the UC/IBD-U group.
Depression was assessed using the Child Depression Inventory (CDI, for ages 10–17) and the Beck Depression Inventory, second version (BDI-II, for ages 18–20). The CDI is a 27-item self-report scale (0–2, total score 0–54). Good reliability and validity have been established. A CDI score of 13 or higher reflected elevated depression [44]. The BDI-II is a 21-item self-report scale (0–3, total score 0–63). It has excellent reliability and good to excellent validity. A BDI-II score of 14 or higher reflected elevated symptoms of depression [45]. The cutoffs for the CDI and BDI-II were only used to decide whether patients had elevated depression, i.e., could be included in the RCT. For the CDI, internal consistency was .85 in the CD group and .86 in the UC/IBD-U group. For the BDI-II, internal consistency was .91 in the CD group and .84 in the UC/IBD-U group. To be able to combine patients of all ages within the disease groups, depression scores were created a Z-score for depression using either the CDI or the BDI-II (depending on age).
Health-related quality of life was assessed by the IBD-specific self-report IMPACT-III, which covers six domains: IBD-related symptoms, systemic symptoms, emotional functioning, social functioning, treatment related concerns, and body image [46]. The 35 items are scored (1–5; total score 35–175). Good psychometric properties have been found [47]. The total score was used, and a higher total score indicates better HRQOL. Although the IMPACT-III originally was designed for youth up to 18 years, we also used it for the patients of 19 and 20 years. This allowed us to combine all patients in to one group for each disease type. This was substantiated by excellent internal consistency in both disease groups: .93 in the CD group and .94 in the UC/IBD-U group.
Statistical Analyses
To test whether the associations of demographic, disease and psychological factors with HRQOL are different for CD than for UC/IBD-U, multiple linear regression analyses were performed for the two disease groups separately: CD (N = 147) and UC/IBD-U (N = 115). UC and IBD-U were combined, since the group with IBD-U patients was quite small (N = 18), IBD-U often resembles UC more than CD [48], and IBD-U has often a similar treatment approach as UC [49]. All variables were continuous, except for gender and SES. For these variables, dummy variables were included in the analyses. The abovementioned cutoffs for the SCARED, CDI, and BDI-II were only used to determine the proportion of patients with elevated anxiety or depressive symptoms. For the remaining questionnaires, no cutoffs were used.
The multiple linear regression analyses were run with two blocks/models, using HRQOL as outcome. In the first block, the demographic and disease variables (gender, age, disease duration, SES, and clinical disease activity) were entered simultaneously in the first regression model. In the second block, the psychological factors (illness perceptions, cognitive coping, anxiety, and depression) were added simultaneously to the variables entered in the first block. To account for missing values, multiple imputation with chained equations was applied using SPSS (m = 15 for approximately 15% of missing data; [50]). As a sensitivity analysis, we also performed a complete case analysis (N = 116; N = 104 for the CD and UC/IBD-U groups, respectively) to see whether the multiple imputations had an effect on the results. A p value of < .05 was considered significant. SPSS Version 24 was used for the analyses (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp). A statistician (JE) supported and advised in analyzing and interpreting the data and results.
Ethical Considerations
This study was performed conform the Declaration of Helsinki and approved by the Institutional Review Board of the Erasmus MC and of each participating center.
Results
Patient Characteristics
In total, 552 patients (aged 10–25 years) were invited for a randomized controlled trial (RCT) and 382 agreed to participate (response rate = 69%). Eight patients had incomplete data. From the final 374 youth, 262 were aged 10–20 years and were included in the current study. Demographic, disease, and psychological characteristics are presented in Table 1. In disease groups (CD and UC/IBD-U), the percentage of patients with active disease (mild-moderate-severe) was 31.3% and 30.4%, respectively. Overall, 50% of the patients had elevated anxiety, 17.9% had elevated depression, and 16.8% had both. For HRQOL, illness perceptions, and cognitive coping, no cutoffs are available; so means with ranges are provided in Table 1.
Influence of Demographic, Disease, and Psychological Variables on HRQOL; Results of Multiple Linear Regression Analyses per Disease Group
In Tables 2 and 3, the standardized estimates, their significance, and the proportion of explained variance for each regression model (model 1 with demographic and disease factors and model 2 with psychological factors added) in the two disease groups are provided. Results are presented from the analyses on the imputed datasets. Results from the complete case analyses were similar (data not shown).
As is seen in Table 2, in the CD group (N = 147), female gender and clinical disease activity were significantly associated with HRQOL in the first model, explaining 37% of the variance in HRQOL. After adding the psychological factors, clinical disease activity (ß = − .170, p = .001), more negative illness perceptions (ß = − .412, p < .001), and more depressive symptoms (ß = − .454, p < .001) were associated with lower HRQOL. The second model explained 74% of the variance in HRQOL, with a significant change in explained variance (R2 change = 37%, p < .001).
In the UC/IBD-U group (N = 115), female gender, age, disease duration, and clinical disease activity were significantly associated with HRQOL in the first model, explaining 32% of the variance in HRQOL. After adding the psychological factors, female gender (ß = − .101, p = .022), lower age (ß = − .193, p < .001), shorter disease duration (ß = .087, p = .045), more negative illness perceptions (ß = − .438, p < .001), more anxiety symptoms (ß = − .201, p = .001), and more depressive symptoms (ß = − .279, p < .001) were associated with lower HRQOL. The second model explained 83% of the variance, with a significant change in explained variance (R2 change = 51%, p < .001).
Discussion
This study examined the influence of psychological factors on HRQOL over and above the influence of demographic and disease factors in youth with IBD and analyzed the results separately for CD and UC/IBD-U. Partly in line with our first hypothesis, in the first model, without the psychological factors included, female gender and clinical disease activity were significantly associated with HRQOL, as were age and disease duration only in the UC/IBD-U group. However, when adding a combination of all psychological factors simultaneously in the second model, the influence of demographic and disease factors was reduced. Subsequently, illness perceptions and depression were associated with HRQOL in youth with IBD, even when controlling for demographic and disease factors. More negative illness perceptions and more depression were associated with a lower HRQOL, in both the CD group and the UC/IBD-U group. A difference between the disease groups was that, in the UC/IBD-U group, anxiety was associated with HRQOL as well. Most importantly, adding the psychological factors resulted in a significant increase in the proportion of explained variance, from approximately 35% by the first model to 74–83% by the second model, in both groups. This high proportion of explained variance underlines the importance of psychological factors contributing to HRQOL in patients with IBD.
These results provide insight in which psychological factors play a role in youth with IBD. Consistently in the two disease groups, negative illness perceptions and depression in particular prove their significant role, whereas cognitive coping was not associated with HRQOL. This was also found in previous studies, which reported that illness perceptions and depression were associated with disease outcomes [22, 28]. Therefore, we recommend to pay attention to these factors when treating patients. Our results suggest that in youth with UC/IBD-U, anxiety should be considered as well.
There are several explanations for only finding an association between anxiety and HRQOL in youth with UC/IBD-U. Firstly, the nonsignificant relationship between anxiety and HRQOL in youth with CD cannot be explained by a difference in the prevalence of elevated anxiety symptoms between the CD and UC/IBD-U groups (49.7% versus 50.4%). Secondly, one might postulate that anxiety is not strongly related to HRQOL in youth with IBD. Although we found a high prevalence of anxiety symptoms in the current sample (see Table 1 and [31]), the presence of anxiety symptoms as such may not have to impact the HRQOL of youth with CD. In children and adolescents, the available studies did not show evidence for differences between CD and UC [23], but Sarid et al. [51] showed worse psychosocial outcomes in patients with UC [27, 52]. Thirdly, anxiety and depression are highly comorbid, have overlapping symptoms, and anxiety is considered a precursor of depression [53, 54]. So anxiety may have played a role in preceding depressive symptoms in these patients. It is possible that anxiety and depression both explained variance in HRQOL, but that depression is more strongly related to HRQOL and therefore diminished the relationship between anxiety and HRQOL in the patients with CD. More research is needed to unravel the interplay between anxiety and depression in youth with IBD. In their benchmark review, Cummings et al. [55] describe several pathways for the anxiety and depression comorbidity in children and adolescents. They also stress the importance of studying specific anxiety disorders for their comorbidity with depression. In IBD, very few studies tested specific anxiety problems (e.g., [11]). As a result, to our knowledge, there are no studies that investigated how specific anxiety problems are related to depressive symptoms in patients with IBD. Fourthly, in adults, several studies reported on the relationship between anxiety and HRQOL in both patients with CD and UC [56, 57]. Anxiety might be more impairing for adults with IBD than for youth with IBD, since adults may have to deal with more disease-related anxieties and worries concerning their daily and social functioning (impact of IBD on employment, career perspectives, income, finding a sexual partner, starting a family, etc.). Lastly, anxiety symptoms may be IBD-specific, i.e., anxiety or worries surrounding their IBD symptoms (e.g., bloody stools, the necessity of a stoma or surgery). These worries are often exorbitant to the actual context but can have a negative impact [58, 59]. More specifically, higher IBD-specific anxiety was associated with lower HRQOL in youth with both CD and UC [58]. However, we are not aware of studies that examined differences between CD and UC with respect to IBD-specific anxiety in youth. Perhaps, youth with UC/IBD-U experience different IBD-specific worries than youth with CD, for example, since youth with UC/IBD-U more often have alarming bloody stools than youth with CD.
Although the CSM postulates that coping is an important factor, in our study, cognitive coping was not significantly related to HRQOL, when simultaneously added to the model with the other psychological factors. Cognitive coping may not be related to HRQOL in IBD patients, as was also found in earlier studies examining individual psychological factors [27, 52]. This is in contrast with the results of a review including a wide range of illnesses in adults, which found that coping was a stronger predictor for health outcomes than illness perceptions [60]. Perhaps, coping plays a different role in IBD than in other illnesses. On the other hand, the type of coping may be of importance, since we only tested cognitive coping styles (and not for example behavioral). However, the results of two adult IBD studies including problem-focused and emotion-focused coping are mixed [61, 62] and therefore do not support this explanation completely.
Comparing the results between patients with CD and UC/IBD-U showed differences in the second model: a significant association of clinical disease activity with HRQOL in the CD group and a significant association of gender, age, and disease duration with HRQOL in de UC/IBD-U group. Most likely, these differences cannot be explained by differences between the two groups, since the groups were similar with respect to the percentages of active disease, males versus females and the disease duration (see Table 1). Only in the CD group, clinical disease activity was associated with HRQOL, even after adding the psychological factors to the model. To our knowledge, in youth, no studies have specifically examined differences between CD and UC with respect to the relationship between clinical disease activity and HRQOL. Patients with CD have a more heterogeneous clinical presentation and are affected by growth failure, more often than patients with UC and IBD-U [1]. The heterogeneous clinical presentation and growth failure can lead to a lower HRQOL. A recent review of Knowles et al. [63] showed that HRQOL was significantly lower for patients with active disease, although no information was provided about differences between CD and UC/IBD-U. In children and adolescents with IBD (both CD and UC), some studies have shown that clinical disease activity remained associated with HRQOL, even when anxiety/depression [19, 21, 64] and parental stress [64, 65] were included as mediators. It was therefore not tested, as in our study, what the influence is of demographic, disease, and psychological factors on the relationship between clinical disease activity and HRQOL. It seems that the relationship between clinical disease activity and HRQOL is not a direct relationship as such.
Only in the UC/IBD-U group, gender, age, and disease duration were significantly associated with HRQOL, even after adding the psychological factors to the model. For gender, previous studies in youth with IBD did not find an association with HRQOL [66,67,68]. These studies all included both CD and UC patients, but the majority of youth had CD (> 70%), which may have masked the association between gender and HRQOL in the UC patients. However, it remains unclear what role gender has in affecting HRQOL, especially since gender is associated with more anxiety and depressive symptoms in general [69], as well as in our own cohort [31]. Anxiety and depressive symptoms are known to affect HRQOL in youth with IBD [21, 64]. For age, our results indicated that older age was associated with lower HRQOL in youth with UC/IBD-U. This is accordance with Otley et al. [68], who also reported that older age was associated with lower HRQOL in the first year after diagnosis of IBD. However, in their sample, a large majority of youth was diagnosed with CD (77%). Other studies did not find association between age and HRQOL [30, 70] or the reversed association (lower HRQOL in younger patients; [20]). These mixed findings were confirmed in a review on predictors of HRQOL in youth with IBD [6]. Finally, in our study, a shorter disease duration was associated with a lower HRQOL in youth with UC/IBD-U. Previous studies have suggested that it seems that disease duration is not associated with HRQOL in general, but only within the first months after diagnosis (of both CD and UC/IBD-U) [30, 68]. However, these studies included mainly CD patients (77% and 100%, respectively) [30, 68]. In our sample, only 20% had a disease duration of 6 months or shorter. Therefore, our results suggest that for youth with CD in the first 6 months after the diagnosis, disease duration is not associated with HRQOL. For UC and IBD-U, this relationship is unclear less clear defined. Although these differences between the disease groups are important to notice, the most important finding remains that, overall, in both disease groups, illness perceptions and depression were significantly associated with HRQOL.
Strengths
Our sample (N = 262) is one of the largest European samples and innovative in studying the influence of both disease, demographic, and psychological factors in youth with IBD. Our large sample covers a broad age range, using internationally validated and age-attuned instruments. This age range is an important life phase, as several biological and psychosocial changes take place, and a chronic disease such as IBD can have negative consequences for the transition to adulthood. In addition, our sample was derived from 6 centers (both urban and rural areas), making generalization of our findings stronger. In addition, and contrary to other studies that only included either anxiety or depression (e.g., [8, 11]), we assessed both anxiety and depression, as this had implications for subsequent psychological treatment. Most importantly, whereas previous studies mostly examined individual relationships between disease factors, psychological factors and HRQOL, we aimed to test the influence of disease, demographic, and psychological factors simultaneously. An advantage of this approach is that the current study took into account the interrelationships between all the factors in their associations with HRQOL.
Limitations
The number of patients with active disease (mostly mild clinical disease activity) was low (25%), although this number is often found in population-based cohorts of patients with IBD. It may be that the associations between the psychological variables and HRQOL are not the same for patients that have more active disease. Nevertheless, studies with a higher proportion of patients with active disease reported similar results [6, 21, 64, 65]. However, despite these findings, it is still possible that for patients with moderate to severe clinical disease activity, the relationships between illness perceptions, depression, and HRQOL are different. Since evidence has been found for a negative impact of clinical disease activity on anxiety, depression, and/or HRQOL (e.g., [11, 23]), even stronger relationships may be found in patient populations with more active disease. Another limitation is that our data were cross-sectional and conclusions on causal relationships cannot be drawn. Longitudinal studies are needed to examine causal relationships over time. Until now, only few studies have been conducted that were able to draw conclusion on causal relationships. For example, a recent study in adults with IBD found evidence for a bidirectional and causal relationship between disease activity and anxiety/depression [71]. However, such studies have not been conducted investigating HRQOL. A last limitation is that we had a response rate of approximately 70%, which can have caused bias, for example, if patients with a lower HRQOL were more inclined to participate than those with higher HRQOL. However, we were not able to compare the HRQOL of responders and nonresponders.
Clinical Implications
These results stress the importance of psychological factors for HRQOL in youth with IBD, over and above demographic and disease variables. In our study sample, 75% of the patients were in clinical remission. Therefore, treating (pediatric) gastroenterologists should pay attention to these psychological factors, in all patients and not only in patients with active disease. We recommend screening for negative illness perceptions and internalizing problems. This can be done either during a medical visit or using short (online) questionnaires prior to the medical visit. Our results also have implications for psychological treatment of these patients: interventions for improving HRQOL should focus on negative illness perceptions and depression and also on anxiety for youth with UC/IBD-U. For example, cognitive behavioral therapy (CBT) has been proven effective in using techniques to restructure thoughts, such as negative illness perceptions [72]. Importantly, at the beginning of a psychological intervention disproportionate, unrealistic or incorrect thoughts and ideas should be identified. At this phase, it is important to determine whether a patient has disproportionate or incorrect negative illness perceptions. These can then be crucial when practicing cognitive and behavioral techniques. Naturally, the techniques of CBT can be used to improve depression and anxiety as well [73, 74].
In conclusion, our study found that negative illness perceptions and depression are negatively associated with HRQOL in youth with IBD, even after controlling for several demographic and disease factors, with also other psychological factors (i.e., coping, anxiety) taken into account. These factors seriously influence HRQOL, even in our cohort with low clinical disease activity, and should be considered by the medical team. Our results indicate that, irrespective of the clinical disease activity, psychological treatment should focus on the way these young IBD patients perceive their disease and on their depressive symptoms. For youth with UC and IBD-U, anxiety and worries should receive attention as well.
References
Griffiths AM. Specificities of inflammatory bowel disease in childhood. Best Pract Res Clin Gastroenterol. 2004;18(3):509–23.
Adamiak T, Walkiewicz-Jedrzejczak D, Fish D, Brown C, Tung J, Khan K, et al. Incidence, clinical characteristics, and natural history of pediatric IBD in Wisconsin: a population-based epidemiological study. Inflamm Bowel Dis. 2013;19(6):1218–23. https://doi.org/10.1097/MIB.0b013e318280b13e.
Ghione S, Sarter H, Fumery M, Armengol-Debeir L, Savoye G, Ley D, et al. Dramatic increase in incidence of ulcerative colitis and Crohn’s disease (1988-2011): a population-based study of French adolescents. Am J Gastroenterol. 2018;113(2):265–72. https://doi.org/10.1038/ajg.2017.228.
Rabizadeh S, Dubinsky M. Update in pediatric inflammatory bowel disease. Rheum Dis Clin N Am. 2013;39(4):789–99.
Arnett JJ. Adolescence and emerging adulthood: A cultural approach (international edition). Fourth ed. Upper Saddle River: Prentice Hall; 2010.
Ross SC, Strachan J, Russell RK, Wilson SL. Psychosocial functioning and health-related quality of life in paediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2011;53(5):480–8. https://doi.org/10.1097/MPG.0b013e31822f2c32.
Knowles SR, Graff LA, Wilding H, Hewitt C, Keefer L, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses—part I. Inflamm Bowel Dis. 2018;24(4):742–51.
Clark JG, Srinath AI, Youk AO, Kirshner MA, McCarthy FN, Keljo DJ, et al. Predictors of depression in youth with Crohn disease. J Pediatr Gastroenterol Nutr. 2014;58(5):569–73. https://doi.org/10.1097/MPG.0000000000000277.
Szigethy E, Bujoreanu SI, Youk AO, Weisz J, Benhayon D, Fairclough D, et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J Am Acad Child Adolesc Psychiatry. 2014;53(7):726–35. https://doi.org/10.1016/j.jaac.2014.04.014.
Kilroy S, Nolan E, Sarma KM. Quality of life and level of anxiety in youths with inflammatory bowel disease in Ireland. J Pediatr Gastroenterol Nutr. 2011;53(3):275–9. https://doi.org/10.1097/MPG.0b013e318214c13100005176-201109000-00008.
Reigada LC, Hoogendoorn CJ, Walsh LC, Lai J, Szigethy E, Cohen BH, et al. Anxiety symptoms and disease severity in children and adolescents with Crohn disease. J Pediatr Gastroenterol Nutr. 2015;60(1):30–5.
Stapersma L, van den Brink G, Szigethy EM, Escher JC, Utens E. Systematic review with meta-analysis: anxiety and depression in children and adolescents with inflammatory bowel disease. Aliment Pharmacol Ther. 2018;48(5):496–506. https://doi.org/10.1111/apt.14865.
Diefenbach M, Leventhal H. The common-sense model of illness representation: theoretical and practical considerations. J Soc Distress Homeless. 1996;5(1):11–38. https://doi.org/10.1007/bf02090456.
Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–7.
Monat AE, Lazarus RS (Eds). Stress and coping: an anthology. 1991. New York: Columbia University Press.
Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, Wadsworth ME. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol Bull. 2001;127(1):87–127.
Compas BE, Jaser SS, Bettis AH, Watson KH, Gruhn MA, Dunbar JP, et al. Coping, emotion regulation, and psychopathology in childhood and adolescence: a meta-analysis and narrative review. Psychol Bull. 2017;143(9):939–91. https://doi.org/10.1037/bul0000110.
Garnefski N, Kraaij V. Specificity of relations between adolescents’ cognitive emotion regulation strategies and symptoms of depression and anxiety. Cognit Emot. 2018;32(7):1401–8. https://doi.org/10.1080/02699931.2016.1232698.
Gray WN, Denson LA, Baldassano RN, Hommel KA. Disease activity, behavioral dysfunction, and health-related quality of life in adolescents with inflammatory bowel disease. Inflamm Bowel Dis. 2011;17(7):1581–6. https://doi.org/10.1002/ibd.21520.
Chouliaras G, Margoni D, Dimakou K, Fessatou S, Panayiotou I, Roma-Giannikou E. Disease impact on the quality of life of children with inflammatory bowel disease. World J Gastroenterol. 2017;23(6):1067–75. https://doi.org/10.3748/wjg.v23.i6.1067.
Engelmann G, Erhard D, Petersen M, Parzer P, Schlarb AA, Resch F, et al. Health-related quality of life in adolescents with inflammatory bowel disease depends on disease activity and psychiatric comorbidity. Child Psychiatry Hum Dev. 2015;46(2):300–7.
Rochelle TL, Fidler H. The importance of illness perceptions, quality of life and psychological status in patients with ulcerative colitis and Crohn’s disease. J Health Psychol. 2013;18(7):972–83.
Brooks AJ, Rowse G, Ryder A, Peach EJ, Corfe BM, Lobo AJ. Systematic review: psychological morbidity in young people with inflammatory bowel disease - risk factors and impacts. Aliment Pharmacol Ther. 2016;44(1):3–15.
McCombie AM, Mulder RT, Gearry RB. How IBD patients cope with IBD: a systematic review. J Crohn's Colitis. 2013;7(2):89–106.
van Erp SJH, Brakenhoff LKMP, Vollmann M, van der Heijde D, Veenendaal RA, Fidder HH, et al. Illness perceptions and outcomes in patients with inflammatory bowel disease: is coping a mediator? Int J Behav Med. 2017;24(2):205–14. https://doi.org/10.1007/s12529-016-9599-y.
van Tilburg MA, Claar RL, Romano JM, et al. The role of coping with symptoms in depression and disability: comparison between inflammatory bowel disease and abdominal pain. J Pediatr Gastroenterol Nutr. 2015;61(4):431–6. https://doi.org/10.1097/MPG.0000000000000841.
van der Have M, Minderhoud IM, Kaptein AA, Leenders M, Siersema PD, Fidder HH, et al. Substantial impact of illness perceptions on quality of life in patients with Crohn’s disease. J Crohns Colitis. 2013;7(8):e292–301.
van Tilburg MA, Claar RL, Romano JM, et al. Psychological factors may play an important role in pediatric Crohn’s disease symptoms and disability. J Pediatr. 2017;184:94–100 e1. https://doi.org/10.1016/j.jpeds.2017.01.058.
Katz L, Tripp DA, Ropeleski M, Depew W, Curtis Nickel J, Vanner S, et al. Mechanisms of quality of life and social support in inflammatory bowel disease. J Clin Psychol Med Settings. 2016;23(1):88–98. https://doi.org/10.1007/s10880-015-9431-x.
Hill R, Lewindon P, Muir R, Grangé I, Connor FL, Ee LC, et al. Quality of life in children with Crohn disease. J Pediatr Gastroenterol Nutr. 2010;51(1):35–40. https://doi.org/10.1097/MPG.0b013e3181c2c0ef.
van den Brink G, Stapersma L, Vlug LE, Rizopolous D, Bodelier AG, van Wering H, et al. Clinical disease activity is associated with anxiety and depressive symptoms in adolescents and young adults with inflammatory bowel disease. Aliment Pharmacol Ther. 2018;48(3):358–69. https://doi.org/10.1111/apt.14832.
van den Brink G, Stapersma L, El Marroun H, et al. Effectiveness of disease-specific cognitive-behavioural therapy on depression, anxiety, quality of life and the clinical course of disease in adolescents with inflammatory bowel disease: study protocol of a multicentre randomised controlled trial (HAPPY-IBD). BMJ Open Gastroenterol. 2016;3(1):e000071. https://doi.org/10.1136/bmjgast-2015-000071bmjgast-2015-000071.
Levine A, Koletzko S, Turner D, Escher JC, Cucchiara S, de Ridder L, et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014;58(6):795–806.
Magro F, Gionchetti P, Eliakim R, Ardizzone S, Armuzzi A, Barreiro-de Acosta M, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J Crohns Colitis. 2017;11(6):649–70.
Gomollon F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: part 1: diagnosis and medical management. J Crohns Colitis. 2017;11(1):3–25.
Statistics Netherlands. Standaard Beroepen Classificatie 2010. The Hague: Statistics Netherlands; 2010.
Kappelman MD, Crandall WV, Colletti RB, Goudie A, Leibowitz IH, Duffy L, et al. Short pediatric Crohn’s disease activity index for quality improvement and observational research. Inflamm Bowel Dis. 2011;17(1):112–7.
Turner D, Griffiths AM, Walters TD, Seah T, Markowitz J, Pfefferkorn M, et al. Mathematical weighting of the pediatric Crohn’s disease activity index (PCDAI) and comparison with its other short versions. Inflamm Bowel Dis. 2012;18(1):55–62.
de Raaij EJ, Schröder C, Maissan FJ, Pool JJ, Wittink H. Cross-cultural adaptation and measurement properties of the Brief Illness Perception Questionnaire-Dutch Language Version. Man Ther. 2012;17(4):330–5. https://doi.org/10.1016/j.math.2012.03.001.
Szigethy EM, Youk AO, Benhayon D, Fairclough DL, Newara MC, Kirshner MA, et al. Depression subtypes in pediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2014;58(5):574–81. https://doi.org/10.1097/MPG.0000000000000262.
Garnefski N, Legerstee J, Kraaij V, Van Den Kommer T, Teerds JAN. Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc. 2002;25(6):603–11.
Muris P, Bodden D, Hale W, Birmaher B, Mayer B. SCARED-NL. Handleiding bij de gereviseerde Nederlandse versie van de Screen for Child Anxiety Related Emotional Disorders. Amsterdam: Boom test uitgevers; 2011.
Bodden DHM, Bögels SM, Muris P. The diagnostic utility of the Screen for Child Anxiety Related Emotional Disorders-71 (SCARED-71). Behav Res Ther. 2009;47(5):418–25. https://doi.org/10.1016/j.brat.2009.01.015.
Timbremont B, Braet C, Roelofs J. Handleiding Children’s Depression Inventory (herziene versie). Amsterdam: Pearson Assessment and Information B.V.; 2008.
Van der Does AJW. BDI-II-NL Handleiding. De Nederlandse versie van de Beck Depression Inventory-2nd edition. Lisse: Harcourt Test Publishers; 2002.
Otley A, Smith C, Nicholas D, Munk M, Avolio J, Sherman PM, et al. The IMPACT questionnaire: a valid measure of health-related quality of life in pediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2002;35(4):557–63.
Loonen HJ, Grootenhuis MA, Last BF, RJd H, Bouquet J, Derkx BHF. Measuring quality of life in children with inflammatory bowel disease: the impact-II (NL). Qual Life Res. 2002;11(1):47–56. https://doi.org/10.2307/4038068.
Birimberg-Schwartz L, Zucker DM, Akriv A, Cucchiara S, Cameron FL, Wilson DC, et al. Development and validation of diagnostic criteria for IBD subtypes including IBD-unclassified in children: a multicentre study from the pediatric IBD Porto Group of ESPGHAN. J Crohns Colitis. 2017;11(9):1078–84. https://doi.org/10.1093/ecco-jcc/jjx053.
Turner D, Ruemmele FM, Orlanski-Meyer E, Griffiths AM, de Carpi JM, Bronsky J, et al. Management of paediatric ulcerative colitis, part 1: ambulatory care- an evidence-based guideline from ECCO and ESPGHAN. J Pediatr Gastroenterol Nutr. 2018;67:257–91. https://doi.org/10.1097/MPG.0000000000002035.
White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–99. https://doi.org/10.1002/sim.4067.
Sarid O, Slonim-Nevo V, Schwartz D, et al. Differing relationship of psycho-social variables with active ulcerative colitis or Crohn’s disease. Int J Behav Med. 2018;25(3):341–50. https://doi.org/10.1007/s12529-018-9712-5.
Dorrian A, Dempster M, Adair P. Adjustment to inflammatory bowel disease: the relative influence of illness perceptions and coping. Inflamm Bowel Dis. 2009;15(1):47–55. https://doi.org/10.1002/ibd.20583.
Axelson DA, Birmaher B. Relation between anxiety and depressive disorders in childhood and adolescence. Depress Anxiety. 2001;14(2):67–78. https://doi.org/10.1002/da.1048.
Garber J, Weersing VR. Comorbidity of anxiety and depression in youth: implications for treatment and prevention. Clin Psychol Sci Pract. 2010;17(4):293–306.
Cummings CM, Caporino NE, Kendall PC. Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychol Bull. 2014;140(3):816–45. https://doi.org/10.1037/a0034733.
Iglesias-Rey M, Barreiro-de Acosta M, Caamano-Isorna F, et al. Psychological factors are associated with changes in the health-related quality of life in inflammatory bowel disease. Inflamm Bowel Dis. 2014;20(1):92–102. https://doi.org/10.1097/01.MIB.0000436955.78220.bc.
Luo XP, Mao R, Chen BL, Qiu Y, Zhang SH, He Y, et al. Over-reaching beyond disease activity: the influence of anxiety and medical economic burden on health-related quality of life in patients with inflammatory bowel disease. Patient Prefer Adherence. 2017;11:23–31.
Reigada LC, Moore MT, Martin CF, Kappelman MD. Psychometric evaluation of the IBD-specific anxiety scale: a novel measure of disease-related anxiety for adolescents with IBD. J Pediatr Psychol. 2017.
Reigada LC, Bruzzese JM, Benkov KJ, Levy J, Waxman AR, Petkova E, et al. Illness-specific anxiety: implications for functioning and utilization of medical services in adolescents with inflammatory bowel disease. J Spec Pediatr Nurs. 2011;16(3):207–15. https://doi.org/10.1111/j.1744-6155.2011.00292.x.
Dempster M, Howell D, McCorry NK. Illness perceptions and coping in physical health conditions: a meta-analysis. J Psychosom Res. 2015;79(6):506–13. https://doi.org/10.1016/j.jpsychores.2015.10.006.
Knowles SR, Wilson JL, Connell WR, Kamm MA. Preliminary examination of the relations between disease activity, illness perceptions, coping strategies, and psychological morbidity in Crohn’s disease guided by the common sense model of illness. Inflamm Bowel Dis. 2011;17(12):2551–7. https://doi.org/10.1002/ibd.21650.
Zhang M, Hong L, Zhang T, Lin Y, Zheng S, Zhou X, et al. Illness perceptions and stress: mediators between disease severity and psychological well-being and quality of life among patients with Crohn’s disease. Patient Prefer Adherence. 2016;10:2387–96.
Knowles SR, Keefer L, Wilding H, Hewitt C, Graff LA, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses—part II. Inflamm Bowel Dis. 2018;24(5):966–76.
Reed-Knight B, Lee JL, Greenley RN, Lewis JD, Blount RL. Disease activity does not explain it all: how internalizing symptoms and caregiver depressive symptoms relate to health-related quality of life among youth with inflammatory bowel disease. Inflamm Bowel Dis. 2016;22:963–7.
Gray WN, Boyle SL, Graef DM, Janicke DM, Jolley CD, Denson LA, et al. Health-related quality of life in youth with Crohn disease: role of disease activity and parenting stress. J Pediatr Gastroenterol Nutr. 2015;60(6):749–53.
Kunz JH, Hommel KA, Greenley RN. Health-related quality of life of youth with inflammatory bowel disease: a comparison with published data using the PedsQL 4.0 generic core scales. Inflamm Bowel Dis. 2010;16(6):939–46. https://doi.org/10.1002/ibd.21128.
De Boer M, Grootenhuis M, Derkx B, Last B. Health-related quality of life and psychosocial functioning of adolescents with inflammatory bowel disease. Inflamm Bowel Dis. 2005;11(4):400–6.
Otley AR, Griffiths AM, Hale S, Kugathasan S, Pfefferkorn M, Mezoff A, et al. Health-related quality of life in the first year after a diagnosis of pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2006;12(8):684–91.
Altemus M, Sarvaiya N, Epperson CN. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320–30. https://doi.org/10.1016/j.yfrne.2014.05.004.
Gallo J, Grant A, Otley AR, Orsi M, MacIntyre B, Gauvry S, et al. Do parents and children agree? Quality-of-life assessment of children with inflammatory bowel disease and their parents. J Pediatr Gastroenterol Nutr. 2014;58(4):481–5.
Gracie DJ, Guthrie EA, Hamlin PJ, Ford AC. Bi-directionality of brain-gut interactions in patients with inflammatory bowel disease. Gastroenterology. 2018;154(6):1635–46 e3. https://doi.org/10.1053/j.gastro.2018.01.027.
Christensen SS, Frostholm L, Ornbol E, Schroder A. Changes in illness perceptions mediated the effect of cognitive behavioural therapy in severe functional somatic syndromes. J Psychosom Res. 2015;78(4):363–70.
Weisz JR, Kuppens S, Ng MY, Eckshtain D, Ugueto AM, Vaughn-Coaxum R, et al. What five decades of research tells us about the effects of youth psychological therapy: a multilevel meta-analysis and implications for science and practice. Am Psychol. 2017;72(2):79–117.
Compton SN, March JS, Brent D, Albano AM, Weersing VR, Curry J. Cognitive-behavioral psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. J Am Acad Child Adolesc Psychiatry. 2004;43(8):930–59. https://doi.org/10.1097/01.chi.0000127589.57468.bf.
Acknowledgments
We are very grateful to the patients and their parents that consented and to the participating hospitals and their professionals that included patients: Erasmus Medical Center (coordinating center), Albert Schweitzer Hospital, Maasstad Hospital, Haga Hospital, Amphia Hospital, and Leiden University Medical Center.
Funding
This work is financially supported by Stichting Crohn en Colitis Ulcerosa Fonds Nederland/Maag Lever Darm Stichting, Fonds NutsOhra, Stichting Theia, and Stichting Vrienden van het Sophia.
Author information
Authors and Affiliations
Contributions
EMS, JCE, and EMWJU contributed to design of the study. LS, GB, AGB, HMW, PCWMH, JCE, and EMWJU contributed to enrollment of patients and acquisition of data. LS and JE contributed to analysis of the data. LS, GB, JE, JCE, and EMWJU contributed the interpretation of the results. LS drafted the article. All authors revised the article critically and approved the final version.
Corresponding author
Ethics declarations
Conflict of Interest
This work was supported by the Stichting Vrienden van het Sophia (SSWO, grant number 985 to JCE), the Stichting Crohn en Colitis Ulcerosa Fonds Nederland (grant number 14.307.04 to EMWJU), Fonds NutsOhra (grant number 1303-012 to EMWJU), and Stichting Theia (grant number 2013201 to EMWJU). JCE received financial support from MSD (research support), Janssen (advisory board), and AbbVie (advisory board). EMS received financial support from NIH (grant), Crohn and Colitis Fund America (grant), AbbVie (consultancy), Merck (consultancy), IHOPE Network (consultancy), and royalties for book editing from APPI. For the remaining authors, none were declared.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Research Involving Human Participants and/or Animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Stapersma, L., van den Brink, G., van der Ende, J. et al. Illness Perceptions and Depression Are Associated with Health-Related Quality of Life in Youth with Inflammatory Bowel Disease. Int.J. Behav. Med. 26, 415–426 (2019). https://doi.org/10.1007/s12529-019-09791-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-019-09791-6